
Abstract
Objective:
The aim of this study was to examine the effect of technology-based rehabilitation on grip strength, functionality, and disease activity in rheumatic diseases with hand involvement, and to compare these effects with the effects of conventional hand rehabilitation and with a control group that continued routine life.
Materials and Methods:
The study included 45 patients, with a mean age of 52.24 ± 10.03 years, who were diagnosed with rheumatic disease involving the hand. The patients were randomized to an intervention group (n = 15), conventional group (n = 15), and control group (n = 15). A virtual reality (VR) application with a leap motion controller (LMC) device was applied to the intervention group and stretching and strengthening exercises were applied to the conventional exercise group twice a week for 8 weeks. Evaluations were made using the Disease Activity Score-28, dynamometer, pinch meter, Michigan hand outcome test, Duruöz Hand Index, Jebsen hand function test, and 9-hole peg test.
Results:
A significant difference was determined in favor of the LMC group in terms of the Jebsen Hand Function test, 9-hole peg test and grip strength after the intervention (P < 0.05).
Conclusion:
For patients with rheumatic diseases with hand involvement, VR rehabilitation via LMC under the guidance of a physiotherapist has positive effects on the patients’ grip strength and hand functions. Developing approaches that will maintain patients’ motivation for exercise during the treatment process may help increase and maintain these effects.
Introduction
Effects such as pain, swelling, tenderness, deformities, limitations, strength and function losses, and skill and coordination deficiencies in the hand joints, which are frequently seen in patients with rheumatic diseases involving hand impairments, are included in body structure and function disorders within the framework of the International Classification of Functioning, Disability and Health (ICF).1–3 These effects caused by disease activity are reflected in individuals’ daily life activities such as eating, changing clothes, and writing, and appear as activity limitations within the framework of ICF. 4 Even if patients continue their routine drug treatments, as they become immune to the drug over time, the drug cannot have the same effect as it did initially and the toxic load gradually increases. 5 Even if the patient is in the remission period, the structural damage to the hands continues to progress. 6 Perrotta et al. 7 reported that exercise plays an important role in managing clinical symptoms and comorbidity in the inflammatory arthritis group, including rheumatoid arthritis (RA) and psoriatic arthritis (PsA). The function of the hand can be ensured with adequate anatomical integrity, mobility, sensation, coordination, and muscle strength. The European Alliance of Association of Rheumatology (EULAR) recommends physical activity and exercise to improve the range of motion, strength, function, skill, and coordination of the hand in rheumatic diseases. 8
In recent years, technology-based rehabilitation applications have been used in hand rehabilitation programs, especially in chronic diseases, as they increase the patient’s motivation and compliance with rehabilitation, as well as providing similar effects to those of conventional rehabilitation. Leap motion controller (LMC), one of these applications, is used in hand rehabilitation because it is small in size, low-cost, portable, contactless, easy to use, and provides visual and auditory feedback. 9 It is a control device consisting of an optical sensor that works with computer interaction. The LMC is a motion-based device specifically designed to acquire 3D positions and orientations of hands and fingers, which consists of two monochrome IR cameras and three infrared cameras. 10 The variety of virtual reality (VR) exercises applied with the LMC allows the exercises to be performed even if there are deformities in the hand. In addition, while patients are in remission, they can perform VR exercises without contact within their active limits, even if they have swelling and tenderness in their joints. The fact that the device is contactless, not working with a marker, has the advantage of providing the necessary hygiene for individuals with rheumatic disease, which is an autoimmune disease. The use of LMC in children with Juvenile Idiopathic Arthritis, one of the rheumatic diseases in which hand involvement is seen, has been reported to result in significant improvements in the gross and fine grip strength of the hand, pain level, coordination, skill, functionality, and well-being, with an 8-week rehabilitation program. 11
To the best of our knowledge, there is only one study in the literature in which the LMC was applied to patients with hand and wrist stiffness. The sample of that study included patients with rheumatic disease diagnosed with RA. It was concluded that adding VR training with LMC to conventional physiotherapy resulted in improvements in grip strength, dexterity, and disability compared to conventional physiotherapy alone. 10 However, no study has been found in which VR was used with LMC in patients with rheumatic diseases with hand involvement. The aim of this study was to examine the effect of technology-based rehabilitation on grip strength, functionality, and disease activity in patients with rheumatic diseases with hand involvement, and to compare these effects with those of a conventional hand rehabilitation program implemented under the supervision of a physiotherapist and the control group that continued routine life.
