
Abstract
Background: Most hereditary hemochromatosis (HH) patients are homozygous for the p.C282Y mutation in the HFE gene. Some studies reported that HH phenotypic expression could be modulated by genetic factors such as HJV and HAMP gene mutations. Aims: The aims of this study were to identify HJV and HAMP mutations and to analyze their impact on HH phenotype in non-p.C282Y homozygous individuals. Methods: Twenty-four Brazilian patients with primary iron overload and non-p.C282Y homozygous genotype (transferrin saturation >50% in women and >60% in men and absence of secondary causes) were selected. Subsequent bidirectional sequencing of the HJV and HAMP exons was performed.
Introduction
H
The presence of lower rates of Brazilian patients carrying a homozygous genotype for the p.C282Y mutation compared with northern European patients may suggest that, in this particular population, other non-HFE mutations may be determinant in the genetic epidemiology of HH (Merryweather-Clarke et al., 1997; Pereira et al., 2001; Cancado et al., 2006; Bittencourt et al., 2009).
The juvenile form of HH (juvenile hemochromatosis [JH]) is a rare iron overload disease that affects young patients, usually leading to organ damage before the age of 30, and frequently causes cardiomyopathy, hypogonadotrophic hypogonadism, and endocrine disease (Wallace and Subramaniam, 2007). JH is classified as type 2A and 2B, which are caused by mutations in genes encoding hemojuvelin (HJV) and hepcidin (HAMP), respectively (Roetto et al., 2003; Papanikolaou et al., 2004). Hepcidin is a peptide that plays a role in iron absorption related to ferroportin of the enterocyte and it is inappropriately decreased in HFE-HH patients (Wallace and Subramaniam, 2007). The function of hemojuvelin remains unclear, but patients with JH type 2A presented with low urinary hepcidin concentration, implying that HJV is hepcidin related (Papanikolaou et al., 2004).
The HJV gene was identified in 2004 and several mutations have been found in patients, but the p.G320V mutation is the most frequent and has been reported in iron overload patients in several populations around the world (Lanzara et al., 2004; Lee et al., 2004; Papanikolaou et al., 2004; Aguilar-Martinez et al., 2007). HAMP gene mutations are a rare cause of JH (Roetto et al., 2003; Jacolot et al., 2004; Porto et al., 2005). Some studies support the concept that digenic inheritance of HFE and HJV or of HFE and HAMP mutations can lead to iron overload or may aggravate the phenotype (Biasiotto et al., 2004; Jacolot et al., 2004; Lee et al., 2004).
Here, we have directly sequenced the HJV and HAMP genes in Brazilian patients with the diagnosis of primary iron overload. The main aims were to identify HJV and HAMP mutations and to analyze their impact on HH phenotype in non-p.C282Y homozygous genotype Brazilian patients.
Materials and Methods
Subjects
Twenty-four Brazilian subjects with primary iron overload and non-p.C282Y homozygous genotype from the Santa Casa Blood Center of Sao Paulo, Sao Paulo, Brazil, were studied. Data of patients (age, “color/ethnicity” group, and symptoms) were obtained through a structured interview. The study protocol was approved by the Institutional Ethics Committees (School of Pharmaceutical Sciences, University of Sao Paulo; and Santa Casa Blood Center of Sao Paulo), and written informed consent was obtained from all participants prior to entering the study.
The diagnosis of primary iron overload was based on the absence of secondary causes of iron overload, such as parenteral or dietary iron overload, alcohol abuse, chronic hemolytic anemia, thalassemia major, and hepatitis, and on the presence of transferrin saturation (>50% in women and >60% in men) (Adams, 2000; Le Gac et al., 2003; Aguilar-Martinez et al., 2005; Brissot et al., 2008). Patients with secondary causes of iron overload and absence of transferrin saturation values defined, and patients carrying a p.C282Y homozygous genotype were excluded from the present study (Zaahl et al., 2004; Mendes et al., 2009). HFE gene sequencing was known for all included individuals (unpublished data).
Family history information of HH or iron overload was obtained through an interview for patients with primary iron overload and non-p.C282Y homozygous or heterozygous genotype. None of these patients reported any family history.
Independently of molecular diagnosis, all patients who were biochemically diagnosed with iron overload at two separate times, without any secondary diseases, were submitted to therapeutic phlebotomy.
Laboratory determinations
Blood was drawn using BD Vacutainer System® containing K2EDTA (Becton Dickinson) for blood cell count and genetic analysis, and an additional sample of blood was collected in a BD Vacutainer System® without anticoagulant.
The concentration of serum iron and total iron binding capacity were measured with the automation system Advia 1650® (Bayer Diagnostics). The value of transferrin saturation was obtained by the ratio of the concentration of serum iron to total iron binding capacity and it was expressed as a percentage. Serum ferritin concentration was determined using Axsym System® (Abbott Laboratories). Determination of hepatitis C was performed using Murex anti-HCV® kit (Murex Biotech S.A), and hepatitis B was detected using Hepanostika anti-HBc Uni-Form® and Hepanostika HbsAg Uni-FormII® kits (BioMérieux).
