
Abstract
Objective:
The purpose of this study was to (1) quantify the oxygen consumption (VO2) and heart rate (HR) of virtual reality (VR) exergaming in youth, (2) compare the physical activity intensity of VR gaming to moderate-intensity thresholds, and (3) quantify the game experience and cybersickness of VR gaming, compared with traditional gaming.
Material and Methods:
Youth (N = 28; age, 9.4 ± 1.2 years) completed 10-minute conditions: seated rest, seated videogame Katamari Forever (SVG-KF), treadmill walking (TW) (5.6 km/h, 0% grade), and VR exergames Beat Saber (BS) and Thrill of the Fight (TOF) while VO2 and HR were collected. Game experience and Child Simulator Sickness Questionnaires were collected after gameplay.
Results:
VO2 and HR for BS (9.1 ± 3.0 mL/kg/min and 119 ± 15 bpm), TW (17.1 ± 2.4 mL/kg/min and 135 ± 15 bpm), and TOF (16.9 ± 5.4 mL/kg/min and 145 ± 19 bpm) were significantly higher than that at rest (4.2 ± 1.5 mL/kg/min and 94 ± 12 bpm) and for SVG-KF (4.3 ± 1.3 mL/kg/min and 94 ± 12 bpm). BS was light-to-moderate, whereas TW and TOF were of moderate intensity based on HR and metabolic equivalents (METs). For game experience, SVG-KF (1.6 ± 1.6) was less challenging than BS (3.3 ± 1.0) and TOF (3.1 ± 1.1). BS was more visually satisfying (3.5 ± 0.7 vs 2.7 ± 0.9) and required more concentration than SVG-KF (3.6 ± 0.7 vs 3.1 ± 1.1). TOF (3.4 ± 0.8) was more fun than SVG-KF (2.8 ± 0.7). Two youths (7%) experienced cybersickness symptoms, but neither requested to stop play. Oculomotor symptoms (0.6 ± 0.9), although minimal, were significantly greater than nausea (0.2 ± 0.5) and disorientation (0.3 ± 0.6) in both games.
Conclusions:
VR exergames provided light- to moderate-intensity exercise, challenge, visual stimulation, attention, and fun with minimal cybersickness symptoms, compared with conventional gameplay in youth.
Introduction
A large body of evidence supports the benefits of physical activity (PA) on the cognitive function and physical condition of youth.1,2 Despite these benefits, accelerometer data suggested that many children (58%) and adolescents (92%) are insufficiently active to meet the recommended 60 minutes per day of moderate-to-vigorous PA (MVPA). 3 One contributor to low PA among some youth could be the time spent on screen-based sedentary hobbies such as watching television or playing video games. 4
Exergames, also known as active video games, contrast the traditionally sedentary nature of gaming by involving dynamic body movements during gameplay. 5 Movements vary by game and system, but previous research has shown promising results for the ability of exergames to increase PA to intensities greater than rest while providing an enjoyable experience, compared with conventional video games.6–13
Immersive virtual reality (VR) games, a novel form of exergaming, use head-mounted displays (HMD) to provide users with life-like 360-degree point-of-view perspectives, combined with handheld controllers that provide increased movement options compared with some console-based exergames. The audio and visual stimuli provide cognitive distraction that may help to reduce discomfort and negative perceptions in exercise settings 14 and create intrinsic motivation for PA. 15 However, some VR users may experience cybersickness. 14 Some VR users experience cybersickness from using HMDs. Cybersickness includes a collection of symptoms including nausea, visual disturbances, and disorientation that can occur during and after gameplay. 14
The VR Institute of Health and Exercise in partnership with San Francisco State University has produced exercise intensity ratings for many VR games derived from a sample of college-age individuals. 16 Other studies have shown that active VR games are capable of significantly increasing HR and VO2, indicating increased energy expenditure that meets the American College of Sports Medicine (ACSM) threshold for moderate-intensity PA.8,17,18 Few studies have investigated the resulting PA intensity of VR gaming in youth and whether the PA intensity achieved meets the ACSM threshold for moderate intensity.12,15,19 There are limited data about VR sickness symptoms in children.20,21
Therefore, the objectives of this laboratory-based study are: (1) to compare the exercise intensity (oxygen consumption [VO2], heart rate [HR], and rate of perceived exertion [RPE]) among two VR exergaming conditions (Beat Saber [BS], Thrill of the Fight [TOF])—seated rest, a seated videogame (Katamari Forever [SVG-KF]), and brisk treadmill walking (TW) (5.6 km/h) (considered comfortable MVPA walking speed for adolescents) 22 ; (2) to compare VR game intensities with ACSM MPA guidelines and to compare the energy intensity classification of two VR games with that of TW; and (3) to compare game experiences among the three video games and self-reported motion sickness symptoms between VR games in youth aged 8–12 years.
