
Abstract
Purpose:
Although the health benefits of behavioral interventions for older adults are well studied, research focused on intervention acceptability in older adult populations is less established and is needed. This mixed methods study investigated older adults’ perceptions of training interventions.
Methods:
Community-dwelling older adults (N = 41) were randomized into three groups (cognitive, physical, and exergame) and completed 20 in-lab training sessions over 10 weeks. At every fifth session, participants provided feedback on their perceived gains across functional domains, enjoyment of and motivation to complete training, and aspects they most and least enjoyed regarding study participation.
Results:
Based on the multivariate analysis of variance, perceived cognitive and everyday function gains did not vary by training group. However, physical and exergame groups perceived greater improvement in physical function than the cognitive training group (P < 0.001). Enjoyment of and motivation to complete training did not vary by training group. Exploratory qualitative coding results suggest that participants across groups most enjoyed social interaction and feelings of improvement. Participants least enjoyed traveling to the study site and engaging in aspects of training (e.g., specific games, structure or duration of training).
Conclusion:
These findings highlight the importance of incorporating meaningful social engagement and balancing the challenge of training components with goal attainment when working with older adults, regardless of the intervention type. Future research and practice should consider salient aspects of the participant experience (e.g., social connection, accessible locations or remote options) when designing interventions for older adults.
Introduction
As we embrace the opportunities and challenges of an aging society, expanding research efforts to better support older adult populations is warranted.1,2 Older adults may benefit from behavioral interventions aimed at preserving functional abilities,2,3 although little is known about intervention acceptability and how it may differ across behavioral intervention types. Research evaluating study acceptability and feasibility in this area is emerging4–7 although not within the context of randomized controlled trials consisting of multiple intervention types. In this mixed methods study, we examine in what ways perceptions of training vary by intervention group (i.e., cognitive, physical, exergame) and how these perceptions affect decisions to continue participating in training following study completion.
Although research on older adults’ perceptions of intervention engagement is limited, the following section briefly reviews older adult participants’ experiences in three training intervention types relevant to this study: cognitive, physical, and exergame.
Cognitive training consists of structured activities aimed at improving or maintaining one or more components of cognition (e.g., memory, executive function 8 ). Current literature on older adults’ perceptions of and motivation to complete cognitive training generally focuses on attitudes toward training and their effects on study adherence; common reasons for training include engaging in novel activities and improving cognitive performance. 9 Participants are often optimistic about the intervention and rate cognitive training as being “somewhat effective.”9,10
Physical training often contains cardiovascular, strength, and/or stretching exercises. Studies assessing physical training perceptions in older adults often focus on populations with cognitive impairment, finding that participants enjoy the social and support aspects of physical intervention programs and generally view their engagement in study activities positively.11–13 Researchers have called for additional work to investigate factors that influence participants’ experiences in exercise interventions. 14
There is growing interest in using gaming technology combined with exercise (i.e., exergaming) to improve or maintain older adults’ functional abilities.15,16 Older adults are often motivated to participate in exergaming for their enjoyment, the potential cognitive and physical benefits, and the immediate performance feedback the exergame provides.6,17 Research suggests strong intervention adherence for participants in exergame conditions.18,19
Perceptions of training across intervention types among healthy community-dwelling older adults, to the authors’ knowledge, have not been researched. Accordingly, we explore (1) in what ways perceptions of training vary by intervention group and (2) how perceptions of training affect older adults’ decisions to continue training participation. We hypothesize that participants will perceive the highest gains in the domain most relevant to their intervention (e.g., the cognitive training group will report higher gains in thinking ability than physical function or everyday task performance, and the physical training group will report higher gains in physical function than thinking ability or everyday task performance). We also predict that perceptions of gains across domains, enjoyment, and motivation to complete training will vary by intervention group, because the substance of the training experience differs by intervention.
Methods
We used a convergent mixed methods approach; this design combines quantitative and qualitative data to build a more complete understanding of older adults’ perceptions of training. 20 This study is preregistered through Open Science Framework (osf.io/j2czg). The larger study from which these data were drawn was approved by the University of Alabama Birmingham's Institutional Review Board; preregistration information is available (osf.io/ka5gy).
