
Abstract
Aim: One of the main problems concerning repeated spontaneous miscarriage (RSM) is the etiological diagnosis. The relation of thrombophilia to RSM is a matter of debate. In this case-control study, we determined the percentages of three thrombophilic mutations (factor V leiden, prothrombin, and methylenetetrahydrofolate reductase) amongst 20 cases with RSM and 20 control normal parous women. Results: There were high statistically significant increases in the number of cases with factor V, prothrombin, and methylenetetrahydrofolate reductase gene mutations compared with normal control and the percentage of multiple gene mutations was higher than single gene mutation. Conclusion: The prevalence of thrombophilic mutations is higher in cases of RSM than control.
Introduction
R
Thrombophilia refers to any persistent hypercoagulable state that is associated with increased risk of thromboembolism. It may be genetically determined, acquired, or both (De-Sweet, 2002).
Thrombophilia, which involves interactions between inherited and acquired risk factors, has been suggested as a possible cause of RSM (Bauduer and Lacombe, 2005). The most common types of hereditary thrombophilia are factor V leiden (FVL), prothrombin (PTH), and methylenetetrahydrofolate reductase (MTHFR) genes mutations, but these are usually undiagnosed because most carriers are asymptomatic (Kovalevsky et al., 2004).
Thrombosis in decidual vessels is believed to be one such cause, leading to intrauterine growth retardation, fetal death, and possibly RSM (Carp et al., 2002).
Thrombophilia has been recently implicated in early pregnancy loss by impairing the initial vascularization process occurring at implantation, which is necessary for successful pregnancy (Azem et al., 2004; Kujovich, 2004).
With the identification of genetic risk factors, there has been synergistic amplification of thrombotic risk when there is an abnormal mutant gene (e.g., FVL) plus an environmental issue (e.g., pregnancy). Current understanding indicates that a combination of risk factors, including multiple inherited thrombophilic defects associated with secondary hypercoagulable states, have a particularly strong association with adverse pregnancy outcome (Kutteh and Triplett, 2006).
The aim of our study was to clarify the association between mutations in thrombophilic factor genes (FVL, PTH, and MTHFR genes) and unexplained RSM.
Materials and Methods
Patients
Between January 2008 and June 2009, 20 consecutive women attending the Obstetrics and Gynecology Department, Benha University Hospital, complaining of history of spontaneous repeated miscarriage were recruited to this study. A control group of another 20 parous, age-matched women with no history of miscarriage were recruited from postnatal wards. Exclusion criteria were a previous history of thrombosis, pregnancy at the time of investigation, use of oral contraceptives, and any other known cause of miscarriage, such as abnormal parental karyotype, diabetes mellitus, abnormal thyroid function, abnormal hysterosalpingogram (anatomical abnormalities, intrauterine adhesions, and cervical incompetence), abnormal serum prolactin and plasma progesterone levels, luteal phase defect, toxoplasmosis, antinuclear factor, or antiphospholipid antibodies. All individuals gave informed consent to participate in this study.
Methods
Venous blood (5 mL) was obtained from each subject and placed immediately into sterile vaccutainer tubes containing EDTA and then the sample was divided into sterile Eppendorff tubes and stored at −80°C until molecular study of the thrombophilic gene mutations.
The detection of mutation in factor V (FV), PTH, and MTHFR genes was based on the reverse-hybridization principle. The assay covered the following three mutations: FV (G1691A), PTH (G20210A), and MTHFR (C677T) (HVD Strip Kit; HVD Life Science).
DNA isolation was according to the protocol of Sambrook et al. (2001)
The extracted DNA concentration was confirmed through measurement in a UV spectrophotometer, and the readings were taken at wavelengths of 260 and 280 nm. The readings at 260 nm allowed calculation of nucleic acid in the sample. An optical density of 1.00 corresponds to ∼50 μg/mL for double-stranded DNA and 40 μg/mL for single-stranded DNA. The ratio between the readings at 260 and 280 nm (OD260/OD280) provides an estimate of the purity of the nucleic acid. Pure preparations of DNA have OD260/OD280 values of 1.7 and 2.0, respectively. If there is contamination with protein or phenol, the OD260/OD280 is significantly <1.7, and if there is contamination with RNA, the OD260/OD280 is significantly >2.0 (Haque et al., 2003).