It was hypothesized that VR exergaming has the capacity to reach moderate-intensity PA in youth and that motion sickness symptoms will be nonexistent to mild in most users and not be responsible for any dropouts from the study.
Materials and Methods
Participants
Twenty-eight youth (19 males and 9 females; ages 8–12 years) were recruited to participate in this study from a Boys & Girls Club summer program via word of mouth and posted flyers between the months of May and August (Table 1). Youth were apparently healthy, had no limitations that prevented proper use of study equipment or completing the required activities, and did not report cybersickness symptoms during the VR familiarization session. Youth and their parent/guardian reviewed study requirements, and before participation, written informed consent (parent) and assent (youth) were obtained. Upon completion of the two study visits, youth were compensated for their participation. This study was approved by the university’s Institutional Review Board.
Participants’ Characteristics (Mean ± SD and %)
Classified as healthy weight, overweight, and obese according to Centers for Disease Control and Prevention Growth Charts using participants’ sex, age, height, and weight.
Procedure and instrumentation
Participants completed two visits separated by >48 hours. During the first visit, participants completed questionnaires about demographics, habitual videogame play, and PA. A Tanita BF-350 Total Body Composition Analyzer (Arlinton Heights, IL, USA) measured participants’ body mass and composition via bioelectrical impedance analysis. Standing and seated height were recorded using a Seca 213 portable stadiometer (Hanover, MD, USA). Body mass index (BMI) for each participant was calculated, and weight categorizations were assigned according to Centers for Disease Control and Prevention (CDC) Growth Chart guidelines using the participant’s sex, age, height, and weight. 23 Participants were fitted with a chest-worn Polar H7 HR monitor (Kempele, Finland) and face mask connected via tubing to a metabolic gas analysis system (GA 200, iWorx Systems Inc., Dover, NH, USA). Breath-by-breath measures of VO2 and HR were recorded at rest while participants sat quietly for 10 minutes.
Following the resting VO2 and HR measurements, participants engaged in a familiarization session that involved instruction, demonstration, and practice playing the SVG-KF (BNE Entertainment) on a Sony PlayStation 3 (San Mateo, CA, USA), BS (Beat Games) and TOF (Sealost Interactive LLC) played on a Meta Quest 2 (Menlo Park, CA, USA) VR headset, and walking (5.6 km/h and 0% grade) on a ProForm Sport 5.5 treadmill (Logan, UT, USA) for 3 minutes each. Each activity was completed without the face mask connected via tubing to a metabolic gas analysis system, followed by 2 minutes each while wearing the face mask for breath-by-breath measures of VO2. BS requires players to perform upper-body movements to avoid obstacles and destroy oncoming shapes according to the rhythm of a song. BS was set to “no-fail” to allow for continuous play of the song Crab Rave by Noisestorm (125 bpm pacing). TOF is a semirealistic boxing simulator that requires players to punch, block, and dodge against an opponent during two consecutive 5-minute rounds. The opponents of TOF are named individually and these opponents scale in difficulty. Participants fought against a beginner-level opponent, Melky, as he is the first selectable opponent proceeding the in-game tutorial opponent.