Sample
We recruited healthy, sedentary community-dwelling older adults (e.g., 65–95 years, no history of heart disease or stroke, no evidence of dementia) with limited physical activity, cognitive training, and videogame experience (<2 hours/week in previous 2 years) from a metropolitan area in the southern United States. Participants were randomly assigned to one of three active intervention groups or a no-contact control as part of a larger study (see Phillips et al. 21 for additional recruitment and study design information). The sample for this study (Table 1) included participants within the cognitive (n = 15), physical (n = 13), and exergame (n = 13) training groups [Mage=71.44 (5.32); 46.34% female; 14.63% non-White].
Sample Characteristics
M, mean; SD, standard deviation.
Procedure
Participants in each training group completed two one-hour sessions corresponding to their intervention assignment each week for a ten-week period (20 sessions in total). All three interventions used three variations of commercially available products that rotated across sessions. At the conclusion of the 5th, 10th, 15th, and 20th sessions, participants provided feedback on their study experiences using a paper worksheet with closed- and open-ended items designed by the study team.
Although the structure and goals of training were similar across interventions, the activities varied by group. Computer-based games for cognitive training—Bird Safari, Jewel Diver, and Road Tour—targeted divided attention, visual perception, and processing speed through Posit Science Corporation’s InSight program. Exercise videos for the physical training intervention consisted of stretching, low-impact aerobics, strength training, and balance training designed for older adults through the Older and Wiser Workout DVD set. Exergame training activities included Xbox 360 Kinect games requiring full body movements, hand–eye coordination, and dancing: Kinect Adventures, Brain and Body Connection, and Just Dance 4.
Measures
At each measurement time point, participants responded to Likert-type and open-ended items. To assess perceived gains in physical, cognitive, and everyday function, participants responded to three items: “On a scale of 1 (little gain) to 5 (high gain), do you feel like you made gains in your physical fitness/thinking ability/ability to carry out daily tasks?” To assess enjoyment and motivation to complete training, participants responded to the following items: “On a scale of 1 (disliked) to 5 (greatly enjoyed), did you enjoy the training program?” and “On a scale of 1 (not motivated) to 5 (highly motivated), how motivated were you to finish the program? Why?” Participants provided written responses to open-ended questions related to elements of the training program they most and least enjoyed.
At their final session, participants responded to a question gauging their interest in continuing participation in training activities: “Are you interested in continuing to participate in the study for an additional 14 weeks? Please circle Yes or No, and indicate the reason for your decision.”
Analytic approach
In our quantitative analysis, we conducted descriptive analyses and an exploratory multivariate analysis of variance (MANOVA) in IBM SPSS Statistics (Version 28). Owing to the small training group sample sizes and the presence of missing data at certain time points, we calculated average ratings for each Likert-type item across the four time points. Analytical assumptions for running the MANOVA (e.g., multivariate normality, independence, homogeneity of covariance), excluding multivariate normality, were met. The Shapiro–Wilk test showed significant departure from normality for average perceived gains in physical function (P = 0.003), enjoyment (P < 0.001), and motivation (P < 0.001). Given our small sample size and recommendations for proceeding when assumptions are violated,22,23 we interpreted MANOVA results using Pillai’s V.
Our qualitative analysis drew on descriptive coding, an approach often used in evaluation, which consists of providing a word or phrase to summarize information expressed through distinct pieces of data.24,25 This approach was appropriate given the structure of our data source (i.e., short written responses) and allowed us to identify topics conveyed through participants’ responses. The first author reviewed responses and developed a protocol with a priori codes. Using this protocol, this author and three additional coders independently assigned a priori and emergent codes to participant responses. The coders then discussed discrepancies in their codes. Initially, all four coders agreed on 68.83% of coded responses, and three of the four researchers were in agreement on 81.03% of coded responses; all coders came to a consensus on the final codes. Using four independent coders and achieving intercoder agreement aided in establishing the trustworthiness of the results.24,26 Researchers were blinded to the participants’ training group until all codes were assigned and agreed upon.
