
Abstract
Objective:
To design a randomized controlled trial combining resistance exercise and cognitive intervention to carry out a dual-task computer-aided product design that combines hardware and software to explore the effects of different intensities of resistance exercise on cognitive function in elderly individuals with cognitive decline.
Materials and Methods:
Forty-eight participants (aged between 60 and 75 years) who satisfied the specified criteria were randomly assigned to one of four groups as follows: control (n = 12), low intensity (n = 12), medium intensity (n = 12), and high intensity (n = 12). The control group exclusively underwent cognitive training, whereas the experimental group underwent dual-task training at varying resistance exercise intensities. The main outcomes were short-term effects on cognitive function and lower limb strength using the Montreal Cognitive Assessment (MoCA), One-Rep Max (1RM) data, and training scores. The secondary outcomes were the effects of the participants’ subjective fatigue and the system availability of the product.
Results:
The experimental group subjected to medium-intensity exercise exhibited the most substantial improvement in MoCA score (P = 0.017). All the groups achieved training scores that were substantially higher than the initial data (P < 0.05), and significant 1RM values were obtained for the left and right legs in the middle- and high-strength groups (P < 0.05). In addition, the participants indicated a positive experience with the application.
Conclusions:
Overall, we found support for the feasibility and acceptability of the product developed by dual-task therapy based on resistance exercise combined with cognitive intervention and showed the initial impact prospect of moderate-intensity resistance exercise. Future applications should be replicated in older individuals with Clinical trial registration: NCT06220565 Ethical approval: H2022013I decline.
Introduction
Population aging is a global reality. The aging population and decreasing physical fitness have led to an increase in the number of individuals showing a trend toward cognitive deterioration. 1 Between normal aging of the brain and Alzheimer’s disease (AD), there are two stages of transition as follows: mild cognitive impairment (MCI) and subjective cognitive decline. 2 Their chance of developing AD is five times higher compared with the general population if they are not treated in a timely manner. 3
Nonpharmacological therapies offer a safer alternative with fewer side effects, 4 rendering them particularly suitable for the elderly because of the minimized risk of drug interactions. Numerous nonpharmacological products are more accessible and easier to use than pharmaceuticals. Examples include easy physical activity, cognitive exercises performed at home, and digital transformation training products (interactive game products, virtual reality game products, interactive hardware, software integration systems, etc.). 5 For instance, Taheri et al. highlighted that technologies such as digital telemedicine can complement traditional methods, offering significant potential to enhance health systems. 6 Bossen et al. created a digital serious game that can be played by patients and their families without the need for professional equipment or high expenditures. This game is designed to train the most significant cognitive decline in the elderly. 7 Faraziani et al. conducted a study that examined the potential of a digital exercise-based health management system to improve the cognitive abilities of older individuals and postpone cognitive decline. It offers evidence to substantiate the use of structured exercise programs and digital training products to preserve cognitive function and mental health in a geriatric population. 8
Nonpharmacological interventions for MCI include exercise intervention, cognitive training, psychotherapy, 9 and cognitive-motor dual-task training (CMDT). 9 Epidemiological evidence suggests that dual-task training, combining physical and cognitive exercises, 10 offers greater improvements in cognitive and physical performance than either training alone. 11 Exercise and cognitive therapies are considered complementary within the framework for fostering neuroplasticity. 12 A recent randomized controlled study has shown that the cognitive benefits of a combined strategy are only effective when both treatment components were applied concurrently 13 ; CMDT has stricter requirements for the cognitive distribution capacity and physical and mental coordination of elderly adults. This assists in delaying the decline in cognitive function and establishes a foundation for translating the benefits of training into living abilities. 14 One study verified the efficacy of mindfulness-based cognitive behavioral therapy and electronic muscle stimulation in enhancing the mental health and balance of the elderly, thereby elucidating the advantages of integrating cognitive and physical dual-task interventions. It also addressed the role of technology in the management of therapeutic interventions and verified the efficacy of dual-task digital health products. 15
While the academic community agrees on the effectiveness of dual tasks in treating MCI, there are bifurcations in the types of exercises and training intensity used in these interventions. The study by Nagamatsu et al. revealed that resistance training, in contrast to aerobic exercise, facilitates increased blood flow to functional areas of the brain, resulting in significant enhancements in memory performance among individuals with MCI. 16 While previous studies have examined the impact of resistance exercise on cognitive function, there is a scarcity of data on the influence of dual-task cognitive intervention depending on various resistance exercise intensities. Taheri noted that while dual-task training can improve cognitive and physical coordination in the elderly, the need for specialized equipment and personnel limits its feasibility in resource-constrained settings, such as community centers or homes. 17
Given the constraints of previous studies, the randomized controlled experiment aims to: (a) investigate the impact of dual-task interventions with varying intensities of resistance exercise on cognitive performance, thereby providing further data for research in this area; and (b) utilize well-established and widely adopted cognitive training materials and implement a digital transformation process to enrich the content and incorporate feedback mechanisms, thereby enhancing adherence to cognitive training protocols. Simultaneously, this approach helps to mitigate the limitations imposed by the unequal distribution of medical resources.
Materials and Methods
Trial design
The 4-week randomized controlled trial adhered to the CONSORT (Consolidated Standards of Reporting Trials (CONSORT) 18 and CONSORT-EHEALTH (Consolidated Standards of Reporting Trials for Electronic and Mobile HEalth Applications and online TeleHealth) 19 guidelines and was approved by the Institutional Ethics Committee for Human Research (H2022013I).