Materials and Methods
Study design
This was a randomized controlled study which included three groups. Approval for the study was granted by the Noninterventional Clinical Research Ethics Committee of Antalya Health Sciences University (decision no: 2023–088). Informed consent was obtained from all study participants and assurances were given of the confidentiality of the information. The study was registered in the clinical trials database (registration number: NCT06385574). A flowchart of the study is shown in Figure 1.
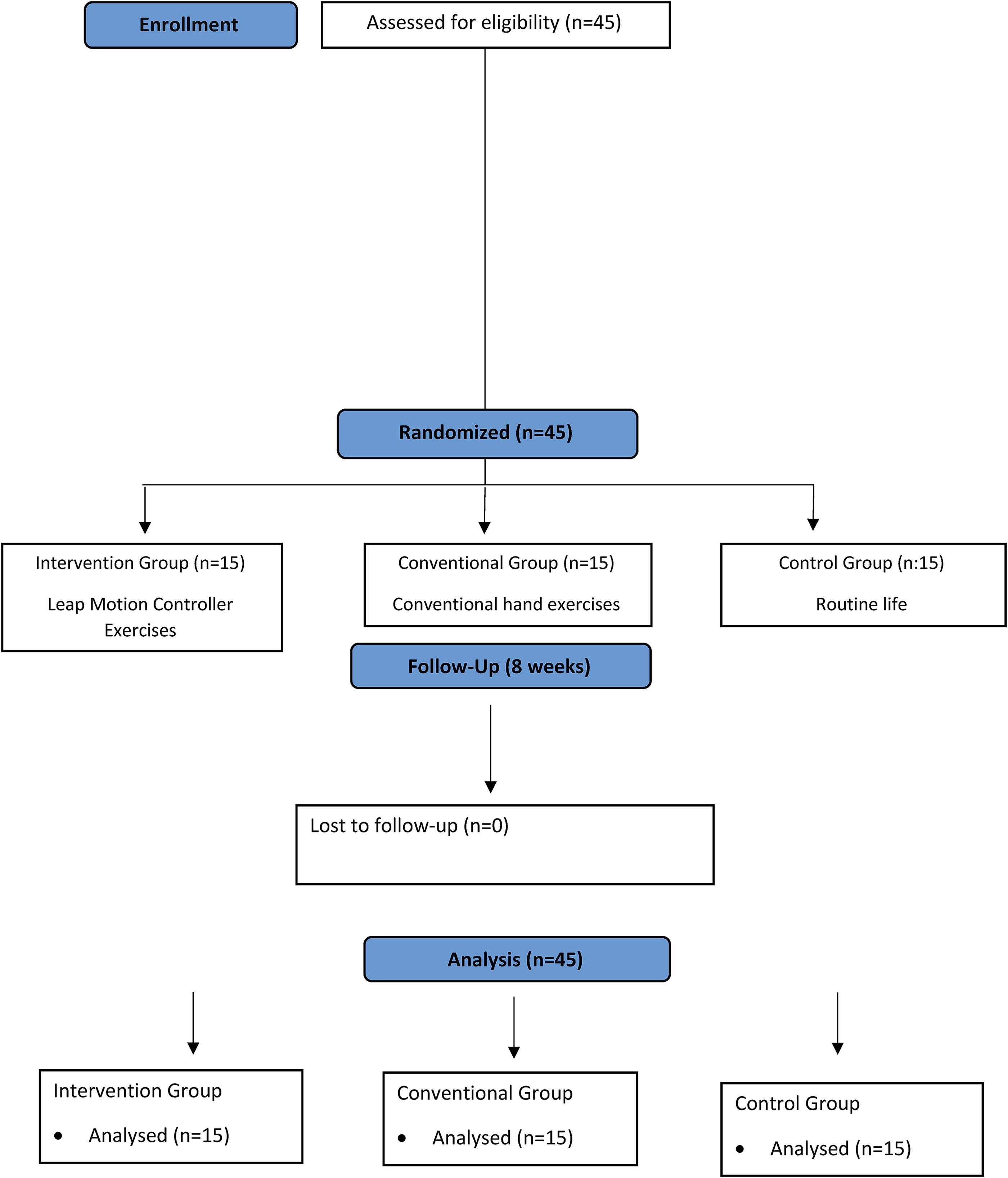
CONSORT flow diagram.