Results
Quantitative feedback
Table 2 presents the results of our descriptive analyses. The multivariate analysis of variance revealed a statistically significant difference in one or more outcomes by training group (Pillai’s V = 0.89, F = 5.66, P < 0.001, η2=0.447). Subsequent univariate analyses suggested statistically significant differences by training group existed only for perceived gains in physical function (F = 16.215, P < 0.001, η2=0.46). There was no significant difference in cognitive function (F = 1.641, P = 0.207, η2=0.80), everyday function (F = 0.561, P = 0.619, η2=0.25), enjoyment of training (F = 1.30, P = 0.878, η2=0.007), or motivation to complete training (F = 0.278, P = 0.759, η2=0.014). Bonferroni post hoc analyses showed that the physical and exergame training groups reported significantly higher perceived gains in physical function than the cognitive training group (P < 0.001 for both groups). Figures 1 and 2 illustrate average ratings over time by training group for each measure.
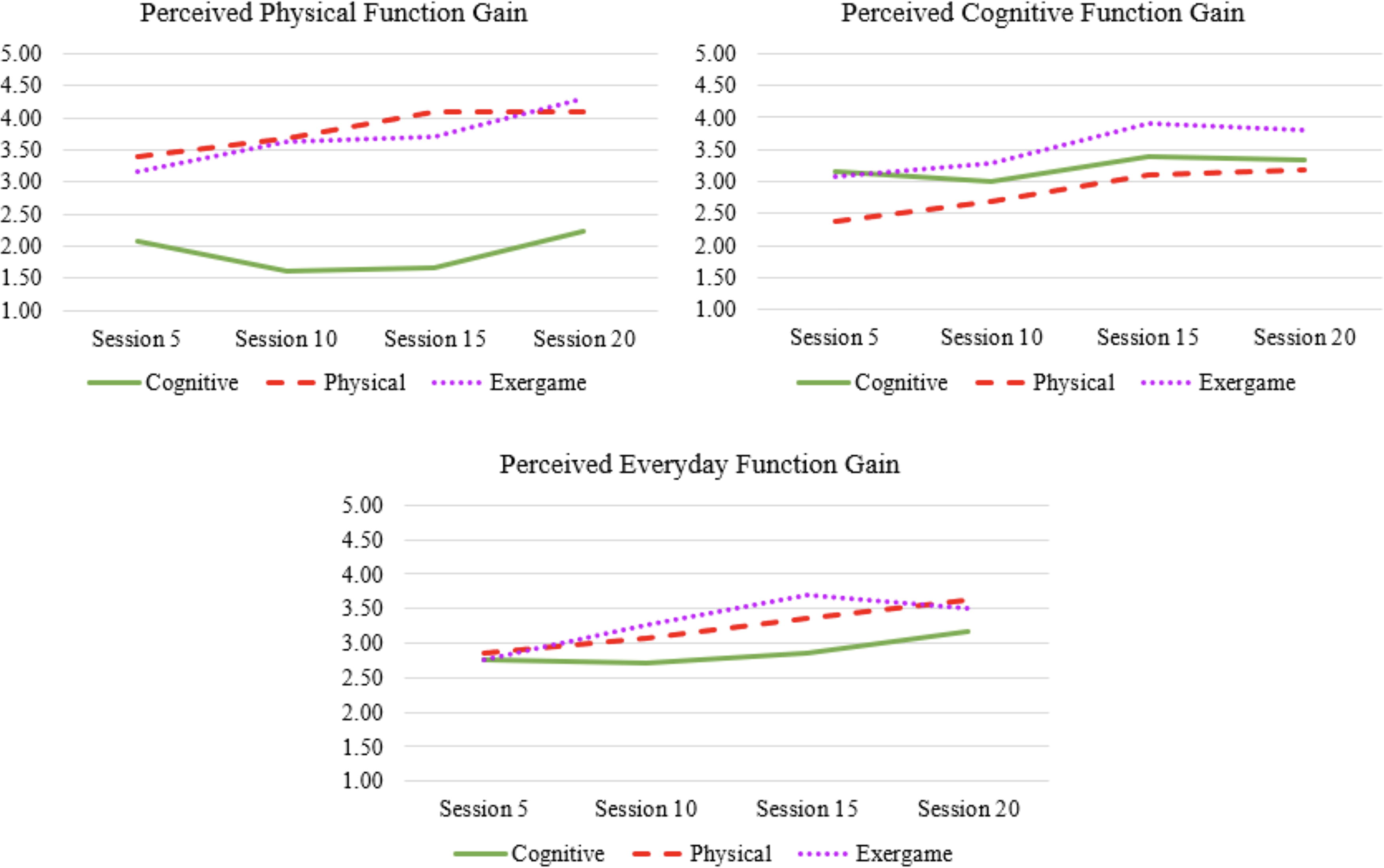
Perceived gains by training group over time.
