
Abstract
Objective:
The present study was conducted to evaluate the effects of video-based exercises added to conventional physiotherapy (CPT) on upper extremity functionality, selective motor control, and proprioception in individuals with unilateral cerebral palsy (UCP).
Materials and Methods:
Thirty patients with UCP were randomized into two groups: the intervention group (15 individuals with a mean age of 9.2 ± 3.8 years) and the control group (15 individuals with a mean age of 8.3 ± 4.1 years). The intervention group received 8 weeks of video-based exercises, and the control group received 8 weeks of conventional physiotherapy. Upper extremity functional abilities, upper extremity selective motor control, proprioception, and entertainment levels were evaluated before and after the intervention for all groups.
Results:
While a significant change was observed in the mean scores of the ABILHAND-Kids, Selective Control of the Upper Extremity Scale right-left scores, shoulder flexion, shoulder abduction, and elbow flexion proprioception angles after the video-based exercises in the intervention group (P < 0.05), a significant change was observed only in the 60-degree flexion angle in the control group (P = 0.001). In the comparison between the groups, there were significant differences in post-intervention value only in shoulder flexion and abduction angles, whereas there was no difference between the groups in elbow flexion angles (P > 0.05).
Conclusion:
Incorporating video-based exercises into the upper extremity rehabilitation processes of individuals with UCP is beneficial in terms of upper extremity functionality, selective motor control, and proprioception.
Introduction
Cerebral palsy (CP) is a motor dysfunction characterized by motor function limitations, postural development problems, and problems in body structure and functions because of congenital or early postnatal brain damage.1,2 Although the findings seen in CP vary depending on the affected central nervous system area, the size of the defect, and the time elapsed after the defect formation, it causes various negative effects on physical functions and the motor system. 3 Negative effects on the motor system negatively affect upper extremity functions such as grasping, object manipulation, and reaching in the majority of individuals with CP. 4 Functional disorders seen in the upper extremity cause negative effects on functional independence, participation, and quality of life. 5 In addition to the mentioned motor function losses, selective motor control (SMC) losses are more common and cause more negative effects on motor functions.6,7 Owing to the impact of SMC abilities, control of independent movements in the joints is achieved. 8 Various findings are observed, such as a decrease in the active range of motion and the emergence of mirror movements in certain body segments, owing to the impact of SMC abilities. 9 In addition to these physical and motor system findings, somatosensory dysfunctions are also commonly observed. 10 It is known that this situation also negatively affects proprioception abilities, and it is emphasized that proprioception should be included in evaluation and treatment programs because of its significant effects on movement and motor function. 11
Health care professionals working with individuals with CP apply various interventions in rehabilitation, focusing on reducing these disorders or maintaining/improving their current functional status. 12 As the rehabilitation process can be continuous and tiring for children with CP, negative periods such as decreased motivation to continue rehabilitation and boredom may occur. 12 It is recommended to implement complementary methods that can attract their attention by making the rehabilitation processes more enjoyable. 13 One of these methods is video-based exercises. In recent years, with the integration of technology into rehabilitation processes, there has been an increasing interest in video-based exercises in CP rehabilitation.14,15 Factors such as providing a meaningful learning experience by providing frequent repetition, encouragement, and motivation during rehabilitation have also been effective in the spread of video-based exercises. 16
In previous studies, it has been stated that video-based exercises improve upper extremity grip strength and motor abilities17,18 and have significant effects on balance, motor functions, speed, and agility. 19 A systematic review emphasized that the video-based interventions in upper extremity rehabilitation in CP higher quality are needed. 20
To the best of our knowledge, it can be said that the number of randomized controlled trials examining the effects of video-based exercises on the upper extremity in individuals with CP is low, and the effects of video-based exercises on upper extremity selective motor control and proprioception in unilateral cerebral palsy (UCP) have not been examined. To fill this gap in the field, this study was planned to examine the effects of video-based exercises on upper extremity functionality, selective motor control, and proprioception in individuals with UCP.
