
Abstract
The effectiveness of robot-assisted board games targeting older adults with mild cognitive impairment was investigated to improve their cognitive function, general self-efficacy, and life satisfaction and reduce depression. A quasiexperimental research design was adopted with 109 older adults from 8 long-term care facilities and day-care centers assigned to the experimental (n = 52) and comparison groups (n = 57). The experimental group underwent a 12-week cognitive training program. Both groups completed before-and-after and 3-month follow-up measurements for outcome variables, including cognitive function (scores of mini-mental state examination [MMSE] and Alzheimer’s Disease Assessment Scale Cognitive Subscale [ADAS-Cog]), depression, general self-efficacy, and life satisfaction. The data were analyzed using the generalized estimating equation (GEE). The program’s usability was assessed using the system usability scale (SUS). The GEE analyses revealed significant postintervention improvements in the experimental group’s MMSE, ADAS-Cog, depression, general self-efficacy, and satisfaction with life scores. These effects persisted for the 3-month follow-up. The mean SUS score was 87.50, indicating the feasibility of robot-assisted interventions among older adults. These findings confirmed that interactive robot-assisted board games can improve cognitive function, general self-efficacy, and life satisfaction and reduce depression among older adults. The administration of long-term care facilities or day-care centers can adopt robot-assisted board games as a training tool to supplement health promotion activities to prevent cognitive deterioration and enhance mental health among older adults.
Introduction
Mild cognitive impairment (MCI) is an intermediate state between cognitively intact individuals and those with dementia. 1 The spectrum of cognitive decline in older adults ranges from classification as normal cognitive decline with aging to subjective cognitive impairment (cognitive complaint with normal cognitive screening test) to MCI to dementia. 2 The Diagnostic and Statistical Manual of Mental Disorders defines MCI as a mild neurocognitive disorder. These are characterized by noticeable declines in cognitive function exceeding that of normal aging. 3 The estimates of progression rates to dementia are critical for prognosis and prevention. A meta-analysis indicated that the prevalence of MCI pooled from the 12 studies was 27% among rural dwellers, which differs by various countries, gender, and age groups. 4 A US study revealed an MCI prevalence of 22%, 5 whereas a Chinese study indicated it as 15.5%. 6 A specific treatment is yet to be devised for MCI. However, the overall risk may be reduced by employing evidence-based strategies and methods to manage cardiovascular and cerebrovascular risk factors. Moreover, nonbiological factors such as sufficient cognitive stimulus and activities are vital. 7
The cognitive training program is an evidence-based approach for nonpharmacotherapy prevention to delay progression from MCI to clinical dementia. A meta-analysis revealed that, in older adults, multicomponent training modules that train multiple cognitive abilities are more effective in cognitive function when compared with single-component training modules that target a specific cognitive ability.8–9 In cognitive interventions, the prefrontal cortex and parietal lobes are typically simulated on both sides of the brain. Core executive functions (working memory, inhibition, and cognitive flexibility) depend on the prefrontal brain regions, one of the most vulnerable areas to age-related decline. Therefore, training executive functions promotes cognitive and neural enhancements in old age. 10
Board games are effective training tools for improving cognitive functions. 11 Games and playing are characteristic of human nature and can improve older adults’ learning motivation. 12 The application of board games in intervention enables people to learn by playing, interacting with others, communicating and enhancing cooperation, exploring the external environment, and learning with interest. 13 Studies have revealed that playing board games benefits the brain health and cognitive function in patients with dementia.14–15 With rapid advances in artificial intelligence (AI), AI-enabled learning involving motion and sound effects is specific, flexible, and accommodates feedback. Thus, by enabling interactive and engaging learning experiences, learning content is made accessible, and participants’ sensory stimulation is increased. 16 Given our aging society, social robots have been developed to provide care to older adults with cognitive impairment and facilitate their independence and well-being. 17 A systematic review revealed that robot-assisted games with multiplayer gaming, including competitive, collaborative, and coactive modes, have emerged as a promising approach to increasing the motivation and effects of patients in rehabilitation therapy. 18
