
Abstract
Objective:
Several health games have been developed for pediatric patients in recent years but few for children with atopic dermatitis (AD). As this chronic disease requires changes in daily habits, this study aimed to develop and validate the content of a board health game for children with AD.
Material and Methods:
This is a content development and validation study of DermatrilhaTM, a board health game about AD. The instrument aims to promote interactions between children with AD and health care providers and offers the exchange of experiences, feelings, and knowledge about the disease in a playful way. The five stages of development of the board game were (a) planning, (b) development, (c) preparation of content validation questionnaires, (d) evaluation by a committee of experts, and (e) pretest with the target audience.
Results:
The expert committee group consisted of 20 professionals: 5 physicians specialized in pediatric dermatology, 5 psychologists specialized in health psychology, 5 designers with experience in illustration, and 5 early childhood educators. The target audience consisted of 25 children aged 7–12 years with AD. The evaluation of the expert committee found 0.95 in the general content validity index and 0.92 in the target audience, thus exceeding 0.80 in all items.
Conclusion:
The board health game Dermatrilha has proven to be a psychoeducational tool for the therapeutic education of children with AD, enabling the exchange of experiences, feelings, and knowledge about the disease among peers and health care providers.
Introduction
Despite the recent significant scientific advances in the treatment of atopic dermatitis (AD), adherence to control measures remains a challenge for patients and their families. 1
This inflammatory chronic skin disease with a multifactorial etiology manifests itself clinically with pruritus, recurrent eczema-like lesions, xerosis, and lichenification. 2 It begins in childhood and affects millions of people around the world. 3 AD treatment aims to reduce itching and lesion extent and severity, improve sleep quality, enable daily activities, restore quality of life, maximize disease-free periods, prevent infectious complications, and minimize adverse treatment events. 2 Thus, the adherence of patients and their families to control the disease is essential.
Patients and caregivers have several questions regarding skin care, and the literature describes that lack of knowledge about AD impacts treatment adherence.3–6 Therefore, health education is beneficial for pediatric patients with AD and their caregivers, as it helps them participate and take a leading role in the care of the disease.
Several common questions can be answered through educational practices, for example, understanding the chronic and relapsing nature of AD, knowledge about ways to apply medications, use of moisturizing creams and soaps, products that should be avoided, and treatment of flare-ups.7–9
Therefore, we can see that AD control depends significantly on treatment adherence. This adherence is not just a transfer of knowledge but also a way to impact patients and their families so that they promote a change in health-related behavior.
A widely studied topic, health education aims to involve patients in health care to improve outcomes and treatment quality. Although the importance of including patients in health education practices is increasingly recognized, professionals still face difficulties offering such practices (especially for the pediatric population) because of the complex language used in consultations and decision making (which is made by the parents), affecting children’s acceptance of treatment.9–11 Thus, the use of health games for pediatric patients expands their possibilities to understand and overcome treatment difficulties.12,13
Health games emerged from interdisciplinary and intersectoral projects involving the collaboration of professionals specialized in different areas. The World Health Organization recommends that health professionals try to include the use of games to assist in the treatment of patients, in addition to encouraging research on health games. 14
These games have numerous uses and can be classified into areas of application, for example, promotion, prevention, therapeutic, assessment, education, and rehabilitation. This classification highlights the different ways of working, depending on the demand of the target audience. 15
For example, physical rehabilitation exercises tend to be, often, repetitive and demotivating for patients, which has been one of the causes of treatment abandonment. For this specific demand, a study was conducted using the Nintendo WII® to improve the balance of elderly people. 16 Another study was conducted in the context of palliative care, where it was identified that starting a conversation about certain topics is a difficult task. Thus, a collaborative card game called “Pallium Game” was developed with the aim of assessing and interacting with the multiple needs of individuals and families in palliative and end-of-life situations. 17
Specifically in pediatrics, we can also find several projects for different specialties, including the “Hope Project,” aimed at pediatric cancer patients and developed with the aim of reducing anxiety and increasing physical activity in hospitalized children. 18 Another example is the game, “Heroes of Diabetes,” which aims to teach children how to manage the disease, 19 in addition to the “Hospital Mirim,” which aims to act as a strategy to cope with the invasive procedure of blood collection, reducing the perception of pain. 20 With some examples, we can see that games can be used to aid in treatments in different ways, depending on the needs of the patients.
The literature on pediatric dermatology includes three health games for AD.11,21,22 Considering the scarcity of health games developed in Portuguese (Brazil) for children with AD and the possibility of providing health education in a playful way for these patients, this study aimed to develop and validate the content of a board health game for the pediatric population with AD.