Materials and Methods
Participants
Thirty individuals with UCP, between the ages of 4 and 18, who had Gross Motor Function Classification System (GMFCS) and Manual Ability Classification System (MACS) levels I, II, and III, and who could follow verbal statements, were included in this study. Fifteen individuals were allocated to the intervention group, and 15 individuals were allocated to the control group. Individuals with UCP who did not volunteer to participate in the study and who had undergone upper extremity/spine surgery or Botulinum toxin in the last 6 months were not included in the study.
The distribution of the individuals with UCP into two groups was carried out by the simple random sampling method (closed envelope method) before the baseline evaluations. The randomization process was done by a different physiotherapist, not by the researcher who applied the evaluations. The flow diagram of the individuals included in the study is shown in Figure 1. This study was conducted following the Principles of the Declaration of Helsinki. The study protocol was registered in ClinicalTrials.gov (Identifier: NCT05846542). The study was ethically approved by Gaziantep Islam Science and Technology University’s Non-Interventional Research Ethics Committee (Protocol Number: 2023/203). Informed written consent forms were obtained from all individuals and their families participating in the study. Data were collected from a special education and rehabilitation center between April and October 2023.
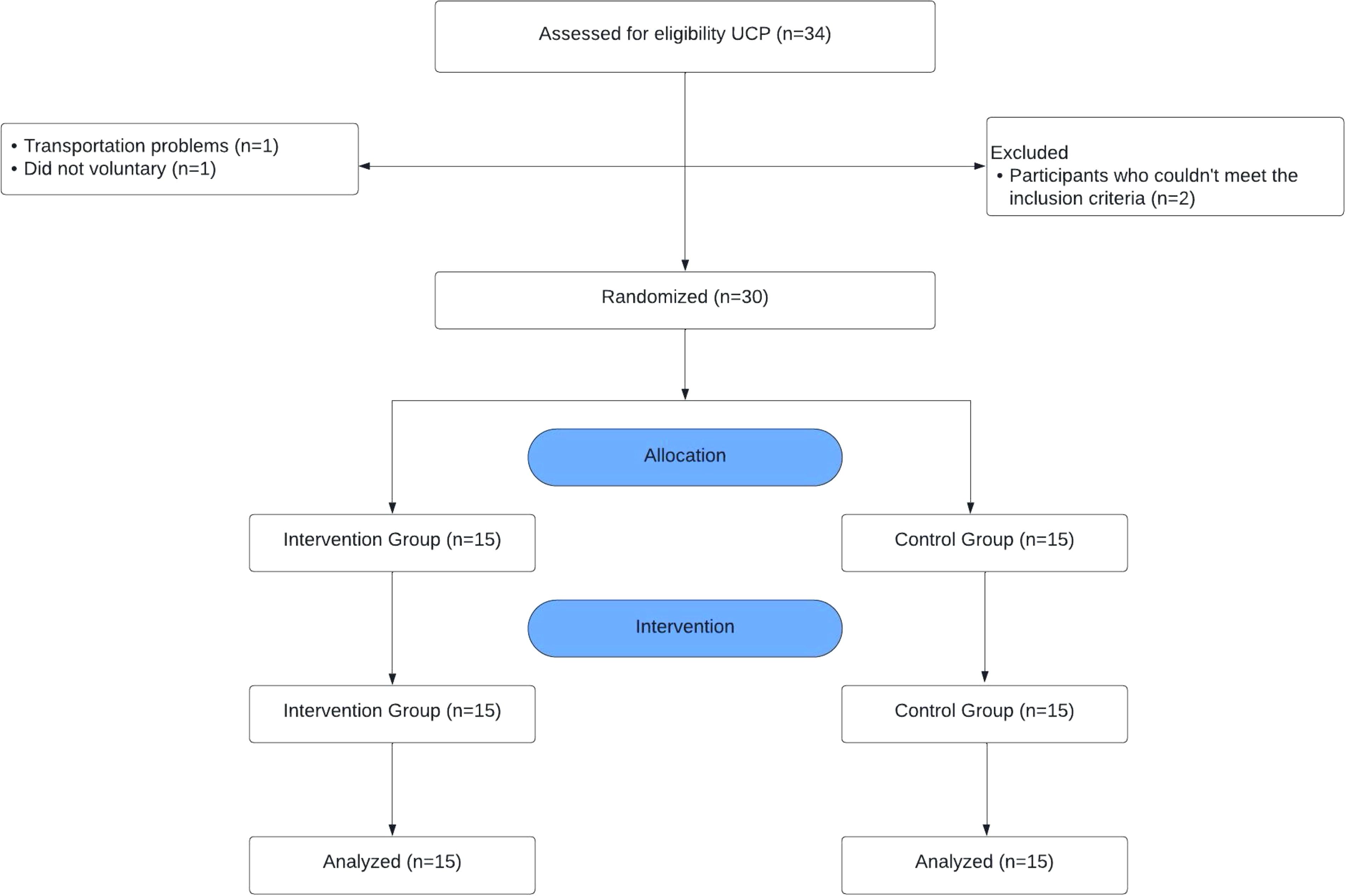
Flowchart.
