
Abstract
Background: Pathogenic mutations in leucine-rich repeat kinase 2 (LRRK2; PARK8) encoding dardarin, implicated in patients with autosomal dominant and sporadic Parkinson's disease (PD) among different ethnic groups (Ashkenazi Jews, North African Arabs, Basques) might be of some help in diagnostic screening and genetic counseling. Aim of the Study: We investigated the seven common mutations spanning exons 31, 35, and 41 reported in the LRRK2 gene among Eastern Indian patients with PD. Methods: Mutations R1441G, R1441C, R1441H, G2019S, Y1699C, I2020T, and I2012T were screened in 320 individuals (PD, 150 and controls, 170) by direct sequencing. Results: We did not observe any of these abovementioned mutations in our studied individuals. Conclusion: We conclude that these mutations are rare causes of PD in the Eastern Indian population and, therefore, of little help for genetic counseling and diagnostic purposes.
Introduction
A
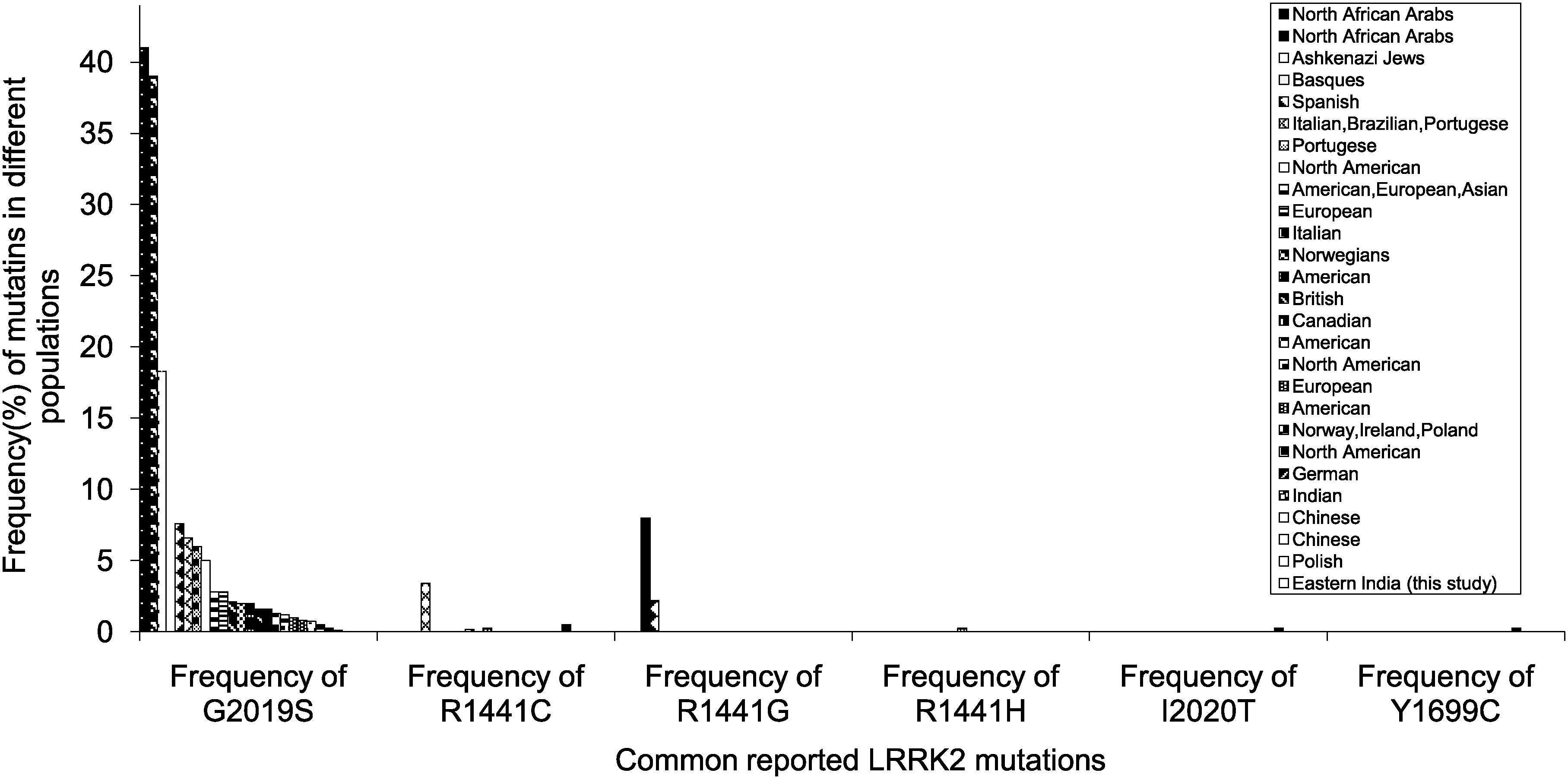
Reported frequencies of common reported leucine rich repeat kinase 2 (LRRK2) mutations in different populations.