Materials and Methods
This is a study on the development and content validation of a board game for health on AD called DermatrilhaTM. The instrument aims to promote interactions between children with AD and health care providers and the exchange of experiences, feelings, and knowledge about the disease in a playful way.
Content validation can validate instruments. In this study, it was composed of five distinct stages: (a) planning of the board game, (b) development of the board game, (c) elaboration of the content validation questionnaire (CVQ) for a committee of experts and the target audience, (d) evaluation of the expert committee, and (e) pretest with the target audience.
23
Planning the Board Game for Health
A meeting was held with a pediatric dermatology team composed of two preceptors from medical residency services, professors from a Pediatric Dermatology Graduate Program, and six graduate students specializing in pediatric dermatology in which the types of instruments to be developed and the age range of the target audience were defined. Based on this definition, field research was carried out to recognize the existing materials for children in general, for those with chronic diseases, and for the specific group of children with AD. Soon after, a literature review was carried out using the keywords (play therapy) AND (health games) AND (serious games) AND (atopic dermatitis) AND (child development) on PubMed, SciELO, and Capes Portal of Periodicals.
Based on the collected information, it was defined that the instrument would be a board health game for children with AD aged from 7 to 12 years.
Development of the Board Game for Health
In this phase, a meeting was held with the members of the instrument development team: a PhD in child and adolescent health, a psychologist with a master’s degree in child and adolescent health, and a graphic designer with an MBA in project management to define the instrument creation cycles. Interdisciplinary techniques, design thinking, and patient-centered design were used to develop the board game for health.
The content, illustration style, and mechanics of the instrument were initially defined. Brainstorming was used for this, followed by the production of four prototypes that were constantly evaluated by the team.
Production began after the prototypes were defined. For this, fortnightly cycles were defined for the achievement of goals, their analysis and evaluation, and definition of aims for the following cycle, totaling seven cycles.
After the cycles were completed, a version of the board game for health Dermatrilha was developed for evaluation by the committee of experts and the target audience.
Summary of Dermatrilha
Objective: To promote interactions between children with AD and health care providers and provide the exchange of experiences, feelings, and knowledge about the disease in a playful way.
Age group indication: children aged from 7 to 12 years.
Materials: 1 board, 1 avatar, 1 dice, 1 manual, 24 tokens, 6 primers, and 60 cards divided into 20 “it happens to me,” 20 “true or false,” and 20 “question mark” cards (Fig. 1).
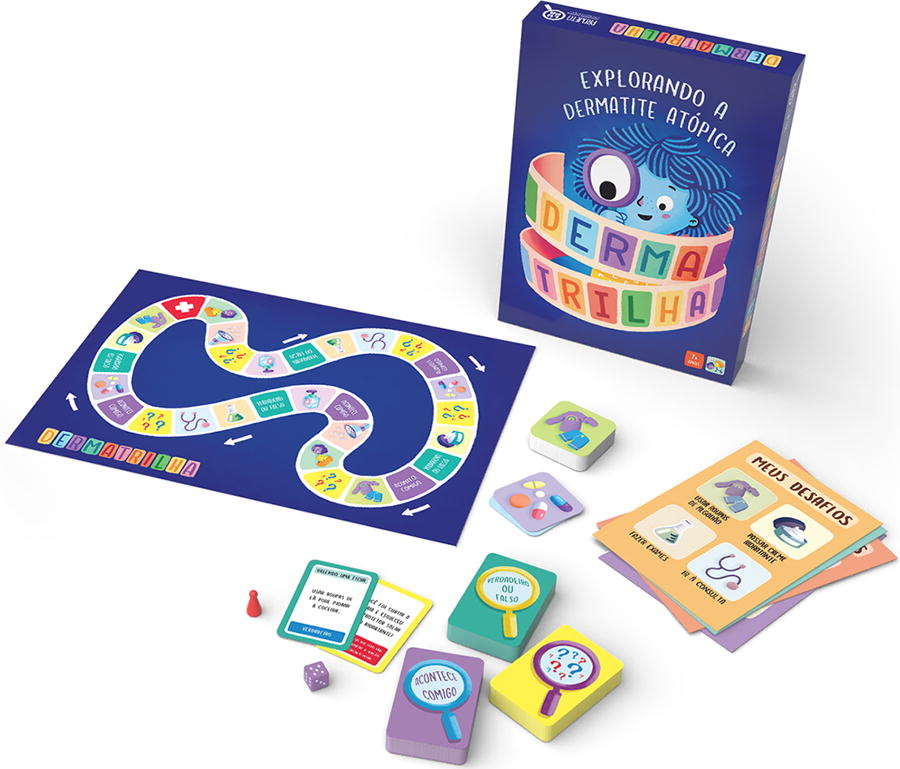
DermatrilhaTM.