Study design and interventions
This study is in the form of a single-blind (the statistician in the study was blind), randomized, controlled trial. Among the children with UCP who met the inclusion criteria between the dates of the research, they were divided into two groups by the sealed envelope randomization method.
The UCP intervention group underwent 15-minute pre-game warm-up (breathing exercises and muscle preparation) and post-game cool-down (breathing exercises and free joint mobility) periods, 2 sessions per week for 8 consecutive weeks, and 30 minutes of video-based exercise interventions (16 sessions in total). Individuals in the UCP control group received conventional physiotherapy training within a certain program for 45 minutes, twice a week for 8 consecutive weeks (16 sessions in total). Conventional physiotherapy training included weight bearing, upper extremity strengthening, and daily living activities. All evaluations were applied to individuals in both groups twice, before and after the intervention. Video-based exercise and conventional physiotherapy interventions were used for all UCP individuals one-on-one, by the same physiotherapist who is an expert in the field, at the special education and rehabilitation center. Video-based exercises were performed on a 55-inch television screen. Video-based exercises were applied in a 15 m2 room with the Xbox Kinect 3600 (Microsoft, Washington, USA) device. For the interventions, the infrared camera sensor of the Xbox 3600 Kinect device was positioned, and the participant was asked to stand approximately 1.5–2 m away from the screen. Within the scope of video-based exercise interventions, different styles of video-based games involving upper extremity movements were determined and executed for individuals.
Video-based games
It consisted of boxing, tennis, bowling, and golf. These games included upper extremity functional movements focused on the elbow and shoulder. 17
In the boxing game, individuals tried to gain points by punching a designated target within a certain time by controlling the boxing gloves they saw on the screen from a first-person perspective. The targets are at different angles and heights.
In tennis, individuals try to score by playing a tennis match on the court they see on the screen. In the bowling game, the participants tried to score points by trying to knock down the pins they saw on the screen. In the bowling game, shots were made with both extremities.
In the golf game, the individual tried to score points by making accurate shots on the golf course on the screen, using both extremities.
Outcome measures
Sociodemographic data of the children such as age, gender, height, weight, and dominant side were recorded. The GMFCS was used to classify the gross motor function levels of the children with UCP included in the study, and the MACS was used to classify manual abilities. 21 GMFCS and MACS were taken as baseline measurements to obtain information about the clinical characteristics of the participants. Other assessments were performed before and after the 8-week training.