Despite extensive studies on the molecular bases of PD in different population groups, very little information is available regarding the molecular pathogenesis of the disease among Eastern Indian patients with reference to this gene. A single report has demonstrated the absence or rarity of common LRRK2 mutations in North Indian patients (Punia et al., 2006). To develop a comprehensive mutation screening of the eastern part of India, we evaluated seven commonly reported pathogenic mutations. To our knowledge, this study is the first report on screening these seven common mutations of LRRK2 gene in the Eastern Indian population.
Subjects and Methods
Collection of patient samples
The base population recruited for this study is patients with PD visiting the Movement Disorder Clinic of Calcutta Medical College and Hospital (CMC) National Neuroscience Centre (NNC), Kolkata, India, from March 1, 2007 to December 23, 2009. Clinical data and a detailed family history of each patient were collected with the help of collaborating clinicians after physical and neurological examination by two independent consultant neurologists. Ethical approval of the research project using human subjects was obtained from the Institutional Ethical Committee of Anthropological Survey of India, Ministry of Culture, Government of India and National Neurosciences Center (collaborating hospital). Hospitals such as CMC and NNC are the main referral centers for cases related to movement disorders and are situated in the heart of Kolkata city, West Bengal. We have meticulously selected only those patients whose ancestors were residents of Eastern India. The demographic data (name, age, address, place of inhabitation, occupation, family pedigree, educational status, monthly income, occupation/professional status of subject during his/her life time, residence area [rural/urban], etc.) was collected by health professionals and epidemiologists.
Case definition
All the cases had to meet the following symptoms at the time of diagnosis: (1) the presence of at least three of the following signs: resting tremor, cogwheel rigidity, bradykinesia, and postural reflex impairment, at least one of which must be either rest tremor or bradykinesia; (2) no suggestion of a cause for another parkinsonian syndrome such as drugs, trauma, brain tumor, or treatment within the last 12 months with dopamine blocking or dopamine depleting agents; and (3) no atypical features such as prominent occulomotor palsy, cerebellar signs, vocal cord paresis, severe orthostatic hypotension, pyramidal signs, amyotrophy, or limb apraxia. Clinical stage of the disease was evaluated according to the classification of Hoehn and Yahr (1967).
The control group consisted of patients' spouses and other healthy community-based, age-, sex-matched volunteers residing in the same ethnic background as the patients with PD. None of the control subjects had diagnosable neurological disorders.
Collection of blood samples and genomic DNA preparation
Approximately 5 mL peripheral blood samples were collected in BD Vacutainer K2 EDTA (6 mL) with written and informed consent from patients with PD, their family members, and from normal individuals as controls. Genomic DNA was prepared from fresh whole blood by using the conventional phenol-chloroform method (Sambrook and Russel, 2001). Genomic DNA was dissolved in TE (10 mM Tris-HCl and 0.1 mM EDTA, pH 8.0).
Polymerase chain reaction
Polymerase chain reaction (PCR) was carried out to amplify exons and adjacent flanking region in a total volume of 10.0 μL containing 40-100 ng genomic DNA, 0.4 μM of each primer, 0.2 mM of each dNTP, 0.5-1.5 mM of MgCl2 (as appropriate), and 0.5 unit of Taq polymerase (Invitrogen, Carlsbad, CA) in a Thermocycler (GeneAmp-9700; PE Applied Biosystems, Foster City, CA). Annealing temperature is calculated based on Tm of the primer pairs. The primers (Table 1) used to amplify the LRRK2 exons (Nos. 31, 35, and 41) containing R1441C, R1441G (4321C>G), R1441H, Y1699C, G2019S (6059T>C), I2020T (6055G>A), and I2012T (T6044C) mutation have been previously reported (Berg et al., 2005). PCR-amplified DNA fragments were analyzed on 2% agarose gel and visualized by ethidium bromide staining.