Participants
Participants were subjected to thrice-weekly sessions of dual-task resistance exercise training through interactive product interventions for a duration of four consecutive weeks, aimed at providing them with varied intensity resistance exercise programs and corresponding instructional videos. The recruitment of potentially eligible participants was facilitated by invitations from community managers and through the distribution of flyers in nursing homes. The inclusion criteria were as follows: (1) age between 60 and 75 years; (2) presence of normal auditory and visual functions or absence of auditory and visual impairments when assisted by corrective devices such as glasses or hearing aids; (3) consciousness and capability to engage in exercise of normal intensity on a daily basis; and (4) sufficient cognitive capacity to comprehend standard training and guidance instructions.
The exclusion criteria were as follows: (1) inability to perform lower limb movements, (2) presence of language communication or cognitive problems, (3) history of severe lower limb disease, and (4) lack of agreement from users and their families to participate in the study. Participants who completed the final 4-week evaluation of the experiment and did not drop out were considered for inclusion in this trial. The participants and their families provided informed consent upon joining the group to affirm their voluntary involvement in the experiment.
Randomization, allocation concealment, and blinding
After the baseline assessment of the trial, the participants were randomly assigned to different groups after the following assessment in the trial: control group (single cognitive training), low-intensity resistance exercise group (40% One-Rep Max [1RM]), medium-intensity resistance exercise group (60% 1RM), and high-intensity resistance exercise group (80% 1RM) in a 1:1:1:1 ratio. To maintain the integrity of the double-blind design, an experienced statistician (D.Z.) used STAS software for random assignment, thereby ensuring the concealment of group allocation from both researchers and participants. To further uphold the study’s blinding protocol, the participants were deliberately not briefed on their assigned study group or overarching research hypotheses through a strategy of limited disclosure. In addition, the statisticians were blinded to the allocation of participants to the respective groups, reinforcing the methodological rigor of the study.
Following allocation, participants were sent emails by researchers providing details on how to access the cognitive training application and graded resistance exercise training goods, along with instructions for participating in the field experiments. The participants could contact the researchers via phone or email for queries regarding the application.
Intervention
Procedure
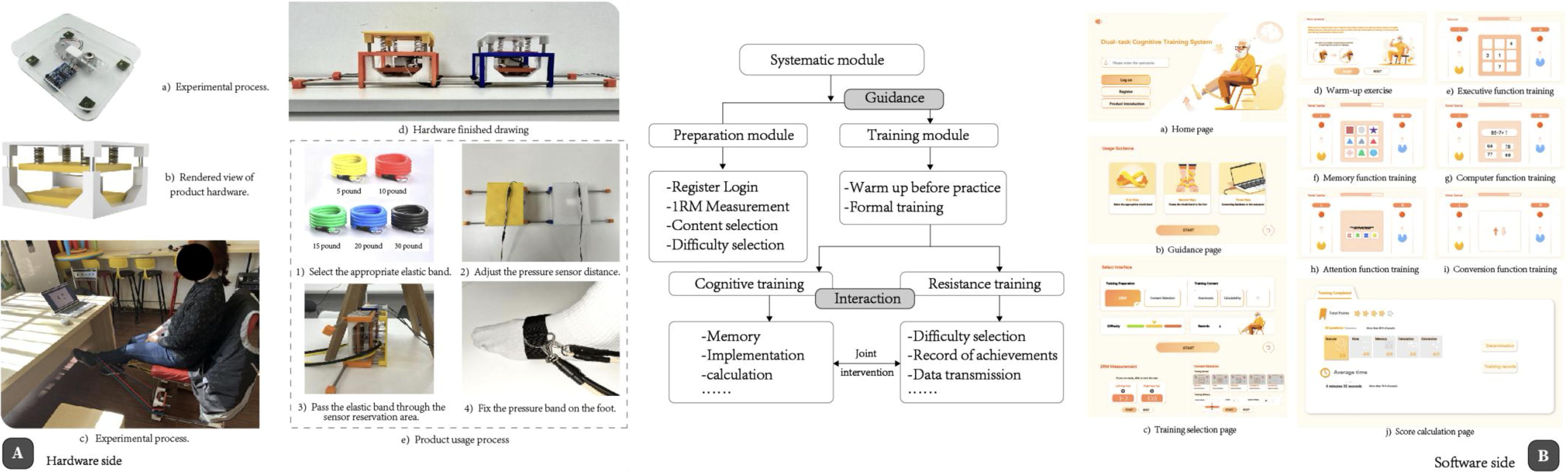
This study developed an interactive training evaluation and intervention system that integrated varying intensities of resistance exercise with cognitive therapy, targeting elderly individuals exhibiting cognitive decline, particularly in the context of dual-task activities. The resistance movement mode of this investigation selected the elastic band based on the safety principle. 20 The product integrates software and hardware to provide computer-aided training that combines resistance exercises with cognitive training. It utilizes nonimmersive training content derived from serious games. 21 Cognitive training is completed by the following two interactive methods: resistance generation and key-answering. Feedback is provided instantaneously when the user inputs information. When utilizing the system, users can select suitable training content and difficulty levels based on their cognitive and physical differences, as illustrated in Figure 1. This study established a specific training duration within the system to maintain constant intervention times across the experimental groups, ensuring controlled variable conditions. 22
Product system structure diagram.
The control group utilized the product exclusively for cognitive training during each formal training session, which encompassed all of the product’s contents, including memory, attention, conversion, execution, calculation, and other training contents.