Primary outcomes
ABILHAND-Kids
Upper extremity functionality and manual abilities were evaluated with the ABILHAND-Kids. The ABILHAND-Kids was validated in children with CP. It consists of 21 items containing manual activities. Each item is answered by parents on a 3-point scale (impossible, difficult, and easy). 22 The highest score was 42, and the lower scores indicate correspond to more difficulty in activities. The test/retest reliability coefficient was 0.98, and internal consistency was 0.94. 22
Selective Control of the Upper Extremity Scale
Upper extremity SMC was assessed by the Selective Control of the Upper Extremity Scale (SCUES). The SCUES is a practical and useful video-based assessment tool developed to evaluate upper extremity SMC. The degree of SMC is determined for each joint according to the person’s ability and form of movement: “Normal Selective Motor Control” (3 points), “Slightly Decreased Selective Motor Control” (2 points), “Moderately Decreased Selective Motor Control” (1 point), and “No Selective Motor Control” (0 point).9,23 The total score of the SCUES ranges between 0 and 15, and higher scores indicate better SMC. The intra-rater reliability coefficient was 0.98. 23 Selective movements in the shoulder, elbow, forearm, wrist, and hand fingers were evaluated for both the right and left extremities. The tester passively demonstrated to the participant the movements he or she was asked to perform. Then, the participant was asked to actively perform the demonstrated movement. Filming was done with a video camera, allowing the participant to observe head, body, and other extremity movements while performing the movements.
The joint position sense test was used to evaluate proprioception. The Clinometer (Plaincode app Development) smartphone application was used for evaluation. This application is considered the goniometer-based gold standard for measuring shoulder joint range of motion in both healthy and symptomatic individuals. 24 The interobserver reliability coefficient was 0.98. 24
Measurements were taken in a sitting position with the child’s knees flexed at 90°. Three measurements were made at the target angle for the shoulder (30–60 degrees of flexion and 30–60 degrees of abduction) and elbow (30–60 degrees of flexion) joints, and the arithmetic means of the evaluations were calculated and recorded. To perceive the position, the child’s eyes were closed, and the shoulder for shoulder measurements and the elbow for elbow measurements were brought to the target angle and kept at this angle for 10 seconds. Then, the child was returned to the neutral position and asked to repeat the target angle with the child’s eyes closed, and the goniometer measurement was made using the Clinometer (smartphone application). The difference between the target angle and the angle produced by the child during the test was recorded as the error score. All evaluations and treatments were performed by the same physiotherapist who is an expert in the field.
Secondary outcomes
The entertainment level of physiotherapy sessions and video-based exercises of the individuals with UCP was evaluated using a 0–10 point numerical rating scale. The scale includes numbers from 0 to 10 on a 10 cm horizontal line. On the line, 0 means “not fun at all” and 10 means “a lot of fun”. The entertainment rating was recorded numerically between 0 and 10.
Statistical analysis
SPSS version 25 package program was used to analyze the data. For analyses, variables determined by numerical measurement were given as arithmetic mean and standard deviation (X ± SD). Compliance with normal distribution was evaluated using the Shapiro–Wilk test. Independent samples t-test was used to compare the means of data between groups, and paired samples t-test was used to compare means within groups. The statistical significance level was taken as P < 0.05. The graph was made using the GraphPad Prism 8 program. Cohen’s d ([mean 1 − mean 2]/standard deviation 1) was used to determine the effect size and magnitude of difference between the assessments, and this test estimates effect sizes (ES) as small (0.2), medium (0.5), large (0.8), and very large (1.3). 25
To determine the number of samples to be included in the study, power analysis was performed using G*Power version 3.1 with α = 0.05 and 1-β (power) = 0.80, d = 1.098. At the end of the pilot study, the calculation was made assuming that there was a difference between the mean scores of the ABILHAND-Kids before and after rehabilitation in individuals with UCP. It was determined that a total of 15 individuals should be included, at least 15 individuals in each group.
Results
The sociodemographic and clinical characteristics of both groups are presented in Table 1. There were no significant differences in the average age, height, weight, and mean scores of the GMFCS and MACS of the two groups (P > 0.05) (Table 1). The comparison of the mean scores of the ABILHAND-Kids, SCUES, and shoulder–elbow proprioception values within and between groups is presented in Table 2.
Sociodemographic and Clinical Characteristics of the Participants
GMFCS, gross motor function classification system; MACS, manual ability classification system; SD, standard deviation.
Within- and Between-Groups Comparison of Upper Extremity Functionality, Upper Extremity Selective Motor Control, and Proprioception
P < 0.05 paired samples t-test.
P < 0.05, independent samples t-test.
ES, effect size; Pa, comparison between the groups before the intervention; Pb, comparison between the groups after the intervention; SCUES, Selective Control of the Upper Extremity Scale.