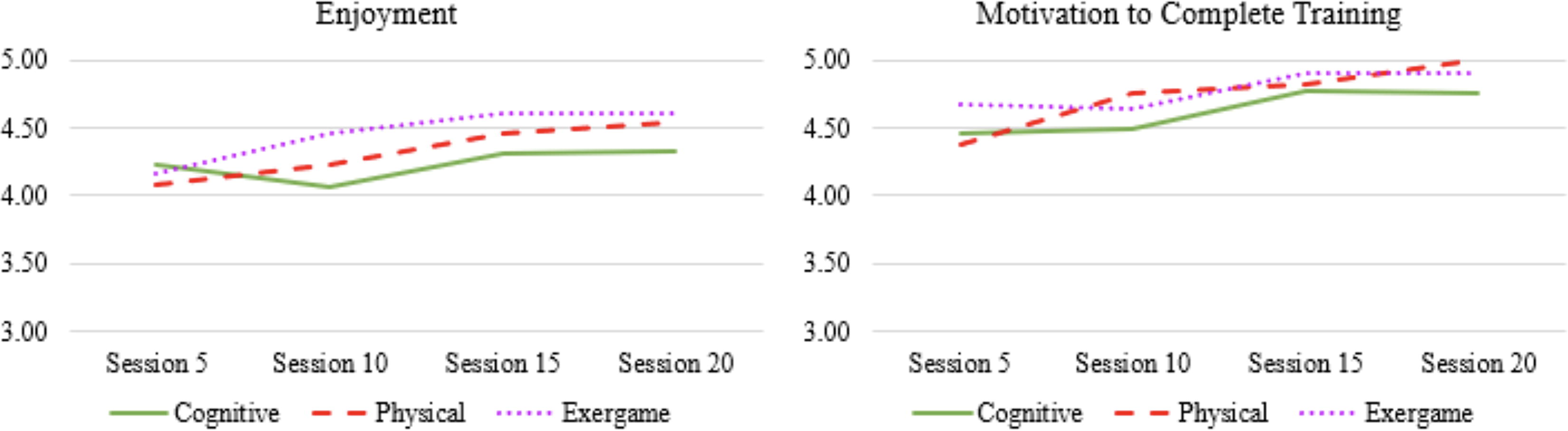
Enjoyment and motivation by training group over time.
Descriptive Statistics
Scales ranged from 1 (no gain/disliked/not motivated) to 5 (high gain/greatly enjoyed/highly motivated).
Qualitative feedback
The following sections present positive and negative aspects of training from participants’ perspectives.
Positive aspects of training
Participants consistently reported enjoying interactions with staff (“great instructor” and “friendliness of the staff”). Participants in the cognitive training group specifically reported enjoying the challenge (“challenge of computer games”) and feelings of improvement associated with training (“seeing progress”; “knowing surely there is some benefit between my ears”; and “ability to be more focused”). Within this group, improvement was cited less frequently at later time points, with only one participant reporting improvement as the most enjoyable aspect by the final session.