The experimental group engaged in cognitive training in conjunction with dual-task training that included low-, medium-, and high-intensity resistance exercise. The cognitive training content was identical to that of the control group, encompassing all of the cognitive training content present in the product. As follows is a description of cognitive training:
Executive function training (Fig. 2B-e): A nine-box grid with numbers from 1 to 9 appears on the screen. The task is to select the numbers in ascending order. Memory function training (Fig. 2B-f): A nine-box grid displays images in various colors for 2 seconds. After a 5-second pause, the same grid reappears with distinct images. The task is to recall and click on the previously shown images. Calculation function training (Fig. 2B-g): The screen presents addition and subtraction problems involving two-digit and one-digit numbers. The task is to calculate and select the correct answers. Attention function training (Fig. 2B-h): The screen displays words in different colors. The task is to match the font color with the meaning of the word. Switching ability training (Fig. 2B-i): Arrows indicate how to control a ball with the legs. If the arrow points up, use the same leg to control the ball. If the arrow points down, use the opposite leg to control the ball.
Integration of hardware and software components.

Protocol of the study.
A thorough assessment system was developed using the electronic Montreal Cognitive Assessment (MoCA) questionnaire, cognitive training score, 1RM measurement, supervisor fatigue assessment, and other programs after each training session. It offers a systematic and thorough evaluation procedure for elderly individuals experiencing cognitive deterioration, and the software system logs the user’s training outcomes, including training duration, precision, and other relevant data. The training results will be displayed using computer vision technology to assist health care professionals in observing training progress and enhancing the evaluation of training outcomes and cognitive abilities.
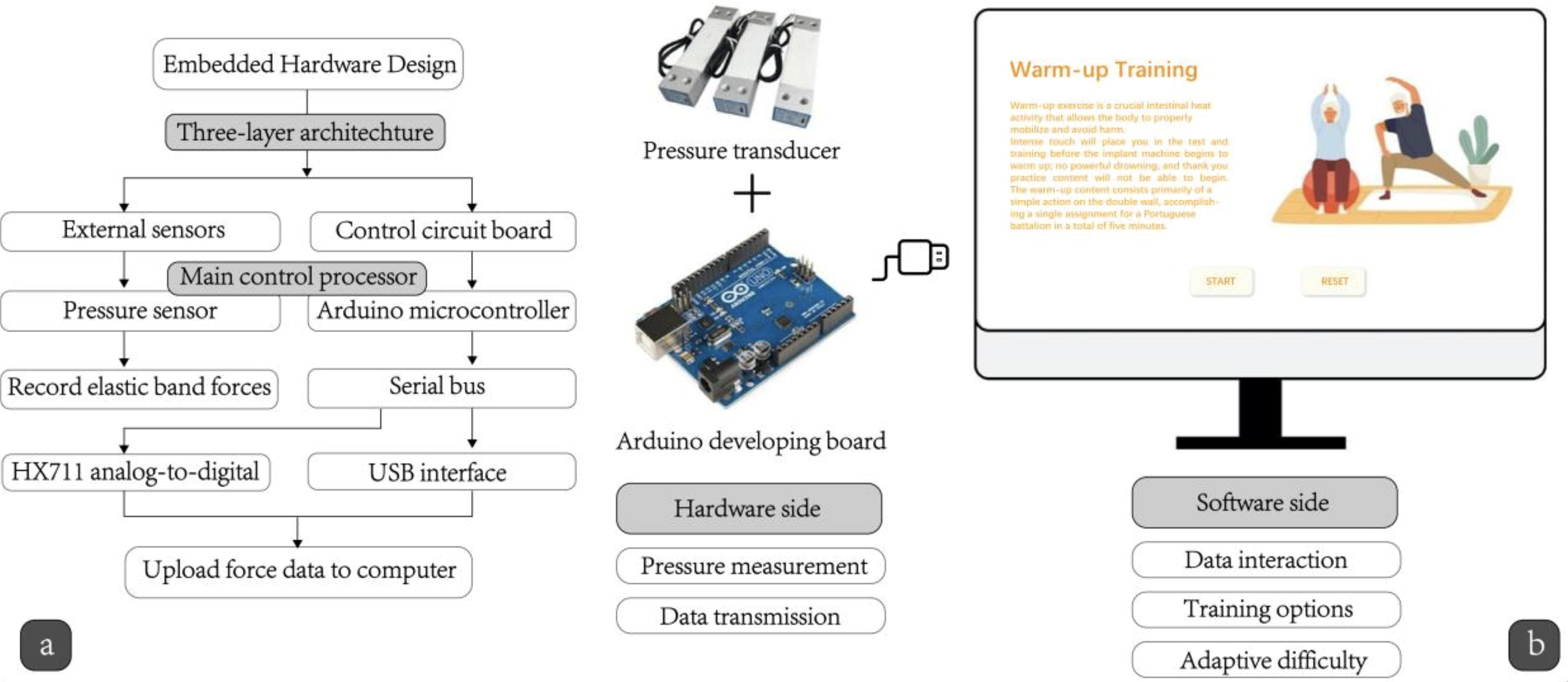
Integrated hardware
The embedded hardware design is a three-tier architecture that consists of external sensors, control circuit boards, and power supplies. The elastic band’s force is recorded by the external sensor, which is a pressure sensor. The control circuit board layer transforms the force data into digital signals and transmits them to the computer via the USB interface. The user’s lower limb force data are collected by the pressure sensor on the hardware side. The dedicated analog/digital (A/D) converter processor of the HX711 weighing sensor is responsible for signal acquisition and amplification, as well as A/D conversion. The SerialPort class Unity plug-in Ardity of C# is utilized to facilitate data transmission between Unity and Arduino, with the Arduino microcontroller serving as the primary control processor. To utilize the Ardity plug-in, it is necessary to configure the serial port name and transmission rate to match those of the Arduino Integrated Development Environment for data communication.