Mutation and polymorphism detection
DNA sequencing
The PCR products free of contaminating bands due to nonspecific amplification were directly sequenced in forward and reverse direction. Nucleotide changes were detected by comparing sequence obtained in a chromatogram with the normal LRRK2 gene sequence (GenBank Accession No. AY792511) using pair-wise BLAST (Tatusova and Madden, 1999) and SeqScape software v2.5
Results
A total of 320 study subjects were included. The LRRK2 mutations were screened in a total of 150 (141 sporadic [94%] and 9 familial [6%]) patients with PD (mean ± SD, age at onset, 52.3 ± 5.17 years; age range, 37-80 years; 126 men and 24 women); Unified Parkinson's Disease Rating Scale (UPDRS) score was 31.2 ± 5.20, Hoehn and Yahr staging, 2.43 ± 1.10 and 170 controls (mean ± SD age [years] 57.6 ± 9.1; 130 men and 40 women). The age (p = 0.74) and sex (p = 0.23) distribution of patients and controls was similar. The patients and controls were classified into three common caste groups, namely Brahmin, Kayastha, and Baidya (Table 2). Minor groups such as Goala, Bagdi, and Poundra Khatriya were broadly named in the “others category” as the fourth group, and Muslims were taken as a religious group (Fig. 2). Most of the patients reported an increase in tremor and imbalance during periods of stress. Only four patients were untreated, whereas others are under antiparkinsonian treatment. Genetic analysis revealed none of the seven commonly reported mutations in the 320 subjects studied.
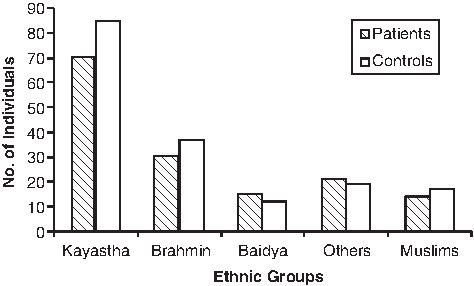
Caste-wise distribution of patients and controls.
Discussion
After screening a cohort of 150 PD patients and unrelated matched controls from Eastern India for the presence of seven common LRRK2 mutations in exon 31, 35, and 41, we did not observe any of these mutations. The LRRK2 G2019S mutation is the most common genetic determinant of PD (both familial and sporadic) identified to date (Fig. 1). Studies so far have reported frequencies of LRRK2 mutations between 1% and 7% in patients with PD of European origin and between 2% and 40% in Ashkenazi Jews and North African Arabs (Lesage et al., 2006; Ozelius et al., 2006; Ishihara et al., 2007). Though the G2019S mutation is absent in the Eastern Indian population, which is in accordance with the Chinese population (Tan et al., 2005), a single report demonstrated the presence of G2019S in only one Indian patient (0.12%) and low prevalence in Asia (Tan et al., 2005; Punia et al., 2006).
The I2012T and I2020T mutations are absent in our study, which is similar to the Taiwanese (Lu et al., 2005), Polish (Bialecka et al., 2005), and North Indian studies (Punia et al., 2006) earlier in contrast to the Japanese and Europeans (Zimprich et al., 2004b; Berg et al., 2005; Funayama et al., 2005). The R1441G mutation occurs in about 8% of patients with PD from the Basque country and 2.5% in the late-onset Spanish population (Paisan-Ruiz et al., 2004; Mata et al., 2005). This mutation is also not found in our cohort (Fig. 1), which is similar to the Italian (Goldwurm et al., 2005), Portuguese (Bras et al., 2005), and North Indian populations (Punia et al., 2006). Similarly, R1441C and R1441H were present neither in Eastern India (Fig. 1) nor among Portuguese (Bras et al., 2005) nor in a study from North India (Punia et al., 2006). Again, Y1669C is absent in our PD patient cohort, for example, the Italian population (Goldwurm et al., 2005), whereas it exists as 0.26% in German cohort (Zimprich et al., 2004b). Since most LRRK2 mutations appear to be limited to certain populations in various geographical locations (Fig. 1), different ancestry and founder effect (Zabetian et al., 2006) can be related to their variability, thereby explaining their absence in Indians.
Our study has some limitations. The studied cohort is relatively small. Although these common mutations are absent in our study, their contribution to PD cannot be completely excluded, as LRRK2 is a large gene and mutations, other rearrangements, or upstream region polymorphisms may exist in this population. Thus, mutation screening of the entire 51 exons of LRRK2 is important to determine the contribution of this gene to PD in Eastern India. Based on our results, routine testing for these mutations for diagnostic purpose and genetic counseling may not be cost effective, at least in the studied population.
Although LRRK2 mutations are reported at various frequencies in populations of Spain, Basques, African Arabs, and Ashkenazi Jews, this study indicates that these mutations do not significantly contribute to PD among the cases with familial PD and sporadic patients cutting across all the castes and groups taken in our study; thereby, they are of little relevance for their pathogenic role in this disease inheritance and cannot be recommended for the diagnostic screening.
Footnotes
Acknowledgments
This research work is supported by the grant from Anthropological Survey of India, Ministry of Culture, Government of India. The authors are thankful to the patients with PD and control subjects for voluntarily taking part in this research work and donating their blood samples. Mitali Maity (nurse in NNC) helped in the collection of blood samples from the OPD of NNC.
Disclosure Statement
No competing financial interests exist.