DNA extraction and sequencing
Genomic DNA was isolated from peripheral blood leukocytes by a salting-out method (Salazar et al., 1998).
Exons 1-4 of the HJV gene and exons 1-3 of the HAMP gene were amplified by polymerase chain reaction using eight and two sets of primers, respectively, as suggested by Lee et al. (2004) and Zaahl et al. (2004). These sets of primers were located 50-100 nucleotides from the splice site. Polymerase chain reaction products were purified using ExoSAP-IT® reagent (GE Healthcare) and were bidirectionally sequenced using the ABI Terminator Sequencing Kit according to the manufacturer's instructions and an ABI 377 Sequencer (Applied Biosystems).
Results
General characteristics
Of the 24 subjects with primary iron overload and non-p.C282Y homozygous genotype included in this study, 9 (37.5%) were women and 15 (62.5%) were men. The median age of studied patients and iron parameters are presented in Table 1. The group of patients was separated into self-identified subgroups according to “color/ethnicity,” as Caucasian descent (n = 11, 45.8%), Mulatto (n = 9, 37.4%), African descent (n = 1, 4.2%), and Asian (n = 3, 12.6%) (Vargens et al., 2008; Santos et al., 2010). In the studied sample, six patients were found to be heterozygous for the HFE p.C282Y and nine patients were heterozygous for the HFE p.H63D (unpublished data).
Data are presented as median (25% and 75% percentiles).
F, female; M, male.
HJV gene sequencing
Screening of the HJV gene revealed no mutations in exons 1-3. In exon 4, the c.929C > G substitution that corresponds to p.A310G amino acid change (rs7540883) was identified (Fig. 1). This variant was detected in compound heterozygosity with the HFE p.H63D polymorphism in a 58-year-old woman presenting with transferrin saturation of 60.0% and serum ferritin concentration of 443.0 μg/L. The main symptom was hepatomegaly at 1 year after menopause. Regarding color/ethnicity, this woman identified herself as Mulatto, and she reported that her father was African descent and her mother was Caucasian descent (Italian).
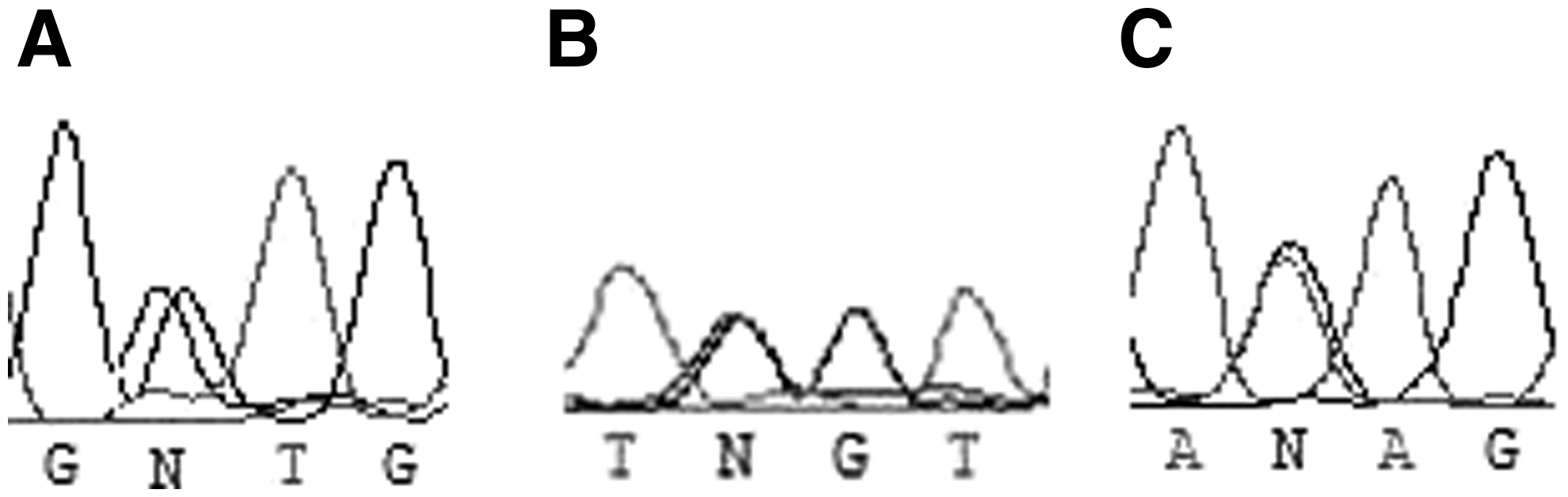
HJV and HAMP gene sequencing results.
In addition, the IVS1-36C > G intronic variant was found in heterozygous form (Fig. 1) in a 46-year-old woman presenting with transferrin saturation of 95.0%, serum ferritin concentration of 2794.0 μg/L, and wild-type genotype for the HFE gene mutations.