The hardware model is designed using SketchUp software to ensure that it is compatible with the sensor’s dimensions, thereby preventing injury and ensuring its normal operation. The sensor is secured to the resin plate using fasteners, and the base is installed at the bottom to enhance the protection. It is imperative to design the architecture of the entire hardware product to position the sensor and finalize the assembly after the sensor has been assembled. SketchUp is used to model the architecture in its entirety, and resin materials are used to 3D print it. The structure is installed with the pressure sensor that has been assembled, and the spring is tightened to prevent movement and guarantee the precision of the pressure measurement. A sliding steel pipe is incorporated into the hardware to facilitate the adjustability of the device, allowing individuals of varying sizes to adjust it to their requirements, as illustrated in Figure 2.
Software equipment
The software component was engineered using the Unity platform, with data transmission facilitated by the Ardity plug-in for the Arduino. The visual effect is determined by the completion of the high-fidelity prototype in Figma. After that, the necessary design elements, including typefaces and buttons, are imported into Unity as image resources. Unity is then used to develop the software in accordance with the interactive logic in Figma. Software functionality is divided into three main segments as follows: 1RM data collection, selection of training content and difficulty, and cognitive training execution. Initially, the users are required to register within the login system upon entering the software platform. This registration facilitates the storage of training results and records in the user’s account, allowing medical professionals to conduct subsequent analyses, after which the software prompts users to select an appropriate resistance exercise intensity. Users then attach the wearable device to a specified area on their lower limbs and initiate a training session once the device is connected. Throughout the training, interactive user data were transmitted in real time to the software via a hardware device, enabling visual interaction. Feedback was delivered through both text and images, which enhanced user engagement with the training program.
Outcome measures
Participants were administered a validated questionnaire either online or in-person at baseline and again 4 weeks postintervention, the experimental procedure is illustrated in Figure 3. No financial incentives or other forms of compensation were provided for the questionnaire completion or study participation. Demographic information was gathered at the outset of the study and is comprehensively detailed in the section dedicated to the measurement of the results.
Primary outcomes
Left and right leg 1RM data
This study analyzed the impact of varying training intensities on lower limb muscle strength by comparing the subjects’ left- and right-leg 1RM data before and after the intervention. This analysis aimed to identify the optimal training intensity and evaluate the effectiveness of the intervention in enhancing lower limb strength in the elderly. 23
Training scores
The training score is determined by accurately fulfilling the training-content requirements within an interactive product. Establishing a specified completion time for each training activity facilitates scoring based on the completion of resistance exercises and cognitive tasks before the countdown is completed. The scores for each task and the total score for the entire training session were documented, facilitating the tracking of training completion and providing insight into the subjects’ cognitive aptitude.
Montreal Cognitive Assessment
The MoCA consists of 11 examination items spanning eight cognitive domains: attention, executive function, memory, language, visual-spatial abilities, abstract thinking, arithmetic, and orientation, culminating in a total score of 30 points. With its cutoff value set at 26, the MoCA exhibits a sensitivity of 90% for detecting MCI and 100% for mild dementia, whereas its specificity for identifying cognitively healthy elderly individuals is 87%. 24
Secondary cognitive outcomes
Borg Rating of Perceived Exertion Scale
The Borg Rating of Perceived Exertion scale is an established tool designed to quantify individuals’ self-perceived exertion levels during physical activities, ranging from 6 (indicating no exertion) to 20 (representing maximum exertion).25,26
System Usability Scale
The System Usability Scale (SUS) was used to assess perceived usability. Upon completion of the designated content tasks, participants utilized the SUS for rapid evaluation. Higher scores indicated superior system usability for the product. 27
Sample size determination
Using the paired means test for sample size determination, 28 10 samples were randomly selected. The calculation of the requisite participant sample size was performed using the PASS software, predicated on pre-experimental data. This preliminary analysis yielded the mean of three paired differences, with the standard deviation (SD) of these paired differences quantified at 2.9. Using these parameters facilitated the determination of a sample size (n) of 12, with a significance level (alpha) of 0.05 and statistical power (power) of 90%.
Experimental process
The study spanned 4 weeks and included three experimental groups and one control group. The interventions were conducted thrice per week, with each session lasting approximately 20 minutes. The experimental protocol was composed of three phases as follows: preparation, warm-up, and dual-task training.
Baseline data collection
A baseline measurement was administered to all participants using the product 1 week before the commencement of the experiment. The baseline data consisted of cognitive training scores, MoCA, and left and right limb 1RM measurement data.
Measurement of the 1RM and warm-up exercise before the experiment
The participants were required to limber up for approximately 5 minutes before the formal experiment. The 1RM measurement of the left and right legs is conducted following the warm-up, and the user may proceed with the measurement once they are prepared. To prevent injury, the user must apply progressive force during the measurement. Gradually increase the weight, repeating the process until the utmost weight that can be safely completed on a single occasion is determined. The subject’s current 1RM is the maximum weight that can be effectively completed on a single occasion. 29 The 1RM measurement is conducted before each formal training session, and the intensity of each training is determined by the percentage of 1RM values that were measured before each training. Then, the subjects’ 1RM values are monitored in real time and adjusted to mitigate the effect of physiological adaptation on their relative exercise intensity.