Polymerase chain reaction amplification according to the protocol of Sambrook et al. (2001), was performed in a single multiplex reaction using biotinylated primers
All polymerase chain reaction reagents and DNA templates were kept refrigerated while all steps were performed until start of the thermal cycling program, using G-storm thermocycler.
Amplification products of FV, PTH, and MTHFR genes were also confirmed by gel electrophoresis (e.g., 3% agarose gel). The bands were expected to be seen at 173, 202, and 223 bp.
Hybridization (Qublan et al., 2005), performed at 45°C in a thermoshaker plate
In our study, hybridization of amplified products to a test strip that contained allele-specific oligonucleotide probes immobilized as an array of parallel lines was used, instead of using radioactive probes. The bound biotinylated sequences were detected using streptavidin-alkaline phosphatase and color substrates.
Color development was performed at room temperature
One milliliter of conjugate solution was added and incubated for 15 min at room temperature on a shaker. Then, 2 mL wash solution B was added and incubated for 5 min at room temperature on the shaker. After that, 1 mL color developer was added in each lane and incubated for 15 min at room temperature in the dark on the shaker. A purple color appeared upon positive reaction.
Interpretation of results
The genotype of a sample was determined using the enclosed collector sheet.
A positive reaction of the uppermost control line indicated the correct function of conjugate solution and color developer. This line always stained positive.
For each polymorphic position, one of the following staining patterns was obtained:
Wild-type probe only: normal genotype.
Wild-type and mutant probe: heterozygous genotype (carrier person).
Mutant probe only: homozygous mutant genotype (affected person).
Figure 1 shows the wild and mutant probes for each of the three thrombophilic genes on test strip design.
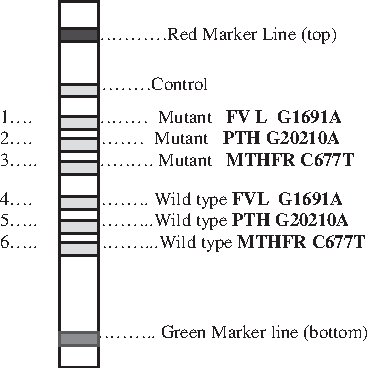
Wild and mutant probes for each of the three genes on test strips.
Statistical analysis
The results are presented as means ± standard deviation and percentages. Comparisons of categorical variables were made between cases and controls using chi-square test.
The Statistics Package for Social Sciences (SPSS) and Microsoft Office Excel were used for data processing and analysis. Differences were considered as statistically significant for a p-value of <0.05.
Results
Our study was performed on 20 women who had RSMs and 20 healthy women as a normal control group for detection of mutation in the three thrombophilic genes, FV, PTH, and MTHFR.
Table 1 contains a description of the clinical data of the RSM cases and the normal control group. These data include maternal age, previous live births, and family history of RSM.
RSM, repeated spontaneous miscarriage.
Table 2 shows that there are statistically significant increases in the percentages of cases with FV, PTH, and MTHFR gene mutations compared with the normal control group (70%, 65%, and 70%, respectively; p < 0.001 for all).
p < 0.001, high significant.
FV, factor V; PTH, prothrombin; MTHFR, methylenetetrahydrofolate reductase.
Table 3 shows that there are statistically significant increases in the percentages of cases with heterozygous and homozygous mutations in FV gene (heterozygous 60% and homozygous 10%), PTH gene (heterozygous 35% and homozygous 30%), and MTHFR gene (heterozygous 45% and homozygous 25%), when compared with normal controls (p < 0.001 for all).
p < 0.001, highly significant.
Table 4 shows that there are high statistically significant increases in the percentages of cases with single (20%) and multiple gene mutations (65%) when compared with normal controls (p < 0.001 for all).
p < 0.001, highly significant.
Discussion
Although several medical causes have been established, up to 50% of cases of RSM remain unexplained after standard gynecological, hormonal, and karyotypic investigations (Lissalde-Lavigne et al., 2005). Acquired and inherited thrombophilia factors are possible causes of RSM (D'Uva et al., 2008).