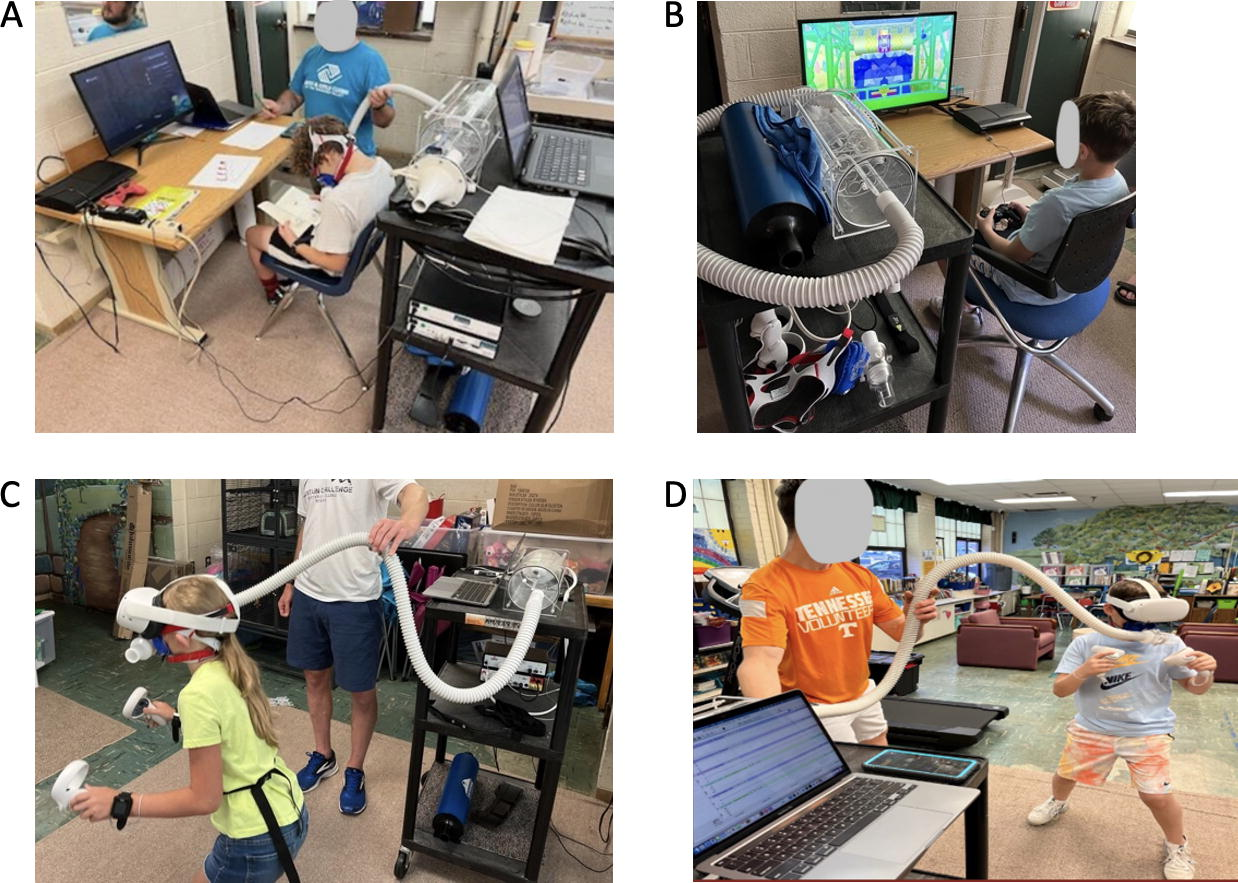
During the second visit, participants were fitted with the face mask and HR monitor to measure VO2 and HR continuously, and they completed five 10-minute conditions in the following order: seated rest, SVG-KF, TW (5.6 km/h, 0% grade), and VR exergames BS and TOF (Fig. 1).7,8 At minutes 4 and 8 of each activity, youth reported their perceived exertion on the Children’s 10-degree OMNI Scale.8,24 Between each condition, participants rested for 5 minutes and responded to the modified Game Experience Questionnaire, to assess how they felt while playing videogames, and to the Child Simulator Sickness Questionnaire 20 following each VR gameplay bout, to measure the presence of cybersickness symptoms.