Participants in the physical and exergame training groups often enjoyed the exercise component (“strength training,” “dancing,” and “the physical exercise”). For the physical training group, multiple aspects (“all of it” and “I liked it all the same”) and social engagement (“being around other people … laughing and enjoying myself” and “working out with my wife”) were mentioned as other enjoyable aspects. For the exergame training group, other enjoyable aspects included playing games (“Kinect adventures” and “rafting”) and finding value in the training, either for themselves or for a greater purpose (“being a part of research” and “doing something worthwhile”).
Participants’ reasons for continuing with training varied, although the most common across groups was seeing improvement (“helps me to improve my awareness” and “helps to increase my physical strength and mental abilities”). The cognitive training group had the most varied reasons for continuing, with nearly every participant describing different themes (e.g., value, fun, challenge, engagement). For the physical and exergame groups, enjoying exercise and seeing improvement were equally listed as reasons for continuation.
Negative aspects of training
Across training groups, participants least enjoyed traveling to the study location (“driving to the site” and “trip to and from the center”). The cognitive training group held the largest variation in responses across both participants and time points, often citing specific aspects of training they disliked; this included training duration (“watching the computer screen for 55 minutes”), physical positioning during training (“sitting in front of a computer screen”), and feeling bored and frustrated by training tasks (“the monotony” and “frustration at missing so many”).
Exercise was commonly listed as the least enjoyable aspect by the physical and exergame training groups, despite also being cited as one of the most enjoyable aspects. Specifically, participants in the physical training group highlighted disdain for the type of exercise (“cardio,” “wall push-ups,” and “all exercise for the body and none for the mind”) and positions required for completing exercises (“on the floor exercise” or “on the mat”). Meanwhile, participants in the exergame training group listed dancing requirements and specific games as the least enjoyable aspects of their experience.
One-third of participants from the cognitive training group did not want to continue with study participation, and 38.46% from both the physical and exergame training groups chose the same. Across groups, participants cited time constraints (“no time” and “don’t want to commit the time”), along with other commitments/personal obligations, as reasons for not continuing. Across the cognitive and physical training groups, although notably not in the exergame training group, participants cited boredom or redundancy in the training that made them not want to continue (“was interesting at first, but got boring and repetitive”).
Discussion
This study assessed older adults’ acceptability and perceptions of three commercially available interventions. We hypothesized that each training group would perceive the highest functional gains in the domain relevant to their training group and, given differences in the substance of the three interventions, perceptions of training would vary by group. We found that the cognitive training group perceived the highest gains in cognitive function compared with other outcomes, and the physical training group perceived the highest gains in physical function compared with other outcomes. The exergame training group rated their improvement similarly across domains, reporting the highest perceived gains in physical function. Ultimately, our second hypothesis was not supported by the results of the MANOVA, excluding perceived gains in physical function. The physical and exergame training groups perceived higher gains in physical function when compared with the cognitive training group, although differences across other functional domains, enjoyment, and motivation did not differ significantly.
These findings are interesting when considered in light of recent debates surrounding cognitive training. The activities performed by the three training groups differed, yet perceived gains across domains were generally not significantly different by group. Scholars who argue that improvements in cognitive performance emerge as a result of psychological effects (e.g., expectancy, motivation, locus of control) 27 would expect to see the cognitive training group perceive significantly higher gains in cognitive function than the physical and exergame training groups. Instead, our findings support the idea that (a) factors other than assignment into a cognitive training group may be influential in an older adult participants’ perceived improvement in cognitive function or (b) interventions not explicitly focused on cognitive training (e.g., exercise) may elicit similar perceived gains.
Although training interventions varied in substance, the general themes of participants’ training enjoyment responses were similar across groups. For example, participants in each group described traveling to the study site and engaging in specific components of their intervention as the least enjoyable aspects of participation, although the specific components varied by group (e.g., duration for the cognitive training group, required positioning for certain exercises for the physical training group, and dancing for the exergame training group). Disliking the required travel to and from the study location, a large urban downtown area, aligns with past research exploring older adults’ motivations for study participation. 28 When considering the most enjoyable aspects of their experience, participants across groups highlighted the importance of social interaction, especially with study staff. Similar to past studies in this area,4,9,11,17 we found participants also reported that training helped them to build wellness, whether that was gaining confidence, strengthening their cognitive or physical abilities, or feeling that they were contributing to something greater than themselves. Taken together, these findings suggest that the training environment, in addition to individual factors, may be critical in determining intervention acceptability, regardless of the assigned intervention type. 7 Older adults’ desire to participate in research may also play a role in intervention acceptability and/or decisions to continue participation.