In the comparison of the mean scores of the ABILHAND-Kids before and after the intervention within the group, there was a statistically significant difference in the values of the intervention group (P = 0.001), whereas no difference was found in the values of the control group (P = 0.096) (Table 2). In the within-group comparison of the mean scores of the SCUES, a difference was seen only in the intervention group (R; P < 0.001, L; P = 0.009). In the comparison between groups, no difference was seen in all parameters in pre-intervention values (P < 0.005). There was a difference in the post-intervention SCUES total mean score of the two groups (P = 0.014) (Table 2). Although there were statistically significant differences in the pre-post evaluations in the intervention group in all parameters of proprioception evaluations in the within-group comparison (P < 0.001), a difference was seen only in the 60-degree elbow flexion angle in the control group (P = 0.001). In the intervention group, a very large ES (1.331) was found for the proprioception value of the elbow 60-degree flexion angle before and after the intervention, whereas medium ES (0.508) was found in the control group (Table 2). In the within-group comparison of post-intervention values of proprioception, a significant difference was found in shoulder flexion angles and abduction angles (P < 0.05) (Table 2). Within-group comparison of the mean scores of the ABILHAND-Kids, SCUES, and proprioception is presented in Figure 2.
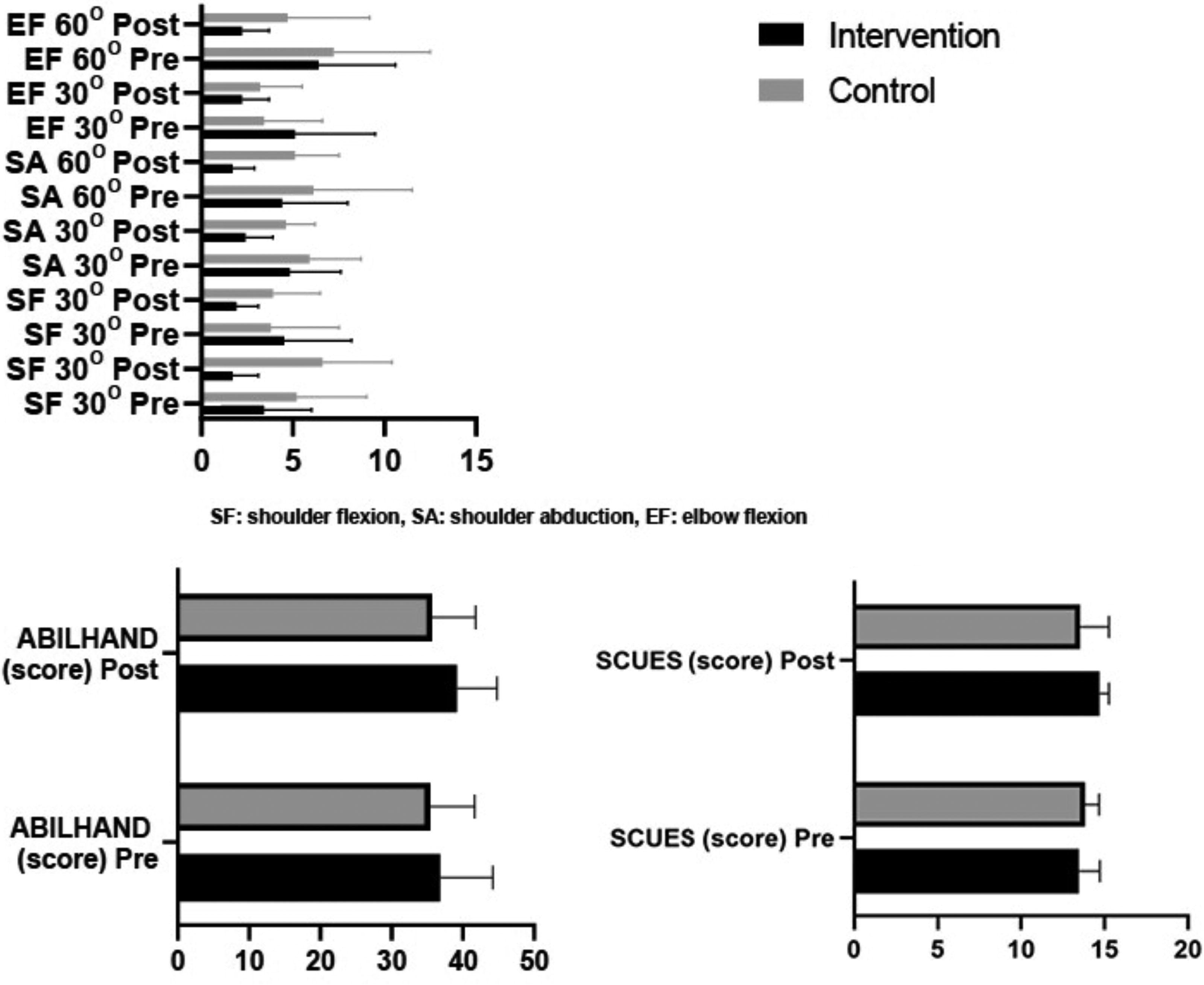
Within-group comparison of the mean scores of the ABILHAND-Kids, SCUES, and proprioception. SCUES, Selective Control of the Upper Extremity Scale.
The entertainment value of the two groups after the intervention was found to be higher in the intervention group (9.6 ± 0.8) than in the control group (6.3 ± 1.5) (P < 0.001).
Discussion
The results of the present study examining the effects of video-based exercises on upper extremity functionality, SMC, and proprioception in individuals with UCP showed that video-based exercises positively improved upper extremity functional abilities, SMC, and proprioception. In addition, all intervention-group children reported that they found the video-based exercises enjoyable. This study is the first to examine the effects of video-based exercises on upper extremity SMC in UCP.