Technology-assisted game products should be designed to satisfy user requirements and expectations. According to the World Health Organization guidelines, programs for monitoring and evaluating digital health interventions should begin with questioning whether the intervention addresses identified requirements, including technical functionality and feasibility, followed by assessing user satisfaction. 19 Limited robot-assisted board games have been developed to prevent or delay the progression from MCI to clinical dementia. A robot-assisted cognitive intervention was developed in Korea comprising daily 60-minute sessions over 4 weeks, demonstrating improvements in the working memory of patients with MCI. 20 Meanwhile, a study in Italy used the humanoid robot NAO to train a memory program, reporting improvements in prose memory and verbal fluency. 21 Both studies suggest that further research in real-world settings is needed to understand fully the potential of robotics in clinical practice. However, other technology-based interventions for older adults with MCI could improve their cognitive function 22 and reduce depression. 23 Improvements in cognitive status may subsequently contribute to life satisfaction. 24 Enhanced cognitive function may reduce the risk of MCI-linked depression 25 and thus contribute to increased life satisfaction. 26 Due to program participation being critical, past studies have emphasized the role of self-efficacy, to which system usability contributes.27–28
Aimed at enhancing the MCI population’s well-being, this study investigated robot-assisted board games to improve cognitive function.
Methods
Research design, settings, and participants
A cluster randomized controlled trial (RCT) was conducted, following the CONSORT extension guidelines. 29 We received administrative support and approached 27 long-term care facilities and day-care centers in northern Taiwan. After explaining the study’s purposes and procedures, eight agreed to participate. They were then randomly assigned to either the experimental or comparison group using a selection method that ensured unbiased allocation. In each facility/center, the number of residents with freedom of movement ranged from 15 to 40. Most of these facilities/centers have prior experience collaborating with schools, allowing students to practice elderly care on-site. All the participants in the facilities/centers received the same intervention and needed to complete three assessments. The research team did not inform the data collectors which participant was in the experimental group or the control group.
The selection criteria for participating were (1) residents with mini-mental state examination (MMSE) scores from 18 to 23, (2) individuals’ willingness to comply with verbal instructions, and (3) to avoid influencing the robot’s operation, no severe chronic diseases such as a stroke. Although this process secured an equal number of facilities/centers for both groups, some older participants signed up but then dropped out, disequalizing the group numbers. Common reasons for refusal included lack of time to participate in 12 activities, unwillingness to continue cognitive training for 12 weeks, unwillingness to fill out questionnaires, and concerns about poor performance in the board games. In addition, older people with inconvenient hand movements, inability to operate robots, and inability to understand instructions or execute actions based on instructions were also excluded from the study. In total, 52 and 57 members participated in the study, respectively, in the experimental and comparison groups (Fig. 1). Using G-Power 3.1.9.7 software, we calculated the sample size using a two-tailed test, with a medium effect size of 0.5, an alpha of 0.05, and a power of 0.8. This confirmed needing a minimum of 34 participants per group.