Steady-state VO2 and HR values between 4 and 8 minutes and RPE between 4 and 8 minutes of each condition were averaged for analysis. Based on ACSM guidelines, the following criteria were used to categorize the exercise intensity of conditions: for light intensity: 1.8–3.94 METs, 30–39.9% of heart rate reserve (HRR), and 2–3.9 RPE; moderate intensity: 3.95–5.69 METs, 40–59.9% of HRR, and 4–6.9 RPE; and vigorous intensity: >5.7 METs, >60% of HRR, and >7 RPE.
Statistical analyses were conducted using IBM SPSS Statistics (version 28; SPSS, Inc., Armonk, NY). Data were checked for assumptions required to run parametric tests. Separate repeated measures analysis of variance (ANOVA) with Bonferroni post hoc tests, compared average VO2, HR, and RPE among the five conditions, the Game Experience Questionnaire scores among the three videogame conditions, and cybersickness symptoms: nausea, oculomotor symptoms, and disorientation between and within VR games. For all tests, P ≤ 0.05 was used to indicate statistical significance.
Results
Participant characteristics and frequency of videogame play and PA are reported in Table 1. Approximately 57% were classified as healthy weight, 11% as overweight, and 32% as obese according to CDC Growth Charts, which use participants’ sex, age, height, and weight. 23 ANOVA tests indicated no between-group differences in VO2, HR, or RPE for any condition; therefore, data were pooled from all weight classifications. Almost a quarter of respondents (21.4% each) reported that their typical duration of video play bout was between 0 and 30 minutes, 30 and 1 hour, and 2 and 3 hours per day. Seventeen participants (60.7%) had previous gaming experience with VR HMDs, mainly the Meta Quest 1 or 2 HMD (50% of all participants). All participants replied “yes” to the question, “Do you think exercise is important?”, and 42.9% of participants exercised between 30 and 60 minutes per bout.
In all three active conditions (BS [119 ± 15 bpm], TW [135 ± 15 bpm], and TOF [145 ± 19 bpm]), HR values were significantly higher than that at rest (94 ± 12 bpm) and for SVG-KF (94 ± 12 bpm) (P < 0.001); rest and SVG-KF were not different from each other. BS HR values were significantly greater than rest and SVG-KF HR values but were significantly less than TW or TOF HR values (P < 0.001) (Fig. 2).

Difference in average heart rate
In all three active conditions (BS [9.1 ± 3.0 mL/kg/min or 2.6 ± 0.8 METs], TW [17.1 ± 2.4 mL/kg/min or 4.8 ± 0.7 METs], and TOF [16.9 ± 5.4 mL/kg/min or 4.8 ± 1.5 METs]), VO2 values were significantly higher than that at rest (4.2 ± 1.5 mL/kg/min or 1.2 ± 0.4 METs) and for SVG-KF (4.3 ± 1.3 mL/kg/min 1.2 ± 0.4 METs) (P < 0.001). Rest and SVG-KF were not different from each other. BS VO2 values were significantly different (P < 0.001) from all other conditions’ VO2 values (Fig. 2).
RPE values of BS (4.1 ± 2.7), TW (4.2 ± 2.0), TOF (6.0 ± 2.4), SVG-KF (0.9 ± 0.8), and rest (0.4 ± 0.6) were significantly different from each other (P < 0.05), with the exception of TW and BS that were not different from each other (Fig. 3).

Difference in average self-reported rate of perceived exertion (RPE) scores among rest, SVG-KF, BS, treadmill walking, and TOF. A = Significantly different from all other conditions; B = significantly different from all other conditions except treadmill; C = significantly different from all other conditions except BS.