The use of game-based interventions in the long-term rehabilitation processes of individuals with CP effectively ensures participation in physical exercises in an exciting and entertaining environment. 26 Game-based interventions applied in a virtual reality environment are recommended for their contribution to the development of motor functions in daily life activities of individuals with UCP. 19 However, the current randomized clinical trials also stated that game-based interventions made positive contributions to the development of upper extremity grip strength and functional abilities in individuals with CP.17,27 A different randomized controlled clinical trial mentioned game-based interventions’ significant effects on balance, motor functions, running speed, agility, bilateral coordination, and strength. 27 It can be specified that the number of randomized controlled clinical trials examining the effects of video-based interventions for the upper extremity in individuals with CP is limited.17,27–30 A systematic review of randomized controlled clinical trials stated that the effects of videogames applied in the virtual reality environment in upper extremity rehabilitation in CP remain unclear, and higher quality clinical studies are needed. 20
The results of a systematic review with meta-analysis indicated that there were improvements in the upper extremity motor abilities affected by videogames in individuals with CP. 18 In addition, it was stated that video-based interventions were used as outcome measures with Quality of Upper Extremities Skills Test and ABILHAND-Kids in evaluating the effects of video-based interventions on body structure and functions, upper extremity functions, and activity levels in CP.28,30 An explorative study examined the results of the game-based approach in CP with ABILHAND-Kids in daily living activities, and they observed positive improvements in upper extremity performance, but there was no change in movement quality. 29 In this study, upper extremity functional abilities were evaluated with ABILHAND-Kids. It was found that there was a positive and significant improvement in the upper extremity functional skill scores of the UCP intervention group post-intervention. Upper extremity-focused video-based exercises implemented in UCP improve upper extremity performance. This is proof that the children with UCP can functionally integrate the skills they acquired in the video-based exercises into their daily life activities.