Another goal of the study was to assess how perceptions of training affect older adults’ decisions to continue participating in their training intervention. Qualitative results suggest participants who chose not to continue training did so because of time constraints and other commitments; this reflects past work finding that personal and study-related factors are more predictive of study retention than external factors. 7 The transportation difficulties and time commitments highlighted in our findings stress the importance of providing accessible training program options that can be done from home, in nearby community locations, or on a flexible schedule. Participants in our sample who did wish to continue training cited a variety of reasons, with the most common being a sense of improvement, which aligns with research on perceptions of exergame training. 17 With its relevance to user acceptability in technology and its consideration of internal and external conditions impacting use, future work may consider older adults’ research engagement through the lens of the Unified Theory of Acceptance and Use of Technology model.29,30
Limitations of this study include a small sample with limited diversity. The sample was 85.37% white, highly educated (M = 15.85 years of formal education), generally healthy, and located within one metropolitan area. Although we collected data across four time points, the small number of participants limited our ability to conduct meaningful micro-longitudinal analyses and to extrapolate based on the qualitative findings. An additional limitation is the single-item tools used to measure our outcomes. Our emphasis on differences by training group did not allow for an investigation of the complex interplay between our outcomes of interest (e.g., motivation, perceived gains), which may be relevant to our findings; future work should disentangle these relationships and identify their role in older adults’ training perceptions. Future research should draw on the strengths of this study, such as the randomized controlled aspect and mixed methods approach while incorporating a larger, more diverse sample with standardized, multi-item measures exhibiting high validity and reliability to account for a wider range of perspectives and changes over time.
Based on the results of this work and other research in the field, 7 future interventions should consider older adults’ experiences while participating in studies, both in person and virtually. For example, providing remote training options that draw on enhancements in commercially available technology may mitigate feasibility challenges such as travel to study sites and time commitments. 28 Given the consistently high ratings across measures by participants in the exergame training group, future interventions, to the extent possible, should include aspects of exergaming to improve subjective outcomes for older adults involved in research. 6 Future research, programs, and education for older adults should also consider the important role played by facilitators. With participants across groups citing social engagement, and staff specifically, as a consistently enjoyable aspect of their participation, interactive training sessions led by qualified staff should be prioritized.31,32
Conclusions
In this mixed methods study, we explored perceived gains in functional domains, training enjoyment, and motivation to continue in the study for older adults enrolled in a four-armed randomized controlled trial. We found that, generally, perceptions of training, enjoyment of training, and aspects that influenced decisions to continue participation did not vary considerably by training group (i.e., cognitive, physical, exergame). Our findings suggest that factors other than the substantive activities within an intervention (e.g., social engagement, intervention site) may be influential for older adults when making decisions to begin or continue participation in research. Researchers and practitioners should consider the importance of the experience for participants when designing and implementing interventions aimed at improving outcomes for older adults.
Footnotes
Authors’ Contributions
A.T.S.: Conceptualization (equal); methodology (lead); data curation (lead); data analysis (equal); writing—original draft, reviewing, and editing (equal). A.M.: Data analysis (equal); writing—original draft, reviewing, and editing (equal). T.S.: Data analysis (equal) and writing—original draft (supporting). K.C.: Data analysis (equal) and writing—original draft (supporting). C.B.P.: Writing—reviewing and editing (equal). L.A.R.: Conceptualization (equal); funding acquisition (lead); data collection (lead); and writing—reviewing and editing (equal).
Author Disclosure Statement
The authors have no conflict of interests to disclose.
Funding Information
The authors would like to acknowledge funding from the University of Alabama at Birmingham through the Edward Roybal Center for Translational Research on Aging Mobility award from the National Institute on Aging at the National Institutes of Health (