HAMP gene sequencing
Mutations were not detected in exons 1-3 of the HAMP gene. The IVS3 + 42G > A intronic substitution was detected in heterozygosity (Fig. 1) in a 47-year-old man presenting with transferrin saturation of 50.0%, serum ferritin concentration of 537.0 μg/L, and heterozygous genotype for the HFE p.H63D polymorphism.
These intronic variants (HJV IVS1-36C > G and HAMP IVS3 + 42G > A) did not demonstrate potential for change in their respective splice site according to GeneSplicer® (www.cbcb.umd.edu/software/GeneSplicer/).
Discussion
Autosomal recessive inheritance is well known as being associated with HFE, HJV, and HAMP gene mutations (Feder et al., 1996; Zaahl et al., 2004), and HH phenotypic expression is complex and modulated by genetic and environmental factors (Beutler, 2003).
In the general population, some studies have reported that the HJV gene mutations are uncommon (Barton et al., 2004; Le Gac et al., 2004; Pissia et al., 2004). Barton et al. evaluated HJV p.G320V and p.I222N mutations in 241 Alabama White individuals and 124 African American individuals. Only one individual with the heterozygous genotype for the p.I222N mutation was found (Barton et al., 2004). In a French study with 333 control subjects, the HJV p.L101P and p.E302K mutations were identified in the heterozygous forms in two and one individuals, respectively (Le Gac et al., 2004). Pissia et al. (2004) performed a genotype screening of 200 unrelated apparently healthy blood donors of Greek origin, and none of the 400 chromosomes that were studied carried the HJV p.G320V mutation.
Previous studies have reported that HJV and HAMP gene mutations act as genetic modifiers in the HH phenotype (Merryweather-Clarke et al., 2003; Biasiotto et al., 2004; Jacolot et al., 2004; Le Gac et al., 2004). Jacolot et al. (2004), based on a digenic model of inheritance, suggested that the association of heterozygous mutations in the HFE and HAMP genes could lead, at least in some cases, to an adult-onset form of primary iron overload. Le Gac et al. (2004) reported new data that HJV mutations could be associated with a similar effect.
Merryweather-Clarke et al. (2003) proposed that the phenotype of p.C282Y heterozygotes and homozygotes may be modified by heterozygosity for mutations that disrupt the function of hepcidin in iron homeostasis, with the severity of iron overload corresponding to the severity of the HAMP mutation. Similarly, Biasiotto et al. (2004) found that the new mutations p.N196K of the HJV gene and −72C > T of the HAMP gene at the heterozygous state aggravated the clinical phenotype and the biochemical indices in HFE compound heterozygous individuals, indicating that both genes behave as similar modifying genes in HH.
In contrast, Altès et al. (2009) found a very low frequency of HJV and HAMP gene variations in a Spanish patient cohort, indicating a minor impact of these mutations in the penetrance of HFE-related hemochromatosis, and Lee et al.(2004) demonstrated that coding region polymorphisms in the HJV gene were also not associated.
We hypothesized that other HJV and HAMP gene mutations could be together with HFE-related mutations and thus increase the risk of developing HH phenotype.
Here, we found the p.A310G polymorphism in the HJV gene (which is apparently nonfunctional) (Lee et al., 2004; Zaahl et al., 2004) and two intronic variants (HJV IVS1-36C > G and HAMP IVS3 + 42G > A). These intronic variants did not demonstrate potential for change in their respective splice site, and even if their impact was confirmed in functional studies, it is improbable that its heterozygosity causes the HH phenotype. Consequently, we were not able to demonstrate digenic inheritance between these two genes and the HFE gene.
The HJV p.A310G polymorphism has been described in previous studies in iron overload subjects, but its presence was not associated with iron overload phenotypes (Lee et al., 2004; Zaahl et al., 2004). In addition, it was detected in 19 African American control subjects in allele frequency of 7% and in 2 African American with iron overload in allele frequency of 2% (Lee et al., 2004).
In the present study, no patients had early age-of-onset iron overload (main characteristic of the JH), and we should not exclude that HJV and HAMP mutations may be common in individuals with clinical signs of the juvenile form. Further, it is possible that additional mutations in other genes related to the regulation of iron homeostasis (e.g., transferrin receptor 2 and ferroportin genes) could have contributed to the hemochromatosis expression in the studied patients. It is also conceivable that these individuals could be carriers of mutations located in intronic or regulatory regions of HH-related genes (Pietrangelo, 2006; Allen et al., 2008).
In conclusion, HJV p.A310G polymorphism and two intronic variants were found, but none of these alterations were associated with digenic inheritance with the HFE gene. Our data indicate that HJV and HAMP functional mutations are not frequent in these patients.
Footnotes
Acknowledgments
This study was supported financially by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, Proc. 2008/54131-0), Brazil. P.C.J.L. Santos is a recipient of fellowship from Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil. The authors thank the patients who participated in the study. The technical assistance of the Laboratory of Genetics and Molecular Cardiology group of the Heart Institute is gratefully acknowledged.
Disclosure Statement
No competing financial interests exist.