The cards contain three main domains as follows:
It Happens to Me: The patient reports and shares their experience with AD with peers, for example, “If you were a physician, how would you take care of children/adolescents who have atopic dermatitis?” “What is the hardest part of treatment for you?” “What do you do when your skin is itchy?” and “What would you say to a child who just found out they have atopic dermatitis?”
True or False: The patient answers whether some sentences about AD are true or false. These cards aim to enable the patient to express their knowledge about the disease and, lacking it, learn it. Some examples of true statements: “to get a good night’s sleep it’d be good to apply plenty of moisturizer before bed” and “children’s liquid soap helps take care of our skin.” Examples of false statements: “a hot bath is very good for those with atopic dermatitis” and “atopic dermatitis is contagious! You can ‘catch’ it from someone else.”
Question Mark: The cards containing the question mark aim to promote interactions that avoid depending on patients’ intended actions. They are either good (positive) or bad luck (negative) cards. Positive cards are actions that favor treatment and advance the patient in the game, whereas negative cards are actions that fail to aid treatment, preventing patients to advance in the game. Example of a positive card: “You taught your friend what atopic dermatitis is. Very good!” An example of a negative card: “You went to enjoy the beach and forgot your sunscreen and moisturizer.”
Development of Content Validation Questionnaires
In total, two content validation questionnaires were elaborated: one for experts (Content Validation Questionnaire for Experts—CVQE) and another for the target audience (Content Validation Questionnaire for the Target Audience—CVTA).
The CVQE was prepared with 21 questions: 20 closed-ended questions about Dermatrilha and 1 open-ended question for comments and suggestions.
The CVTA included 10 questions, namely, 7 closed-ended questions about the game and 3 open-ended questions for the description of interests, learning, comments, and suggestions.
The answers to the closed questions were performed on a 4-point Likert scale, with the answer “no” worth 0 points; “partially,” 1; “yes,” 2; and “I can’t give an opinion,” 3 points.
Expert Committee Assessment
The expert committee consisted of 20 experts, including 5 physicians specialized in pediatric dermatology, 5 psychologists specialized in health psychology, 5 designers with experience in illustration, and 5 educators with at least 5 years of experience in early childhood education. Participants were chosen by a formal email invitation sent to professionals who participate in atopic dermatitis support groups in Brazil, considering their knowledge/ability on the subject.
The CVQE, Dermatrilha, and an explanatory video with two children playing the game were emailed to expert committee members. In their evaluation, the experts were able to suggest modifications to the initial guidelines and format of the instruments, change or reject inappropriate items, and develop new ones.
Pretest with the Target Audience
The target audience consisted of 25 children aged from 7 to 12 years who met the clinical criteria for AD according to Hanifin and Rajka’s 24 classification and were under medical follow-up at the pediatric dermatology service of a tertiary hospital in Brazil.
The target audience evaluation was carried out in person. Each participant was invited to play Dermatrilha and answer the CVTA to assess their understanding, interest, and motivation toward the instrument. These participants could also make changes and suggestions for the game.
The content validity index (CVI) was used to evaluate content validity as it measures the proportion of agreeing judges with the aspects of an instrument, considering a minimum agreement of 0.80. 25 This study was approved by the Human Research Ethics Committee at Clinical Hospital of the Federal University of Paraná, under opinion no. 2063.230/2009-10, and the participants and/or their caregivers signed the assent form and/or the free and informed consent form.
Results
Content validity by the expert committee
The expert committee group consisted of 20 professionals, 90% of whom were female and 10% male. Regarding degrees, 6 (30.0%) were specialists, 11 (55.0%) had master’s degrees, and 3 (15.0%) had PhDs. They resided in the Brazilian municipalities of Curitiba (40.0%), São Paulo (20.0%), Florianópolis (20.0%), Joinville (5.0%), Recife (5.0%), Campo Largo (5.0%), and Santo André (5.0%).
In the expert committee evaluation of the content validity of Dermatrilha, CVI values remained above 0.80 for all items, obtaining a 0.95 total CVI (Table 1).
Content Validity of DermatrilhaTM According to the Expert Committee (n = 20)
AD, atopic dermatitis; E*, educators; GD*, graphic designers; CVI, content validity index; Phy*, physicians; Psy*, psychologists;
The answers to the CVQE open-ended question suggested including two cards on the use of moisturizing cream, modifying the language of one card, and increasing the size of the board.
Content validity by the target audience
The target audience group consisted of 25 children aged from 7 to 12 years, of which 14 were girls and 11 boys residing in the Brazilian municipalities of Curitiba (75.7%), Colombo (9.1%), Pinhais (6.1%), Piraquara (6.1%), and São José dos Pinhais (3.0%). Patients received a diagnosis of AD at a median age of 2 years (interquartile range = 0–6).