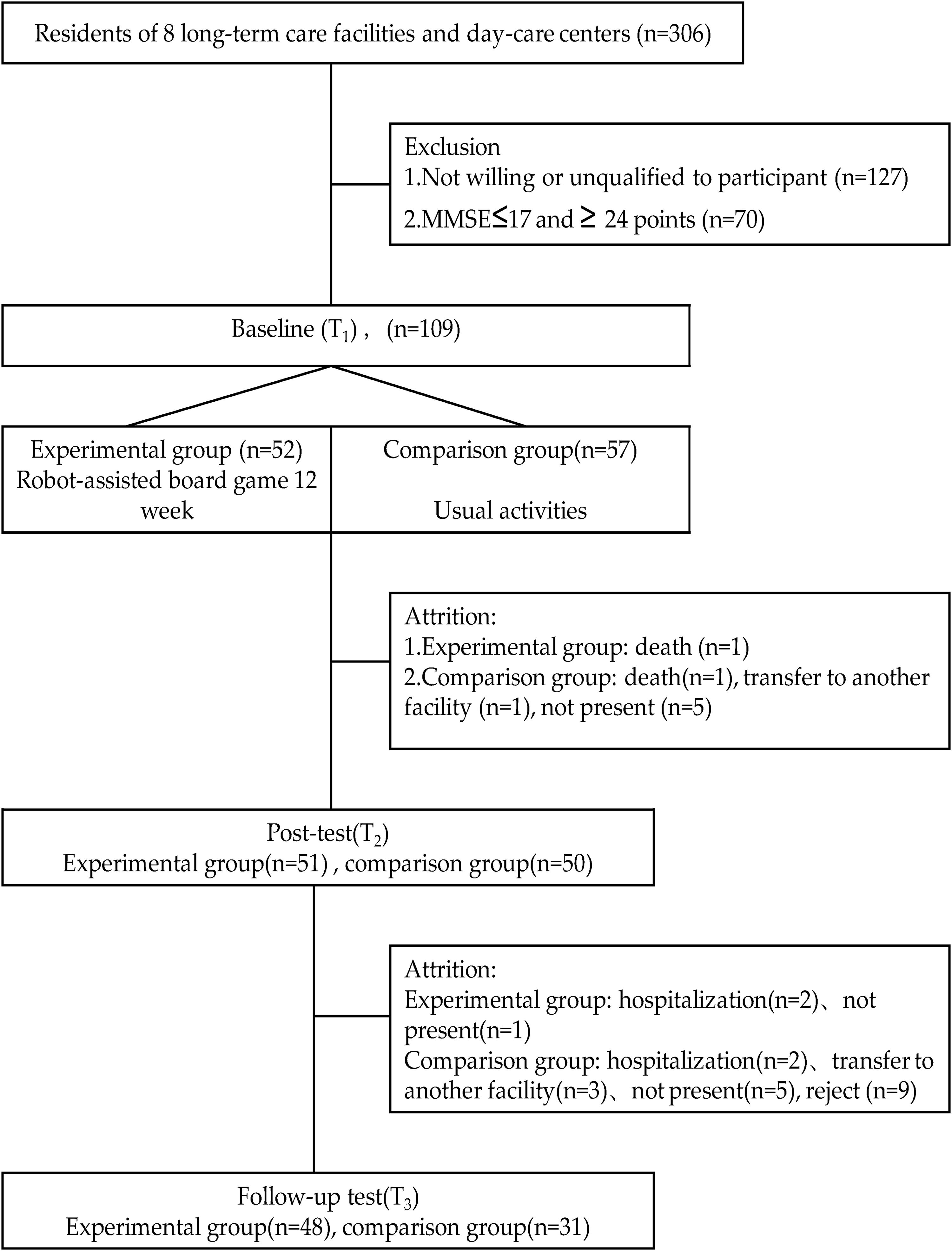
Flowchart of participant enrollment intervention and measurements.
The purpose, procedure, and relevant protections of the study were explained to all participants, and their informed consent was obtained. Only the participants in the experimental group received the intervention. However, due to the Institutional Review Board’s requirements, the comparison group also received the intervention after the study was completed. Assigning the dates for interventions at facilities/centers was at the administrators’ discretion.
Measurements
MMSE
The intervention effect is critical when designing a cognitive training board game with a plausible framework. The MMSE is an 11-item screening test that quantifies the severity of cognitive impairment and documents change over time. It examines registration (repeating named prompts), attention and calculation, recall, language, orientation, and ability to follow simple commands. The total score ranges from 0 to 30. 30
Alzheimer’s Disease Assessment Scale Cognitive Subscale
Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) includes a two-part scale: one measures cognitive functions and the other noncognitive functions, such as mood and behavior. The scale comprises 11 items, including word recall, naming objects and fingers, following commands, constructional praxis, ideational praxis, orientation, word recognition, remembering test directions, spoken language, and comprehension. The total score ranges from 0 to 70. 31 In this study, Cronbach’s α coefficient on ADAS-Cog was 0.77.