Single-nucleotide polymorphisms of the genes coding for coagulation factors are the causes of congenital thrombophilia, which might lead to early RSM and fetal loss in advanced pregnancy. The most frequent reasons of thrombophilia are gene mutations in FVL (G1691 A), PTH (G20210A), and 5, 10-MTHFR (C677T) (Agnieszka et al., 2008).
Our data showed significant increases of allele frequency as well as homozygosity and heterozygosity of FVL gene in women with unexplained RSMs when compared with normal controls. Many reports in the literature (Foka et al., 2000; Zammiti et al., 2006; Ivanov et al., 2009) have been in agreement with our study. On the other hand, Murphy et al. (2000) and Jivraj et al. (2006) showed a nonsignificant difference in FVL allele frequency between women with unexplained RSM and controls. Our finding may be explained by Dizon-Townson et al. (1997), who reported that microthrombi in the placental vasculature of future pregnancies were found to be a common finding among women with RSM. Also, they found that fetal carriage of FVL was associated with histologically proven placental infarction. Moreover, Burton et al. (1999) suggested that, before 8 weeks gestation, the maternal arterial connections with the intervillous space are restricted to tortuous networks, following which direct channels of communication are established, which are initially of small caliber but later become delineated by the end of first trimester. This suggests that thrombosis of the placental vasculature may lead to first-trimester RSM.
After that, Kujovich (2004) reported that mutation in the FV gene increases thrombin generation, with a four- to eightfold increased risk of thrombosis in heterozygous mutation and an 80-fold increased risk in homozygous mutation, which leads to vascular placental insufficiency that has been suggested as a potential cause of early RSM.
Another possible prothrombotic risk factor is PTH mutation. In the case of PTH, our study showed a significant increase in allele frequency as well as homozygosity and heterozygosity of PTH gene mutation in women with unexplained RSM when compared with normal controls. Our results concurred with those of Foka et al. (2000), Pihusch et al. (2001), and Ivanov et al. (2009). Our results may be explained by the fact that the PTH G20210A mutation was associated with a higher PTH clotting activity and a two- to sevenfold increase in risk of venous thrombosis, which may lead to miscarriage (Ercan et al., 2008).
In the study on MTHFR, our results showed a significant increase of allele frequency as well as homozygosity and heterozygosity of the MTHFR gene in women with unexplained RSM when compared with normal controls.
These findings were in agreement with those of Nelen et al. (2000), Ogasawara et al. (2000), and Unfried et al. (2002). The finding regarding MTHER may be explained by Berry et al. (1995), who mentioned that MTHFR mutation homozygosity might predispose to a thermolabile variant of the MTHFR enzyme, with 50% of normal activity, which in turn explains hyperhomocysteinemia, which may lead to structural and neurological effects on the fetus, causing fetal loss.
In the case of multiple gene mutations, our results showed a significantly increased prevalence of multiple thrombophilic gene mutations (of FVL, PTH, and MTHFR C677T) in women with RSM compared with the normal control group.
The concept of multiple gene mutations as a risk factor for RSM has been supported by many authors (Coulam et al., 2006; D'Uva et al., 2008; Vora et al., 2008), but disagreed by others (Carp et al., 2002; Jaslow et al., 2010).
The role of multiple gene mutations may be explained by uncontrolled and enhanced coagulation in the intervillous spaces of the placenta, which may induce fibrin deposition within the fetal circulation that could lead to fetal stem vessel thrombosis, placental infarction, and miscarriage (Lissalde-Lavigne et al., 2005).
Moreover, as several factors interact to create thrombosis, the action of thrombophilic factors during placentation may become amplified, thereby giving rise to modifications in placental circulation and subsequent RSM. The bottom line for the study is that multiple thrombophilic gene mutations and/or single gene mutations are risk factors for recurrent miscarriage.
These results emphasize the role of thrombophilia as a cause of RSM, which remains a common complication of pregnancy, in order to establish a possible protocol that supports the etiological diagnosis of RSM associated with thromboprophylaxis of these patients.
However, prospective longitudinal study of acquired thrombophilia is recommended. Study of other congenital thrombophilic factors is also recommended.
Footnotes
Disclosure Statement
All authors disclose that there are no commercial associations that might create a conflict of interest in connection with this manuscript.