Stage of formal experimental training
Following the measurement, a 10-minute interval was implemented, and the formal training phase commenced. There was a total of three cycles of formal training, each lasting approximately 3 minutes. A 3-minute break was taken between each of the two training sessions. The overall duration is approximately 20 minutes. During a single training session, it is necessary to complete the cognitive training assignment and the specified percentage 1RM resistance exercise 6–10 times. The subjective exhaustion was assessed using the Borg perceived fatigue scale following the conclusion of a single experiment to assess the difference in fatigue between the pre- and postexperiment periods.
The control group exclusively utilized the product for cognitive training during each formal training session, encompassing all content. Users can select training materials for a single session based on their specific requirements, which may include topics such as memory, attention, conversion, execution, and calculation. Dual-task training was performed by the experimental group, which consisted of low-, medium-, and high-intensity resistance exercises. The cognitive training material used in the product was identical to that used in the control group, which comprised the entire cognitive training content.
Postexperiment phase
Following 4 weeks of experimental intervention, MoCA was administered to reevaluate the cognitive functions of the participants. Participants also completed a SUS to assess the usability of the product system. A brief semi-structured interview was also conducted to gauge the participants’ postexperiment psychological responses, their perspectives on the product, and suggestions for future enhancement.
Statistical analyses
The data collected in the experiment were analyzed using SPSS 26 and Microsoft Excel. The measurement data are presented as mean ± SD and median (quartile) [median (P25, P75)]. The nonparametric Kruskal–Wallis (K-W) test was used to compare data between the subjective and objective data groups, 30 whereas the Wilcoxon signed-rank test was used within each group. Measurement data are presented as mean ± SD and median (interquartile range) [median (P25, P75)].31,32 The nonparametric K-W test was used to compare data between the subjective and objective groups, whereas the Wilcoxon signed-rank test was used for within-group comparisons. 33
Results
Baseline characteristics
We randomly allocated 48 participants who met the recruitment criteria into four groups as follows: a control group, a low-intensity resistance exercise group (40% 1RM), a medium-intensity resistance exercise group (60% 1RM), and a high-intensity resistance exercise group (80% 1RM). The mean age of the study sample was 67.5 years (SD = 7.96), with a predominance of female participants (26/48, 54.17%). Daily activities were performed using the right leg as the inertial leg (48/48). Table 1 summarizes the demographic characteristics and MoCA scores along with the K-W test results for each group. The age composition, MoCA scores, and cognitive training scores of the groups in the K-W test at baseline were not significantly different (P > 0.05), despite the fact that the subjects’ cognitive status and age range (60–75 years) varied. Therefore, it is possible to ascertain to a certain extent that the intervention study’s outcomes will not be impacted. The lack of significant variance among the groups renders the data appropriate for further trials and analyses.
Participant Baseline Characteristics
P < 0.05.
P < 0.01.
MoCA, Montreal Cognitive Assessment; 1RM, One-Rep Max.
At baseline, all participants, except one, believed that cognitive training products were effective in alleviating cognitive decline, with 76% (65/85) asserting that such products could facilitate the restoration of cognitive function. A significant proportion of the participants reported a lack of active engagement in interventions aimed at mitigating cognitive decline. Adverse events were infrequently reported, with only one documented case of serious adverse events.
Primary outcomes
Application utilization in the control and intervention groups is shown in Table 2. Following a 4-week training intervention utilizing the product, a significant enhancement in MoCA scores was observed in the low-intensity group compared with baseline values (preintervention: mean = 25.00 (24.00, 26.00); postintervention: mean = 25.00 (24.00, 27.00); P = 0.046). The moderate-intensity group exhibited a notable increase in MoCA scores from the baseline (preintervention: mean = 25.00 (24.00, 26.00); postintervention: mean = 27.00 (27.00, 27.00), P = 0.017). No significant alteration in MoCA scores was detected in either the control or high-intensity groups postintervention. Intergroup comparisons revealed a statistically significant difference in the delta of the MoCA scores pre- and postintervention between the groups (P = 0.008). Specifically, marked differences were identified between the moderate-intensity group and both the control group (P = 0.022) and the high-intensity group (P = 0.022), whereas no significant differences were found among the remaining groups. The training scores before and after training in each group were subjected to the Wilcoxon signed-rank test exclusively because of the distinct training methodologies used in each group. The findings indicated that, relative to the initial data, the training scores of both the control and experimental groups were markedly elevated (P = 0.017). The training score data were analyzed between the groups using the Wilcoxon signed-rank test. The results indicated a statistically significant difference between the control group and the other three groups (P < 0.05). Simultaneously, there were substantial disparities between the low-intensity and high-intensity groups, as well as between the medium-intensity and high-intensity groups (P < 0.05).
Results of Primary and Secondary Interventions
P < 0.05.
P < 0.01.
Negligible.
Medium.
C, Control; LIG, Low-intensity; MIG, Medium-intensity; HIG, High-intensity.
Analysis of 1RM data for the left leg revealed that the moderate-intensity group exhibited a statistically significant enhancement in strength performance compared with baseline measurements (preintervention: mean = 9.39, (7.90, 11.24); postintervention: mean = 9.97, (8.53, 11.76), P = 0.018), as illustrated in Figure 4. Similarly, the high-intensity group demonstrated a significant increase in strength performance postexperiment relative to baseline (preintervention: mean = 9.63, (8.28, 10.54); postintervention: mean = 10.02, (8.97, 10.98), P = 0.018). The analysis pertaining to right leg strength indicated significant improvements in both the moderate-(P = 0.018) and high-intensity (P = 0.018) groups when comparing pre- and postintervention data. Following intergroup evaluation in the left leg 1RM, the findings indicated that the moderate-intensity group experienced a substantially greater increase in left leg strength than both the control group (P = 0.034) and the low-intensity group (P = 0.020). Significantly greater limb strength improvement was observed in the high-intensity group than in the control (P = 0.024) and low-intensity groups (P = 0.013). The improvement in strength of the right leg did not differ significantly between the groups (Fig. 4).