Geriatric Depression Scale Short-Form
To identify symptoms of depression, the Geriatric Depression Scale Short-Form (GDS-15) screening tool was used to establish how participants felt in the preceding week.32–33 Scores above 10 suggest further checks for a depressive diagnosis. Of the 15 items, 10 indicated depression when answered positively, whereas question numbers 1, 5, 7, 11, and 13 indicated depression when answered negatively. Cronbach’s α coefficient for the GDS-15 was 0.73 in this study.
Satisfaction with Life Scale
The Satisfaction with Life Scale (SWLS) focused on assessing global life satisfaction among participants. 34 SWLS contains five items scored on a 1–7 Likert scale with a higher score indicating a higher level of life satisfaction. In this study, the Cronbach’s α coefficient for the SWLS was 0.87.
New General Self-Efficacy Scale
The eight-item New General Self-Efficacy Scale (NGSE) scale assesses how much people believe they can achieve their objectives despite difficulties. 35 Items were scored on a Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree), with a higher score indicating a higher level of self-efficacy. A sample item is “Even when things are tough, I can perform quite well.” In this study, the Cronbach’s α coefficient for the NGSE was 0.96.
System Usability Scale
System Usability Scale (SUS) is a 10-item scale, with items scored on a Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). It is widely used for measuring the usability of educational technology. 28 The SUS provides a single score on a scale of 0 to 100, offering a subjective measure of usability. For positive items (1–5), each score was adjusted by subtracting 1 point, while for negative items (6–10), 5 points were subtracted. After adjusting each item’s score, all scores were summed and then multiplied by 2.5 to derive the total score. According to Hyzy et al., an average SUS score of 68 is considered the minimum threshold for product qualification. 36
Board game design and development
Based on the aspects of MMSE and ADAS-Cog, six topics were developed for the board game, including orientation (people, time, and place), attention and calculation, short-term memory (recall), language skills, ability to understand and follow instructions, and visuospatial abilities (visual and spatial relationships between objects). The six topics, descriptions, and corresponding aspects of MMSE and ADAS-Cog are contained in the Supplementary Table S1, whereas the example photos are shown in Table 1. Five experts in health education, nursing, elderly care, and clinical care evaluated the board game. The research team introduced modifications based on their suggestions. The board game set comprised the following categories: (1) a cardboard map, (2) 32 general cards with QR codes, each card containing 10 questions, (3) chance and destiny cards, (4) chips, (5) game pieces, (6) dice, and (7) a robot named Kebbi. Players scan the QR codes on the cards to trigger the robot to display questions or training tasks. Players who answer correctly receive reward points, whereas incorrect answers elicit encouragement from the robot to try again.
The Six Major Units of the Game
Intervention procedure
Four members of the research team received training as game facilitators. The experimental group underwent 3 months of robot-assisted board game training, that is, 12 once-weekly 60-minute sessions. The training occurred in the long-term care facility (LTC) where the residents live.
Figure 2 presents a series of photos showing how the robot-assisted board game proceeds. Research staff arranged the board game props and robots on tables and introduced the game and its rules, and the robot’s operations were demonstrated to the attendees. One of the six topics was selected for the day’s cognitive training.

Playing process of robot-assisted board games.
One robot can be paired with 2–5 players, each choosing and naming their own game piece. Players roll dice to determine the number of spaces to advance, and correctly answering questions earns reward points. Players are encouraged to cooperate to answer questions or complete cognitive training tasks. After playing for 1 hour, the reward points were calculated. The player with the highest points is announced and appreciated by other players and staff.
Statistical analyses
Descriptive analyses were performed for demographic and outcome variables. A two-tailed χ2 and t test were performed to compare the differences between the experimental and comparison groups. A generalized estimating equation (GEE) was used to investigate the effects of the time point, group, and their interaction on outcome variables. GEE analyses enabled an understanding of the patterns of change and their effects at both the individual and group levels. 37 SPSS (version 23.0; IBM Corp) was used for the statistical analyses.
Results
The mean age and standard deviation (SD) of the experimental and comparison groups were 82.56 (SD = 7.88) and 81.44 (SD = 7.43), respectively. The experimental and comparison groups evidenced no statistically significant differences in the demographic and outcome variables (Table 2).