In CP, SMC has an important role in movement control in daily life and in performing movements fluently and independently. 8 Previous randomized controlled clinical trials investigated the effects of video-based rehabilitation on arm functions, muscle weakness, balance, postural control, and ambulation in CP. 31 In addition, it is noteworthy that its effects on hand grip strength were also investigated.18,32,33 Compared with previous studies, the current study is characterized by the evaluation of the effects of video-based exercises on upper extremity SMC and proprioception, as well as ABILHAND-Kids score, in the rehabilitation of individuals with UCP. In a randomized controlled clinical trial, it was stated that Kinect Video Game Training positively affected lower extremity SMC, except for right hip abduction, compared with the control group. 34 Apart from this study focusing on lower extremity SMC, no study has been found investigating the effect of video-based interventions on upper extremity SMC in UCP. In the present study, it was found that 8-week video-based exercise interventions for the upper extremity have positive contributions to the development of upper extremity SMC in individuals with UCP. Based on this information, it can be stated that SMC is weak in individuals with UCP, and its development contributes to functionality. It can be put forward that the development of SMC skills is one of the issues that should be the focus of rehabilitation interventions and that video-based exercises can be used in rehabilitation practices in terms of improving the upper extremity SMC of individuals with UCP. It can also be stated that, unlike the control group that received conventional physiotherapy, repetitive movements in video-based exercises, therapist feedback, and the fact that the selected games include functional movements at different angles for the upper extremity have positive effects on children’s motor control.
Proprioception is a complex somatosensory modality consisting of kinesthesia and joint position sense. Kinesthesia is defined as the sensation of limb movement without the use of vision, while position sense is characterized by static limb position. 35 In this study, both factors were taken into account in proprioception evaluation. In light of this information, the possible positive effects of improving upper extremity proprioception in individuals with UCP on motor movement development and the functionality of the affected upper extremity can be mentioned. After a comprehensive evaluation, the findings of this study showed that video-based exercise interventions improved upper extremity proprioception in individuals with UCP. The nature of video-based exercises, which include repetitive activities, unlike the conventional physiotherapy applied to the control group, their entertaining structure, and the fact that they keep motivation high can be considered among the effective reasons for the positive effects.
As rehabilitation processes in CP involve long periods of time, monotony can be boring for children. 36 The use of game-based interventions in rehabilitation processes effectively ensures participation in physical exercises in an exciting and entertaining environment. 25 Moreover, it was also reported to be a noninvasive motivational approach. 37 In this study, all children in the intervention group stated that they found the video-based exercises enjoyable. Incorporating video-based exercises into rehabilitation processes provides the opportunity for positive feedback in terms of repetitive practice and entertainment.
The strengths of this study include the presence of a UCP control group, the equal planning of intervention periods for both groups, and the homogeneity of the groups. Another strength of this study is that it is the first study to investigate the effects of video-based exercises on upper extremity SMC in UCP. The primary limitation of our study is that the inclusion of a broad age range of the study. One of the limitations of this study is that proprioception evaluations were taken only from the affected upper extremity. Furthermore, it is recommended to evaluate both extremities comparatively in future studies. Since post-evaluation measurements were not taken into account in this study, it is not known how long the gains lasted. Therefore, it is recommended to evaluate how long the gains continue in future studies.
Conclusions
In conclusion, the present study revealed that video-based exercises contribute to the development of upper extremity SMC, proprioception, and upper extremity functional abilities in individuals with UCP. This study also presented the applicability of video-based exercises as an entertaining approach in rehabilitation procedures in the development of upper extremity functionality. It can be emphasized that the inclusion of video-based exercises in intervention approaches for the upper extremity functionality of individuals with UCP may make positive contributions to physiotherapists and clinicians working in this field.
Footnotes
Authors’ Contributions
Conceptualization—D.G.K. and Ç.M.; Design—D.G.K. and Ç.M.; Supervision—D.G.K. and Ç.M.; Resources and funding acquisition—D.G.K., Ç.M., Y.K., and M.A.; Materials—D.G.K., Ç.M., Y.K., and M.A.; Data collection and processing—D.G.K., Ç.M., Y.K., and M.A.; Analysis and interpretation—D.G.K. and Ç.M.; Literature search—D.G.K., Ç.M., Y.K., and M.A.; Writing—original draft—D.G.K., Ç.M., and Y.K.; Writing—reviewing and editing—D.G.K., Ç.M., Y.K., and M.A.
Author Disclosure Statement
The authors report no conflict of interest.
Funding Information
The authors received no financial support for the research and authorship of this article.