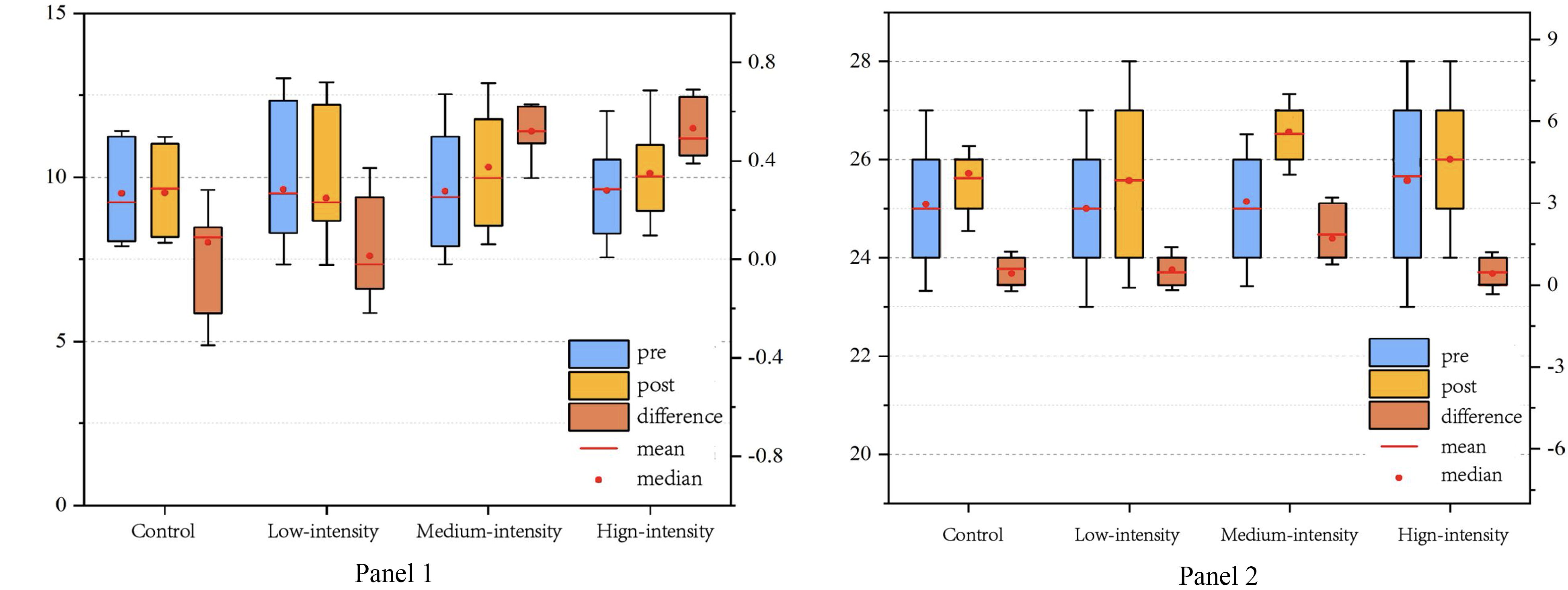
Variations in the 1RM and MoCA scores of the left leg following the intervention.
Secondary outcomes
This study used the Borg Rating of Perceived Exertion Scale (BRPE) to evaluate the impact of training products on the perceived training intensity of the elderly. The findings revealed that the mean score of the control group, classified as extremely relaxed, was 10.29. The low-intensity group’s mean score was 11.71, which was positioned between “extremely relaxed” and “relaxed.” The medium-intensity group had a mean score of 12.43, categorized as “relaxed,” whereas the high-intensity group recorded a mean score of 14.43, indicating a sensation of being “a little fatigued.” Data between the groups were analyzed using the paired Wilcoxon signed-rank test. The findings indicated statistically significant differences (P < 0.05) between the control group and the other three groups.
System availability was evaluated using SUS, and the experimental group achieved an average system usability score of 73.27 out of 100. Scores exceeding 70 were classified as good, indicating a high system availability.
Effect size
Cliff’s Delta is a nonparametric statistic that is used to quantify the effect magnitude between two independent samples. It denotes the probability that the value of random selection in one sample is greater than, equal to, or less than the value of random selection in another sample. The degree of contact between the fractional distributions is indicated by this metric, which is supported from −1 to 1. As follows is an explanation of the Delta Cliff effect: | d | < 0.2: Negligible difference; 0.2 ≤ | d | < 0.5: Medium difference; 0.5 ≤ | d | < 0.8: Large difference. 34 The level of significance for all analyses was 5%. The R software package 35 and the Statistical Package for the Social Sciences Version 17 software package were used to analyze the data. 36
The MoCA cognitive performance Cliff’s Delta value of the medium-intensity group was −0.74, which was substantially higher compared with the other groups. The MoCA scores of the high-intensity group and the control group were both −0.34, suggesting that the scores were relatively low and similar. Cliff’s Delta was 0.55 in the comparison between the moderate-intensity group and the high-intensity group, which further substantiated the moderate-intensity group’s substantial advantage in cognitive score improvement. The training scores of the medium-intensity group were significantly higher than those of the control group and other groups, as indicated by the Cliff’s Delta value of −0.55. The high-intensity group’s Cliff’s Delta value was −0.36, slightly higher than the control group, but not as good as the medium-intensity group. The comparison between each group and the control group revealed that the medium-intensity group performed the best in terms of training scores (Cliff’s Delta = −0.58), followed by the low-intensity group (Cliff’s Delta = −0.38), and the high-intensity group performed relatively poorly (Cliff’s Delta = −0.14). In the comparison of right leg 1RM, the Cliff’s Delta value of the high-intensity group was −0.36, which was marginally lower compared with the moderate-intensity group, despite the fact that the P values of the moderate-intensity and high-intensity groups were identical before and after the experiment. In the left leg 1RM group, the medium-intensity group had a substantially higher score than the high-intensity group, as evidenced by the Cliff’s Delta value of 0.74 when comparing the two groups.