Demographic and Outcome Variables
ADAS-Cog, Alzheimer’s Disease Assessment Scale Cognitive Subscale; GDS, Geriatric Depression Scale Short-Form; MMSE, mini-mental state examination; NGSE, New General Self-Efficacy Scale; SD, standard deviation; SWLS, Satisfaction with Life Scale.
Due to high dropouts in the comparison group, at follow-up, the differences between the noncompleters and completers were analyzed. Differences in the age, gender, year in education, partner status, comorbidity, MMSE, ADAS-Cog, GDS-15, SWLS, and NGSE variables were compared using χ2 and independent t tests. No significant differences were observed (P > 0.05).
Figure 3 shows the changes in outcomes across the pre-, post-, and 3-month follow-up assessments. Significant postintervention improvements in the experimental group were indicated by comparative GEE analyses of five outcome variables, including MMSE (estimate = 1.74, P < 0.001), ADAS-Cog (estimate = −4.33, P < 0.001), GDS-15 (estimate = −1.20, P < 0.018), SWLS (estimate = 3.38, P = 0.001), and NGSE (estimate = 3.02, P < 0.001; Table 3). Comparative GEE analyses indicated that the experimental group exhibited significant intervention effects between the pretest and 3-month follow-up regarding MMSE (estimate = 1.35, P = 0.002), ADAS-Cog (estimate = −3.60, P < 0.001), GDS-15 (estimate = −1.59, P = 0.007), SWLS (estimate = 3.64, P = 0.002), and NGSE (estimate = 2.86, P = 0.006).
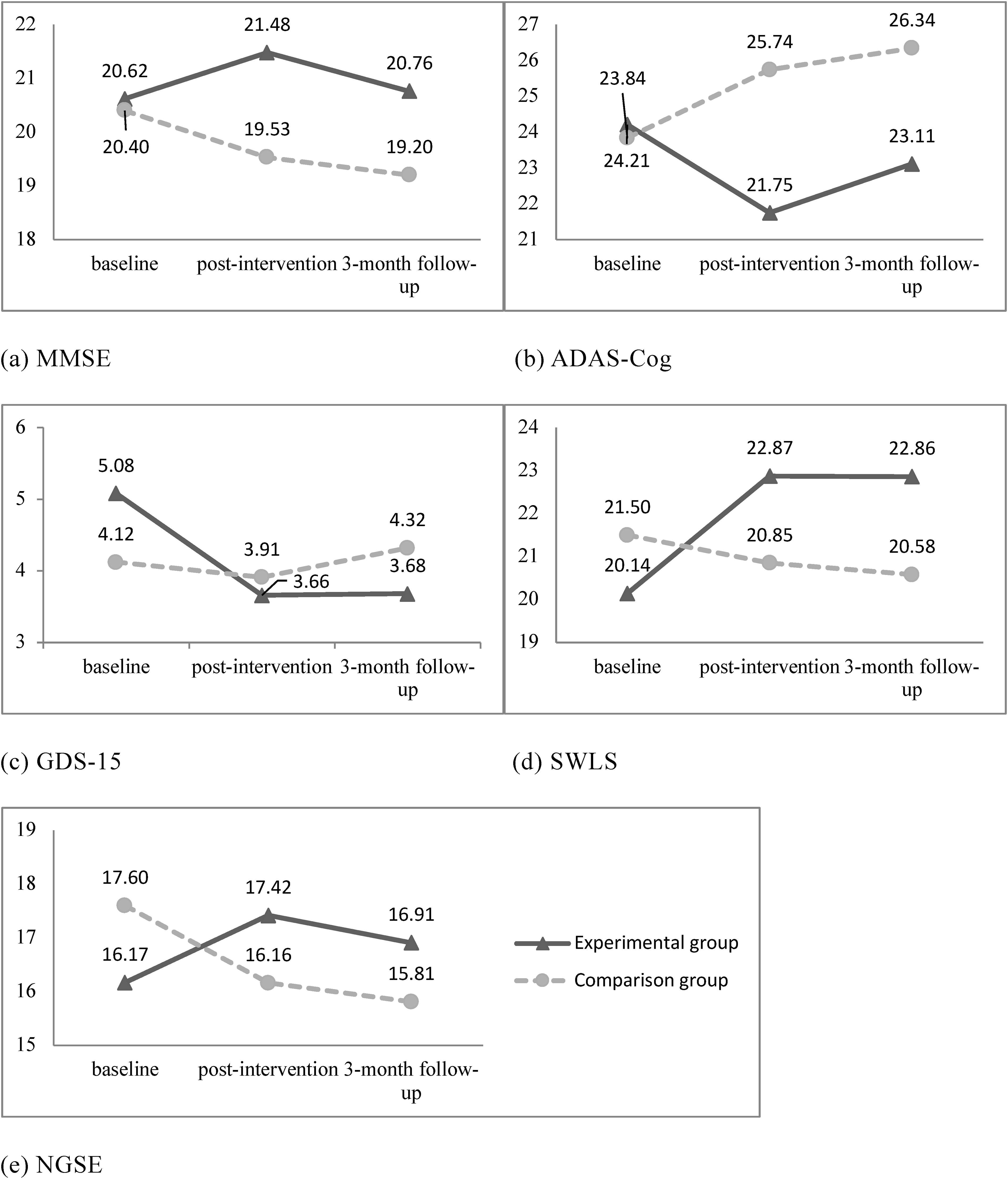
The changes of outcomes in the pre-, post-, and follow-up assessments. ADAS-Cog, Alzheimer’s Disease Assessment Scale Cognitive Subscale; GDS, Geriatric Depression Scale Short-Form; MMSE, mini-mental state examination; NGSE, New General Self-Efficacy Scale; SWLS, Satisfaction with Life Scale.
Results of the Generalized Estimating Equation Analyses of the Five Outcome Variables
ADAS-Cog, Alzheimer’s Disease Assessment Scale Cognitive Subscale; GDS, Geriatric Depression Scale Short-Form; GEE, generalized estimating equation; MMSE, mini-mental state examination; NGSE, New General Self-Efficacy Scale; SE, standard error; SWLS, Satisfaction with Life Scale.
Reference group: comparison group.