Based on METs, BS was classified as light intensity (2.6 ± 0.8 METs), whereas TW (4.9 ± 0.7 METs) and TOF (4.8 ± 1.5 METs) were classified as moderate intensity. A total of 7%, 89%, and 75% of participants, respectively, obtained above the moderate-intensity threshold for METs while playing BS. Based on %HRR, BS (23 ± 11%) was classified as light intensity, TW (39 ± 11%) as light-to-moderate intensity, and TOF (47 ± 18%) as moderate intensity. During TOF, 11%, 39%, and 61% of participants, respectively, obtained above the moderate-intensity threshold for HRR%. %HRR was significantly greater for TW and TOF than for other conditions (P < 0.05). BS was significantly greater than SVG-KF (0 ± 4%) and rest (0 ± 0%) (P < 0.05). Based on RPE, BS (4.1 ± 2.7) and TW (4.2 ± 2.0) were classified as light-to-moderate intensity, and TOF (6.0 ± 2.4) was classified as moderate-to-vigorous intensity; 57%, 50%, and 86% of participants, respectively, obtained above the moderate-intensity threshold for RPE (Fig. 4).

95% confidence intervals and activity intensity classification of BS, treadmill walking, and TOF based on ACSM guidelines
For game experience, youth reported SVG-KF (1.6 ± 1.6) was less challenging than BS (3.3 ± 1.0) and TOF (3.1 ± 1.1; P < 0.05). BS was more visually satisfying (3.5 ± 0.7 vs 2.7 ± 0.9; P < 0.05) and required more concentration than SVG-KF (3.6 ± 0.7 vs 3.1 ± 1.1; P < 0.05). TOF (3.4 ± 0.8) was more fun than SVG-KF (2.8 ± 0.7; P < 0.05), but there were no significant differences in the happiness, enjoyment, or boredom parameters among the three games (Table 2).
Differences in Game Experience Among Video Games
Scores ranged from 0 to 4, with 0 being the lowest score and 4 being the highest score, except for boredom, which was reverse coded (0 = extremely boring and 4 = not boring at all). A = Significantly different TOF versus SVG-KF; B = significantly different all; C = significantly different BS versus SVG-KF; D = significantly different SVG-KF and TOF versus BS; E = significantly different BS and TOF versus SVG-KF.
Two youths (7%) experienced disorientation or oculomotor symptoms, but neither requested to stop play. Oculomotor symptoms (0.6 ± 0.9) were significantly greater than nausea (0.2 ± 0.5) and disorientation (0.3 ± 0.6) in both games (P < 0.05), with no differences between games. Oculomotor symptoms were the most reported (4% and 4%), followed by disorientation (4% and 0%) and nausea (0% and 0%) for BS and TOF, respectively.
Discussion
The current study measured a variety of physiological data and gameplay experience measures during four different activities (resting, seated video gaming, TW, and BS and TOF VR gaming) in youths aged 8–12 years. Both HMD VR exergames (BS and TOF) increased VO2, HR, and RPE than rest and SVG-KF. In addition, the game type influenced whether VO2, HR, and RPE matched TW. TOF was consistently categorized as moderate intensity based on METs, %HRR, and RPE, and values were equivalent to or greater than the moderate-intensity TW condition. BS was classified as light intensity based on METs and %HRR and as moderate intensity based on RPE. To our knowledge, this is one of the first studies to compare the energy expenditure of HMD VR exergames in youth.
Our findings of increased energy expenditure are supported by previous studies on a variety of populations (children through adults) using a range of TV screen-based gaming consoles and VR exergames using HMD (Nintendo Wii®, Sony Playstation Move®, and Microsoft XBOX Kinect®, HTC VIVE®).6–12,15,25 Gomez et al. 8 found that TOF provided the highest average VO2 value (32.5 ± 7.1 mL/kg/min), the highest average HR (149 ± 16 bpm), and the highest average Borg 6–20 RPE score (12.7 ± 0.4), and it was categorized as the most vigorous activity based on METs, compared with two other VR exergames: Holopoint (24.8 ± 6.6 mL/kg/min) and Audioshield (19.1 ± 5.9 mL/kg/min) in a sample of 41 adults (ages 18–39). Sanders et al. 7 found that the mean HR of Kinect Boxing (126.4 ± 3.0 bpm) was significantly higher (P < 0.001) than that of TW (103.3 ± 2.0 bpm) and Wii Boxing (104.5 ± 2.2) in a sample of 27 college students. Despite having a significantly higher HR and RPE, Kinect Boxing was preferred to Wii Boxing and TW. 7 In the current study, TOF yielded the highest average HR and RPE scores of the three conditions, and it also had the highest “fun” score on the Game Experience Questionnaire. Boxing simulation games consistently produce the highest intensity of activity compared with other active games, regardless of the gaming device.7,8 Audioshield and BS are both rhythm games that require upper-body leaning or ducking movements to avoid obstacles. But without much engagement of the lower body, their ability to produce vigorous-intensity PA may be limited. 8
VR exergame design (programmed controller movements, gameplay–space integration, locomotion, etc.) has an influence on the PA intensity.