Discussion
The academic consensus recognizes the effectiveness of dual-task interventions for MCI.9,37,38 While the impact of resistance exercise on cognitive function has been studied, there are limited comprehensive data on the effects of different intensities of resistance exercise in dual-task cognitive interventions. To fill this gap, this study aimed to address cognitive decline in the elderly by integrating resistance exercises with cognitive interventions using a dual-task computer-aided product design that encompasses both hardware and software components. This investigation focused on the efficacy of a dual-task cognitive intervention model in mitigating cognitive deterioration among the elderly. It assessed the model’s potential advantages in enhancing cognitive function and analyzed how varying intensities of resistance exercise affected cognitive capabilities, with the goal of identifying the optimal intensity level for resistance exercises to maximize the effectiveness of the intervention. Our findings indicate that the dual-task approach, which combines resistance exercises with cognitive interventions, is both feasible and promising. It has shown potential in aiding elderly individuals to improve cognitive function and bolster lower limb strength.
The findings revealed that the training performance of each group, including the control and high-intensity groups, significantly exceeded the baseline measurements of cognitive task execution. At the same time, comparison between groups shows that the score of moderate-intensity training was significantly higher compared with the high-intensity group. The MoCA scale scores of the low- and medium-intensity experimental groups exhibited significant increases from their baseline data post-trial, indicating overall cognitive enhancement. Engaging in physical activities in cognitively challenging environments offers more neurological and cognitive benefits than solitary physical activities. Dual-task training notably enhances cognitive performance, memory, executive function, emotional well-being, and activities of daily living in adults with cognitive decline.10,39 These outcomes are consistent with the experimental results obtained by Fabel et al.40,41 The training intensity disparity between all exercise methods is demonstrated in our intergroup comparison. The MoCA scale score improvement postexperiment was significantly more pronounced in the moderate-intensity group than in the control and high-intensity groups. No notable differences were observed in score improvements between the control group and the low- and high-intensity exercise groups. This study indicates that a regimen combining moderate-intensity resistance exercise with cognitive training significantly enhances cognitive function in elderly individuals with cognitive impairment in the short term. This finding is noteworthy and suggests that future research should investigate the long-term effects of such intervention strategies, specifically those that combine moderate-intensity resistance exercises with cognitive training and examine the role of supervision in enhancing these effects.
No significant changes were observed in the 1RM data for the left and right legs before and after the experiment in either the control or low-intensity groups regarding lower limb strength improvement. Conversely, the postexperiment 1RM data for both the left and right legs in the medium- and high-intensity groups demonstrated significant increases compared with the pre-experiment values. The analysis of pre- and postexperiment 1RM data indicated that medium- and high-intensity resistance exercises significantly enhanced the left lower limb strength in elderly individuals. Although no marked difference was noted in the impact on right leg muscle strength across the groups, postintervention analysis showed that the right lower limb strength in the medium- and high-intensity groups was significantly greater than the preintervention level, highlighting a clear intervention effect. The minimal change in right leg strength postintervention may be due to the established movement patterns on the right side of the elderly, suggesting that extended effort and physical activity are required for significant modifications. 42 The application of dual-task training appears promising for improving lower limb strength in older individuals. Furthermore, increasing the training duration might yield a statistically significant improvement in right lower limb strength.43–45
The Cliff’s Delta value was used to further quantify the effect magnitude of various groups. The results indicated that the improvement of moderate-intensity training scores was substantially distinct from that of other groups, with high-intensity groups following in that order. The Cliff’s Delta value of 0.55 in the comparison between the moderate-intensity and high-intensity groups further substantiated the moderate-intensity group’s substantial advantage in cognitive score improvement. In addition, the moderate training intensity may have a more positive effect on cognitive function, as evidenced by the greatest effect on MoCA score and training score difference in the medium-intensity group. This was followed by high-intensity training, low-intensity training, and the control group. The medium-intensity group demonstrated substantial advantages in the right leg 1RM and left leg 1RM scores during the assessment of lower limb strength, particularly when contrasted with the low-intensity group. The medium-intensity group exhibited a greater difference in effect intensity in both scores. It further supports the short-term intervention strategy of medium-intensity resistance exercise in conjunction with cognitive training, which has the most apparent impact on the enhancement of cognitive function and lower limb strength exercise in the geriatric group with cognitive decline.