Reference group: time (baseline).
Reference group: group (comparison) × time (baseline).
The mean SUS score was 87.50 ± 4.61, which indicates that the participants found the system usable.
Discussion
Our findings support the effectiveness of robot-assisted board games targeting older adults with MCI to improve their cognitive function, general self-efficacy, satisfaction with life, and depression. Most participants, with a mean age of over 80 years, had never played with a robot. However, the high SUS scores support the feasibility of conducting robot-assisted interventions among older adult populations. While the previous study in school-age children found that gamification techniques with board game interventions may not be as effective as without gamification, our findings suggest that gamification may be more effective among older adults. 38 This difference could imply that gamification elements are more engaging or beneficial for older populations.
Favorable outcomes in the experimental group were linked to the board game play arrangements. One robot can be paired with 2–5 players. Staff member facilitators would assist players in operating the robot when necessary and encourage players to discuss finding the best answers. The board game questions and tasks were based on MMSE and ADAS-Cog, thus familiarizing the players with the question patterns. Regarding the MMSE and ADAS-Cog scores, participants’ cognitive functions significantly improved after the 12 sessions. A prior study demonstrated that board games can improve visual working memory and that social interaction may amplify these cognitive benefits. 39 In addition, board games can be adapted for individuals with varying levels of cognitive function, including those with moderate dementia, by adjusting the difficulty level of the game. 40 A Spanish study observed a similar effect where game-based interventions were found to be effective in maintaining or enhancing cognitive processes among healthy older adults. 41 Such robot-assisted gameplay could further enhance cognitive engagement, providing a personalized, adaptable experience that encourages sustained participation.