Participants
The study included 45 patients, aged ≥18 years, who presented at the Rheumatology Outpatient Clinic of Training and Research Hospital and were diagnosed with rheumatic disease with hand involvement. The study inclusion criteria were defined as a diagnosis by a rheumatologist of rheumatic disease meeting the most recent criteria, involvement of the hand joints (pain, swelling, and tenderness), age ≥18 years, being on stable drug treatment for the last 6 months, having sufficient cooperation to participate in the study, and voluntary participation. Patients were excluded from the study if they had any additional orthopedic and/or neurological disease affecting hand functions. All patients who met the inclusion criteria were informed about the study and provided a signed written consent form. After the patients were assessed by a blind assessor, the groups were assigned by a statistician according to age and gender. The assessor physiotherapist was unaware of which group the patients were assigned to. The patients were randomly separated into three groups as the intervention, conventional exercise, and control groups. The patients were aware of the interventions since they would perform the exercises themselves under the supervision of physiotherapists other than the assessor. All assessments were performed before the intervention and repeated at the end of the 8 weeks.
Intervention protocol
VR exercises, comprising 10 free games, were downloaded from LMC to a computer, then were performed for 30 minutes a day, 3 days a week for 8 weeks. The patients played the games via LMC on the computer under the supervision of a physiotherapist, using both their right and left hands. Rest breaks were taken as needed between the games, which involved flying balls and paper planes. While the games were being played, the physiotherapist provided verbal motivation to the patients.10,11 In the first 4 weeks, ball games were played for 30 minutes. It consisted of eight games in total. In the last 4 weeks, every three games (ball, plane, and helicopter games) were played for 10 minutes (Fig. 2). The games were repeated 5–6 times depending on their type, duration, and difficulty (Supplementary Data).

Treatment protocol.
Conventional exercise group
The patients in this group underwent a rehabilitation program consisting of hand stretching and strengthening exercises under the supervision of a physiotherapist. The rehabilitation program was implemented for 30 minutes a day, 3 days a week, for 8 weeks. 12 The exercises consisted of 5 minutes of wrist and finger range of motion, 10 minutes of stretching, and 15 minutes of strengthening with a ball and rubber band. Each exercise was repeated 10 times. After 4 weeks, the number of repetitions was increased to 15 (Fig. 2).
Control group
The patients with rheumatic disease in this group continued their routine drug treatments and did not participate in any exercise program. After the end of this study, these control group patients were enrolled in the LMC exercise program (Fig. 2).
Outcome measures
Disease activity score 28 (DAS 28)
The DAS 28, developed by Fransen and Van Riel in 2005, 13 evaluates swelling and tenderness in 28 joints including the proximal interphalangeal joint, metacarpophalangeal joint, wrist, elbow, shoulder and knee joints, erythrocyte sedimentation rate (ESR) value, and provides a global evaluation of the patient (VAS 0–100 mm). The DAS 28 value is calculated using the following formula: DAS28 = (0.56 × √ Number of Tender Joints) + (0.28 × √ Number of Swollen Joints) + (0.70 × Ln (ESR value)) + (0.014 × Patient global assessment). A higher overall score indicates high disease activity. 13
Hand grip strength measurement
Hand grip strength was measured using the Jamar hydraulic hand dynamometer (Sammons Preston, USA), which was developed by Bechtol in 1954. 14 Grip tests were performed in the standard position recommended by the American Association of Hand Therapists. The patient was seated in a position of 90°–20° hip and knee flexion, shoulder adduction, forearm neutral position, 90° flexion of the elbow, 0°−30° wrist extension, and 0°−15° ulnar deviation. The measurement was repeated three times, and the average value was recorded. 15
Fine grip strength measurement
Fine grip strength measurements were made using finger dynamometry (Pinchmetre-Sammons Preston, USA). Grip tests were performed in the standard position recommended by the American Association of Hand Therapists. Three different finger grasps were evaluated: (1) Fingertip grip strength, (2) Lateral grip strength, (3) Three point grip strength. The measurements were repeated three times, and the average value was recorded. 15
Jebsen-Taylor hand function test (JHFT)
This test, developed by Jebsen 16 to evaluate the effectiveness of treatment in hand injuries, consists of tasks that involve the grasp types commonly used in daily living activities and the speed of performing these tasks is evaluated. 17 Each stage of the test, which consists of seven substeps, was explained to the patients in detail before the tasks, which were then performed with both the dominant and nondominant hands. The time was recorded in seconds with a stopwatch.