Unlike TW and TOF gameplay, BS was unable to consistently elicit moderate-intensity PA under the conditions of this study. BS offers a variety of songs with different difficulty settings and multiple gameplay modifiers. Songs with higher total beats would require more swings, higher tempos would require faster swings, and additional obstacles would require more total body movement to avoid. Future research is needed to examine physiological responses to playing BS under different in-game parameters. Another area for future research would be further exploration of whether physiological responses differ by weight classification. Although we did not see any differences between weight categories in our outcome variables, we had unequal numbers of participants in each weight category. Future studies could either limit inclusion criteria to one weight category or stratify recruitment to have an equal distribution of participants from the different weight categories.
Our sample of youths found TOF significantly more fun, challenging, and physically intense, and BS to be more visually satisfying than the SVG-KF. Polechonski et al. 15 found that 91% of the 11 adolescents found that VR games played on an OMNI omnidirectional treadmill were more fun than normal computer games, and 73% would be willing to replace traditional video games with VR exergames. Similarly, Sousa et al. 26 found that 29 college-age adults preferred the VR exergame BS, finding it more immersive, challenging, and overall positive than the sedentary VR game Thumper. Some previous studies support that enjoyment of PA in a virtual environment promotes engaging in activity longer and more frequently.27,28
An estimated 16% of VR users stop playing because of cybersickness symptoms (nausea, disorientation, and oculomotor disturbances). 14 But symptoms can be avoided/reduced by taking frequent breaks. 29 Dropout rates because of cybersickness symptoms in an adult study were small, and symptoms were reported less frequently in 10-minute versus 50-minute gaming sessions. 14 Neither BS nor TOF yielded a high presence of cybersickness in the adolescent population of this study, so that aspect of VR exergaming did not appear to be a barrier to users of the HMD VR games among our participants. Similarly, Sousa et al. 26 found the presence of motion sickness was very low after 29 college-age students finished a 20-minute session of BS (0.89 ± 1.29).
One-third of the youths in this study (32%) owned a VR headset, and most (60%) reported previous experience using one, namely, a Meta Quest 1 or 2 (46%), in the past. The prevalence of this model’s use and the current popularity of video games among the youth support the feasibility of using VR exergaming as an intervention for increasing PA among children. 30 This study does not advocate for VR exergaming to replace traditional methods of PA, such as free play, outdoor time, and sport participation. However, the results of this study suggest that it has potential as an opportunity to increase PA for some sedentary youths. VR gaming could be a way to combine the current popularity of video games with moderate PA for youths interested in video games.
Conclusions
In conclusion, the selected VR exergames show promising capabilities to provide PA at an intensity that meets ACSM guidelines for health benefits. VR exergames with a greater focus on full-body movement and specific motions to activate a variety of large muscle groups may be worth exploring as exercise interventions. Although the participants of this study experienced little cybersickness, precautions should be taken when playing, and VR exergaming should not be the only method that children and youth obtain use to exercise because of the potential benefits associated with outdoor play and social interaction with peers during activity.
Footnotes
Authors’ Contributions
C.A.G.: conceptualization (lead), methodology (supporting), writing—original draft (lead), and writing—review and editing (equal). J.F.O.: conceptualization (supporting), methodology (supporting), supervision (supporting), and writing—review and editing (equal). S.A.C.: conceptualization (supporting), methodology (supporting), resources (lead), and writing—review and editing (equal). J.A.S.: conceptualization (lead), methodology (lead), formal analysis (lead), supervision (lead), writing—original draft (supporting), and writing—review and editing (equal).
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
This research project was funded by the