Our investigation into dual-task training produced outcomes aligned with those reported by Donnezan et al.,37,46 indicating that dual-task training might more effectively enhance both physical and cognitive performance than training in either domain alone. 47 Cognitive and physical training programs can improve cognitive and motor functions in individuals with MCI. 48 A combined approach can significantly improve the cognitive performance of elderly individuals with dementia. The integrated training program encompassing various tasks significantly affected memory, executive function, attention, visual-spatial ability, and overall cognition in the elderly population. 49 Our research advances beyond previous studies by addressing the limitations of fixed training difficulty levels for individual participants. By acknowledging individual differences, our approach facilitates the flexible adjustment of training difficulty and content, ensuring adaptive training tailored to each participant’s needs. Our training solutions enable precise assessment of participants’ distinct skill levels within cognitive training programs. The post-test results indicated that these innovations positively influenced the cognitive and physical training and assessment processes in the elderly population. The experiment demonstrated that integrating cognitive training with resistance exercise compels participants to engage in complex tasks such as inhibition, planning, and executing rapid motor responses to external cues, potentially providing broader cognitive benefits than domain-specific tasks such as memory training alone.50,51 Nonetheless, additional research is required to substantiate and quantify the positive effects of this integrated approach.
The subjective fatigue scores of the subjects exhibited an upward trend as resistance exercise intensity increased. Resistance training at a high intensity will increase the elderly’s fatigue during dual-task cognitive training, which may be detrimental to their ability to maintain consistency over the long term. The experimental group’s average usability score for product availability was 73.27 points, denoting acceptable usability but also highlighting substantial potential for enhancement. This may be ascribed to the dual-component framework of the product, which comprises hardware and software elements. Consequently, technicians must initiate instructional guidance for elderly users due to the complexity of their operations. It is recommended that the product be optimized to simplify the user interface by reducing the number of operational steps.
Following a 4-week experimental intervention, this study explored the application of serious gaming methodologies to product interaction strategies within traditional cognitive training frameworks, starting with the objectives of functional cognition, behavioral interaction, and emotional experience. 12 Using both subjective and objective measures, this study evaluated a product’s efficacy in enhancing the cognitive function of elderly users, improving training adherence, and enhancing user experience.52,53 Experimental observations indicate that, in the short term, dual-task training interventions, which incorporate secondary cognitive or motor tasks, can concurrently augment physical functions (such as lower limb strength) and cognitive functions in elderly individuals under dual-task scenarios (e.g., response time to auditory cues during resistance exercises or balance maintenance). Furthermore, the product encourages user self-motivation, effectively ameliorating psychological issues, such as lack of confidence, anxiety, and tension experienced by elderly individuals during training. Through serious gamified interaction, the product fulfills users’ social-emotional needs and aspirations for self-actualization, boosts their eagerness to actively engage in rehabilitative training, and positively influences training compliance. However, the extent to which these benefits extend to untrained cognitive ability remains unclear.
Limitations and suggestions
This study has several limitations. This study focused on senior individuals with at least one junior high school education level, which may limit the generalizability of the findings to other populations. In addition, participants were selected from a nonrepresentative sociological society, which could have influenced the study outcomes. 54 While this study demonstrates that interactive training products can notably enhance the cognitive level and lower limb muscle strength of senior individuals in the short term, it does not establish the sustainability of training effects or other transfer effects. 55 Therefore, the sample size and intervention time for the product must be increased. 56
Furthermore, improvements can be made to the hardware prototype of the device. Data lines were used to transfer data between the software and hardware to ensure a fast and stable data transmission during the experiment. However, the presence of numerous wire ports on the exterior of hardware can affect the functionality of the product. One potential direction for improvement is to incorporate data storage or utilize a wireless transmission module with proven stability and timely data transmission to enhance a product’s esthetics and user experience.
There is also potential for enhancing the personalization and richness of interactive training software content. The practical products of this study currently encompass cognitive domain training content such as memory, attention, executive function, conversion, and processing speed. However, each training content only allows difficulty adjustments, resulting in a relatively limited selection of training options for users. Consequently, prolonged use of a product may lead to negative user emotions and diminished enthusiasm for training. 57 Furthermore, an unresolved question remains regarding the extent to which the benefits of this training regimen can be generalized to cognitive skills that have not been directly trained.50,58 Therefore, it is necessary to develop more training content to expand user choices. This expansion can enhance user initiative in training and involve the product in a broader range of cognitive areas. 59 Nevertheless, the significance of the research findings and the application potential of the developed products are indisputable.
Conclusion
In summary, we found support for the feasibility and acceptability of combined resistance exercises and cognitive intervention therapy. The novelty of this research lies in the fact that it is confirmed via randomized controlled trials utilizing both subjective and objective data that overall cognitive function and lower limb muscle strength are enhanced in products designed with moderate-intensity resistance exercises in conjunction with cognitive intervention therapy. The enhancement effect is anticipated to gain widespread acceptance and implementation among community-dwelling elderly people with cognitive decline, and the initial findings offer promise, hopefully, to inform future effectiveness research in this field.
Footnotes
Acknowledgments
The authors thank the Human Subjects Research Ethics Committee for allowing access to patients and all participants for their collaboration in this study. The authors would like to thank the contributions of the following research assistants who assisted with the data collection, data management and/or data organization for this study: Mr. Xingqiang Zhang.
Authors’ Contributions
T.W. and T.H. contributed to study design. T.W. performed the data collection and analysis. T.H. and D.Z. wrote this article. The authors have reviewed and approved the final version of this article. This article has been submitted solely to this journal and has not been published or submitted elsewhere.
Ethical Approval
This study was approved by the Human Subjects Research Ethics Committee (reference number: H2022013I), which confirmed that the study complied with the National and International Guidelines for Scientific Research with Humans. All participants provided written informed consent before participating in the study.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available, but are available from the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China(72471140), National Key R&D Program (Grant No. 2022YFB3303303, First label) and the Fundamental Research Funds for the Central Universities (Grant No. YG2023ZD10).