Nine-Hole peg test (NHPT)
This test was developed by Kellor et al. 18 and standardized by Mathiowetz et al. 19 The device consists of a square platform and a storage box. There are nine holes in the square-shaped area (12.7 × 2 cm) and nine cylindrical pegs that fit these holes. During the test, the patient sits at the table with the 9-hole board, and the patient is asked to quickly take the nine pegs from the storage box, place them in the holes in random order, and quickly remove them from the holes without taking a break and place them in the storage box. The time taken to complete the task is measured in seconds with a stopwatch. The test is performed two times consecutively for both hands and the average result is taken. The total test score is calculated by averaging the scores for both hands.
Duruöz hand index (DHI)
It is a valuable test that was first developed to evaluate the hand functions of patients with RA, for which the validity and reliability has been proven in many diseases related to the upper extremity. 20 The test consists of 18 questions, scored on a Likert-type scale, providing a total score in the range of 0–90 points, with lower scores indicating better functional status. 21
Michigan hand outcome questionnaire (MHQ)
This questionnaire is a scale consisting of 57 different items in six sections. The items are scored on a Likert-type scale from 1–5 points, with 1 representing the most positive answer, and 5 the most negative answer. For each section, the total score is in the range of 0–100, and with the exception of the pain section, 0 represents the worst score and 100 represents the best score. In the pain section, a higher score indicates a higher level of pain. 22 Each of the six different categories in the scale is scored separately. 23
Statistical method
Sample size
The effect size obtained from the reference article was found to be moderate (d: 0.5). 24 As a result of the power analysis conducted, assuming that an effect size at approximately the same level (d = 0.48) could be obtained based on the results in the reference study, the minimum sample size was calculated to be 45 patients in total, using 0.05 alpha margin of error and 0.80 research power values. The study was completed with 45 patients in total, as 15 in each of the three groups.
Statistical analysis
Data obtained in the study were analyzed statistically using SPSS version 25 software (IBM SPSS Statistics; IBM Corporation, Armonk, NY, USA). Descriptive statistics of the data were calculated as mean ± standard deviation values. As a result of descriptive analyses, the conformity of the data to normal distribution was evaluated with the Shapiro-Wilk test. Intragroup comparisons were evaluated with the Paired-T Test for groups with normal distribution, and with the Wilcoxon Test for those with non-normal distribution. Differences between groups were compared with analysis of variance (ANOVA) if data showed normal distribution, and with the Kruskal–Wallis Test if the data distribution was not normal. The level of statistical significance was accepted as P < 0.05.
Results
Evaluations were made of 45 patients with a mean age of 52.24 ± 10.03 years, who presented at Antalya Training and Research Hospital and met the inclusion criteria, as 15 patients in each of the three groups. The sociodemographic characteristics (age, gender, etc.) and health-related data (disease duration, diagnosis, etc.) of the study participants were shown in Table 1 as mean and percentage.
Descriptive Statistics Regarding the Sociodemographic Characteristics of the Participants
LMC, leap motion controller; CE, conventional exercise group; BMI, body mass index; RA, rheumatoid arthritis; PsA, psoriatic arthritis.
In the intergroup comparisons, there was a significant improvement only in the intervention group according to the DHI scores after the intervention and also there was significant improvement in many subparameters of MHQ (hand function, daily living activities, pain and satisfaction) using for assessing hand function in both the intervention and conventional exercise groups (Table 2, P < 0.05).
Intragroup and Intergroup Comparison of Participants’ Evaluations of Disease Activity and Hand Functionality at Baseline and After the İntervention
*P < 0.05.
DAS28, Disease Activity Index-28; DHI, Duruöz Hand Index; MHQ, Michigan Hand Questionnaire; T.V., test value; LMC, leap motion controller; CEG, conventional exercise group.
In the intergroup comparisons, there was a significant improvement in hand and fine grip strength in the intervention group, and the intervention group was superior to the conventional exercise group in terms of three-point grip strength. There was a significance in only three point grip (fine) strength in conventional exercise group after the intervention (Table 3, P < 0.05).
Intragroup and Intergroup Comparison of Participants’ Grip Strength Evaluations at Baseline and After the İntervention
*P < 0.05.
LMC, leap motion controller; CEG, conventional exercise group.
In the intergroup comparisons, statistically significant improvements were detected in the intervention and conventional exercise groups for the dominant and nondominant side in JHFT for assessing hand function (Table 5). The intervention group was found to be superior to the control group in many subparameters of the JHFT (writing, turning cards, simulated feedings, moving light-heavy objects) and for both sides (dominant and nondominant) in the NHPT for assessing hand function (P < 0.05, Tables 4 and 5).
Intragroup and Intergroup Comparisons of Participants’ 9-Hole Peg Test Results at Baseline and After the İntervention
*P < 0.05.