Players’ feedback indicates that cooperative gameplay, rather than competition, improves depression and life satisfaction. Activities fostering social interaction can help reduce depression and perceived social isolation, enhancing life satisfaction among older adults.42–44 Socializing may lead to social cohesion and personal satisfaction resulting from performed social activities and interactions.45–46 Interestingly, such feedback toward game playing is less common among adolescent players.47–48 More research is needed to clarify the benefits of competitive games for different age groups.
Bandura proposed four sources of self-efficacy: mastery experiences, vicarious experiences, verbal persuasion, and physiological and affective states. 49 The experimental group participants underwent 12 cognitive training sessions and gradually familiarized themselves with the robot’s operations and question patterns, thus affording a sense of mastery. Participants had the opportunity to answer their questions and observe each other responding, which helped them gain vicarious experience. After passing the question challenges, participants received feedback and praise from the robot and group members, which may have strengthened their positive affection, thus improving perceptions of self-efficacy.
This research involved integrating gamification and using assisted robots to play board games. Gamification could increase user motivation and enhance engagement during the learning process. 50 Assisted robots have been gradually adopted as an innovative intervention tool for older adults with cognitive impairment. Pooled results of an article of systematic review and meta-analysis indicated that social robots can reduce agitation and anxiety and improve the quality of life for older adults. 51 The authors suggested that older people with higher cognitive capabilities engaged more actively than those with lower capabilities. The participants of this study all suffered MCI, and thus, subgroup analysis was not performed. To overcome this, more diverse groups are needed to clarify how using robots in activity engagement improves cognitive capabilities.
Iizuka et al. suggest that playing face-to-face with other people could increase cognitive benefits compared with the same task on a device. 39 Our study indicates that human–robot interaction and playing face-to-face with others could significantly increase cognitive benefit. The finding adds what could be another intervention mode for board games designed for older adults. Moreover, because this study took place during the COVID-19 pandemic, data collection was challenging due to the participants’ anxieties, which led to lower participation rates. During the third measurement, several participants in the comparison group declined to complete the third measurement since they had not received interventions and had twice completed the same questionnaire. This caused disparities between the experimental and comparison groups at the third assessment.
Limitations and future studies
The study encountered several limitations. First, it could not distinguish between intervention efficacy resulting from group or individual interactions. The research findings must be interpreted with caution. Second, the study did not apply an RCT design, which allows external generalizability. Similar future studies adopt an RCT design. Previous studies have revealed that individual interactions with robots were more acceptable and applicable when personalized engagement was possible, as in this study.52–53 Peer support, formed through mutual assistance in answering questions, may have contributed to the intervention’s effects. Future research should consider adding a social support component to enhance motivation and intervention effectiveness. The small, easy-to-operate, child-like robots made cognitive training engaging, differing from formal assessments by medical staff. Future studies could apply robot-assisted board games to design cognitive training programs for the elderly.
Conclusion
Robot-assisted board games, designed based on the six domains of the MMSE and ADAS-Cog, have been shown to benefit older adults with MCI, including improvements in cognitive function, general self-efficacy, life satisfaction, and depression. It is recommended that administrators of long-term care facilities incorporate these games into health promotion programs to help reduce the risk of cognitive and mental decline among elderly residents.
Ethical Consideration
The local IRB, Tri-Service General Hospital Institutional Review Board (C202105210), approved the study and all participants gave informed consent. The data were identified by numbers alone; therefore, participant identity and the collected information were not associated, thereby ensuring anonymity. The data sets generated or analyzed in this study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors thank all the participants for their time and commitment. This article was subsidized by the National Taiwan Normal University, Taiwan, ROC.
Authors’ Contributions
J.L.G., C.M.H., and L.C.L. were responsible for the study conception and design. J.L.G., L.C.L., F.H.L., and L.T.L. provided administrative, technical, and material support. L.C.L., J.Y.L., C.M.H., and J.L.G. performed data management and statistical analysis. All authors were responsible for the drafting of the article. All authors read and approved the final article.
Author Disclosure Statement
The authors declare no conflicts of interest and confirm that there are no competing financial interests.
Funding Information
This work was supported by the National Science and Technology Council, Taiwan (Grant number NSTC 1112622-H-003-005).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.