In the target audience evaluation of the content validity of Dermatrilha, CVI values remained above 0.80 for all questions, obtaining a 0.92 total CVI (Table 2).
Content Validity Evaluation of DermatrilhaTM by the Target Audience (n = 25)
Regarding the open question “what did you like most about the game?”, 28.0% referred to the “true or false” cards; 24.0%, to “it happens to me” cards; 20.0%, to playing in a group; 12.0%, to the board; 12.0%, to learning about AD care; and 4.0%, to the illustrations.
This study categorized and divided the answers to the open-ended question “what did you learn from the game?” into the following themes: 56.0% answered having learned about the general care of AD; 20.0%, the correct use of clothes; 12.0%, the use of moisturizing creams; and 12.0%, the use of soaps.
Of the 25 children who participated in the health board game evaluation, 84.0% had no suggestions and 16.0% recommended a larger board.
The final version of Dermatrilha incorporated the modification suggestions from both groups.
Discussion
This study validated the content of Dermatrilha, the first board health game for pediatric patients with AD. Few studies have developed and validated instruments for this population. The literature has three digital health games and no board games for this population.
The first digital health game was developed in Brazil in 2011, called “Dermaplay,” and it aimed to assess children’s knowledge about AD before and after using the instrument. The authors found that the children showed increased knowledge after the intervention (before = 68.4%; after = 88.9%). 21 The second game was developed in England in 2022 to relieve the clinical symptoms of AD, especially pruritus, by virtual reality. That pilot study concluded that virtual reality helped relieve symptoms but that the game still required modifications for clinical use. 22 The third game, called the “Shared Decision-Making Game,” was specifically developed for children with moderate and severe AD in Taiwan in 2023 by an interactive PowerPoint platform with educational objectives. The instrument showed an 81.0 content validity score. 11
This study developed an instrument in the format of a board game for use in medical and psychotherapeutic consultations and support groups. Board games are useful tools that are well received by children to achieve the goal of communicating and sharing information in a clear and accessible language. 26 By playing games, children direct their behavior by the meaning the situation provides and engage in activities in which they can assume new identities, explore worlds, and learn by playing.27,28
Thus, board games applied to health can be considered a leisure space for children 26 and a two-way street for interacting with them as professionals can communicate more effectively with them in an understandable language.
Several board games for health have been developed for other pediatric specialties and have shown great results.10,26,29–32
A 2019 systematic review evaluated 11 studies that used board games applied to health to increase educational knowledge. The authors concluded that board games effectively achieve positive outcomes for children’s health. 33
Our results show that Dermatrilha is an instrument with information that improves children’s knowledge about the disease and provides interaction between them and health care providers.
This study carefully planned the development of Dermatrilha to create a game with which all patients could relate. Thus, the informative cards (true or false) address topics that are part of the AD treatment protocol, “it happens to me cards” address patients’ main experiences with the disease, and the “question mark” cards address the main successes and mistakes experienced during treatment in clinical practice.
This study has some limitations, including the age range of its target audience (from 7 to 12 years). As AD is a disease that most often emerges in early childhood, it would be interesting to develop another instrument for the population under seven years of age and the beginning of diagnosis. Another limitation refers to its content validation method, which cross-sectionally evaluated patients’ impressions of Dermatrilha. Longitudinal and before-and-after studies are encouraged to assess the clinical effect of the disease and long-term motivation. However, the instrument proved to be useful and effective for the therapeutic education of children with AD in a playful way, and the members of the expert committee and the target audience groups validated the instrument for clinical use and in support groups.
Conclusion
The expert committee and target audience groups deemed the board game for heath Dermatrilha as valid (0.93 and 0.92 content validity, respectively). This psychoeducational tool on AD offers an alternative to traditional practices.
The possibility of providing health education for pediatric patients in a playful way, contemplating the situations they experience in their daily lives, can contribute to promote health in this population. The development of this type of educational and therapeutic device brings adjuvant forms of treatment for diseases that require constant care and changes in daily routine.
Footnotes
Acknowledgments
We would like to thank all the children and their families who participated in the study, as well as the professionals who participated in the instrument content validation process.
Authors’ Contributions
M.Muzzolon.: writing–original draft. Methodology, Research, Data Collection, and Conceptualization.; M.Morgan.: writing–review and editing.; I.R.: writing–review and editing.; R.I.: writing–review and editing.; V.O.d.C.: writing–original draft. Methodology, Research, Data Collection, Conceptualization.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the University of Parana grant #88887509039/2020-00.