LMC, leap motion controller; CEG, conventional exercise group.
Intragroup and Intergroup Comparisons of Participants’ Jebsen-Taylor Hand Function Test Results at Baseline and After the İntervention
*P < 0.05.
LMC, leap motion controller; CEG, conventional exercise group.
Discussion
This study is the first randomized controlled study in literature to have compared 8-week technology-based rehabilitation and physiotherapy and rehabilitation programs applied to patients with rheumatic disease with hand involvement. The effects of technology-based rehabilitation and physiotherapy and rehabilitation programs on hand functions and grip strength of individuals with rheumatic disease with hand involvement were examined in the study. The group that received a technology-based rehabilitation program showed significantly more improvement in functional subtests and both gross and fine grip strength compared to the control group. There was no superiority between the conventional exercise group and the technology-based exercise group.
A wide variety of exercises are used in hand rehabilitation for both disorders and functional disorders. Recently, technology in the form of virtual reality (VR)-based therapy has become an important rehabilitation tool used by physiotherapists. VR therapy refers to a broad class of interventions but can be broadly defined as technological interventions that change aspects of the physical world. 25 Microsoft Kinect, Nintendo Wii-Fit, and many more are among the VR devices currently available, but these do not primarily detect fine hand and hand movements, so will be of limited benefit to finger movements in hand rehabilitation. LMC is a low-cost, markerless motion capture device that tracks fine movements of fingers and hands without the use of data gloves or markers. The LMC device can track the movement of multiple fingers and the hands with submillimetric accuracy.26,27 Although there are few studies in literature on the use of LMC in hand rehabilitation, it has been reported that it can be used in upper extremity rehabilitation.26,28 In a pilot study conducted with the elderly, it was stated that LMC-based games could be used as a promising tool for hand rehabilitation. 29
In a study examining upper extremity functions using LMC in hand rehabilitation, positive improvements were noted in the Jebsen-Taylor hand function test, 9-hole peg test, and gross and fine grip strength evaluation in both the LMC and conventional exercise groups, with similar results in both groups. 11 Although the population group of that study consisted of children with different diagnoses and ages from those of the current study patients, the results were observed to be in parallel with the current study. In another study, hand functions and grip strength were evaluated using LMC in patients with hand stiffness, including rheumatic diseases. It was reported that functionality improved, and grip strength increased in both the conventional group and the group using LMC, and similar to the current study, no superiority was found between the groups. 24 In the current study, the LMC group was superior to the control group in terms of triple grip strength. This result can be considered to be very valuable in terms of patients being able to function in daily life, because a daily living activity that requires triple comprehension, such as writing, is one of the most skillful tasks performed on a regular basis. 30 In another study of the use of LMC in elderly patients, a significant increase was observed in hand functions evaluated using the Duruöz hand function test after the program. 31 In a study conducted using different evaluation methods from our study, it was thought that hand rehabilitation with LMC could help patients with hand burns increase finger range of motion, reduce wound thickness and improve hand function. 32 The current study results can be said to be compatible with the literature.
There were some limitations to this study, primarily that since there was only a single LMC device, the patients’ hands could not be operated bilaterally at the same time. Another limitation was that most of the patients included in the study were female. Finally, due to financial restrictions, only free-of-charge games suitable for the LMC device were used. Future studies can be planned to include gender homogeneity in the groups and games specific to the type of hand involvement of the patients.
Conclusions
Both technology-based rehabilitation and conventional hand exercises performed under the guidance of a physiotherapist were determined to have positive effects on the grip strength and hand functions of patients with rheumatic diseases with hand involvement. Additionally, the technology-based hand exercise program was superior to the traditional exercise group in terms of fine grip strength. Developing approaches that will maintain patients’ motivation for exercise during the treatment process may help increase and maintain these effects. Technology-based rehabilitation can be used as a feasible, safe, and effective method in the clinical setting.
Footnotes
Acknowledgment
The authors thank all patients who participated in the study.
Authors’ Contributions
S.Y.C.: Conceptualization (lead); methodology, investigation, review, and editing; writing—original draft. S.Y.: Methodology, investigation. M.D.: Investigation, software (lead); writing—review and editing (equal), formal analysis. G.S.U.: Investigation (equal). O.K.K.: Conceptualization (supporting), supervision, draft (supporting). A.A.: Supervision, data sources.
Author Disclosure Statement
The authors declared no conflict of interest.
Funding Information
This study supported financially by Scientific and Technological Research Council of Turkey with 123S872 project number.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.