
Abstract
Recent studies have identified genetic markers that may directly influence the risk of the coronary artery disease (CAD), in particular the renin angiotensin system genes. Since there are no existing data for the Tunisian population, we investigated the association between these polymorphisms (angiotensin-converting enzyme [ACE] insertion/deletion [Ins/Del]; the angiotensinogen T174M and M235T; and the angiotensin II type 1 receptor A1166C polymorphisms) and CAD in Tunisians. Study subjects comprised 341 cases and 316 age- and sex-matched healthy individuals. Clinical characteristics and other biochemical and environmental risk factors were collected for both. The distribution of the Ins/Del genotypes was significantly different between cases and controls (p = 0.049) with the genotype Ins/Ins identified as a risk, p = 0.02. Similarly, the distributions of the T174M and M235T genotypes were significantly different between cases and controls (p = 0.037 and 0.047, respectively) with 174 M/M and 235 T/T as the risky genotypes (p = 0.001 and 0.026, respectively). However, A1166C genotype frequencies were not significantly different between patients and controls. In conclusion, our results suggest that a significantly higher risk of CAD was associated with the Ins/Del, the M235T, and T174M polymorphisms; other environmental variables such as body mass index; and biochemical variables such as cholesterol.
Introduction
C
ACE influences the cardiovascular system via the metabolism of bioactive peptides including bradykinin and angiotensins (Krieger and Dzau, 1991). Serum ACE level remains relatively constant over time in a given individual, whereas it varies significantly among unrelated individuals. A major component of the interindividual quantitative variation in serum ACE activity is genetically determined (Cambien et al., 1988) and linked to the ACE gene locus (on chromosome 17) (Zhu et al., 2001). The Ins/Del polymorphism in the ACE gene consisting of the presence (Ins) or absence (Del) within intron 16 of a 287 bp Alu repeat sequence, resulting in three genotypes: Del/Del, Ins/Ins (homozygous), and Ins/Del (heterozygous) (Rigat et al., 1990), was found to account for nearly half the variation in the serum ACE activity in some populations (Tiret et al., 1992; Agerholm-Larsen et al., 1999).
The AGT is located on chromosome 1q42-43 and comprises five exons and four introns spanning 12 kb (Gaillard et al., 1989; Jeunemaitre et al., 1997). Several molecular variants of this gene have been detected, and two polymorphisms in exon 2 were the most studied. In the first polymorphism, a methionine at position 235 is replaced by a threonine (M235T variant) and in the second, a threonine at position 174 is replaced by a methionine (T174M variant) (Jeunemaitre et al., 1992).
The A1166C polymorphism consisted of an A to C transversion at the position 1166, which is located in the 3′ untranslated region of the AT1R gene (chromosome 3) (Bonnardeaux et al., 1994). Many studies have shown that it is associated with coronary heart disease and myocardial infarction (MI) (Tiret et al., 1994).
The aim of the present study is to investigate the relationship between RAS gene polymorphisms and CAD in the Tunisian population, while analyzing and adjusting for other environmental and biochemical variables.
Materials and Methods
Study subjects
This is a case-control designed study conducted in the intensive care units of cardiology of different hospitals in Tunisia. Our study sample consisted of 341 cases who had a stable angina (SA) or an acute coronary syndrome defined as acute MI (AMI) or unstable angina. Relevant history of cardiovascular disease, cardiovascular risk factors, and current treatment were obtained from each patient using a standard questionnaire, and the data were validated with reference to hospital records. SA or acute coronary syndrome was defined for this study according to the following criteria: clinical symptoms, electrocardiogram findings, and cardiac enzyme abnormalities. For some patients, these data were also corroborated by coronary angiography. AMI was classified as ST segment elevation and/or new bundle branch block and non-ST elevation based on the presence or absence of N1 mm of ST segment elevation on two or more continuous leads on the initial electrocardiogram. Unstable angina is defined as a clinical syndrome falling between SA and MI in the spectrum of patients with CAD.
Risk factors such as body mass index (BMI, kg/m2), family history of coronary disease, arterial hypertension (≥130 mm Hg systolic blood pressure, ≥90 mm Hg diastolic blood pressure), smoking history, and hyperlipidemia (total cholesterol N240 mg/dL and triglycerides N250 mg/dL) were also evaluated. The control group consisted of 316 healthy individuals with no personal and family history of CAD. Patients were matched with controls with regard to sex and age. Since ethnic differences may influence our conclusions, only Tunisian Arabs were included as cases or controls. Berbers (native Tunisians) and other Tunisian ethnic minorities were not considered.
Genotyping protocols
Genomic DNA was extracted from peripheral blood leukocytes using the salting out method as described by Miller et al. (1988). Polymerase chain reaction-based protocols were used to identify the ACE Ins/Del (Fig. 1) (Rigat et al., 1992; Lindpaintner et al., 1995), AGT M235T (Russ et al., 1993), AGT T174M (Fig. 2) (Caulfield et al., 1994), and ATR1 A1166C (Bonnardeaux et al., 1994) polymorphisms, as previously described.
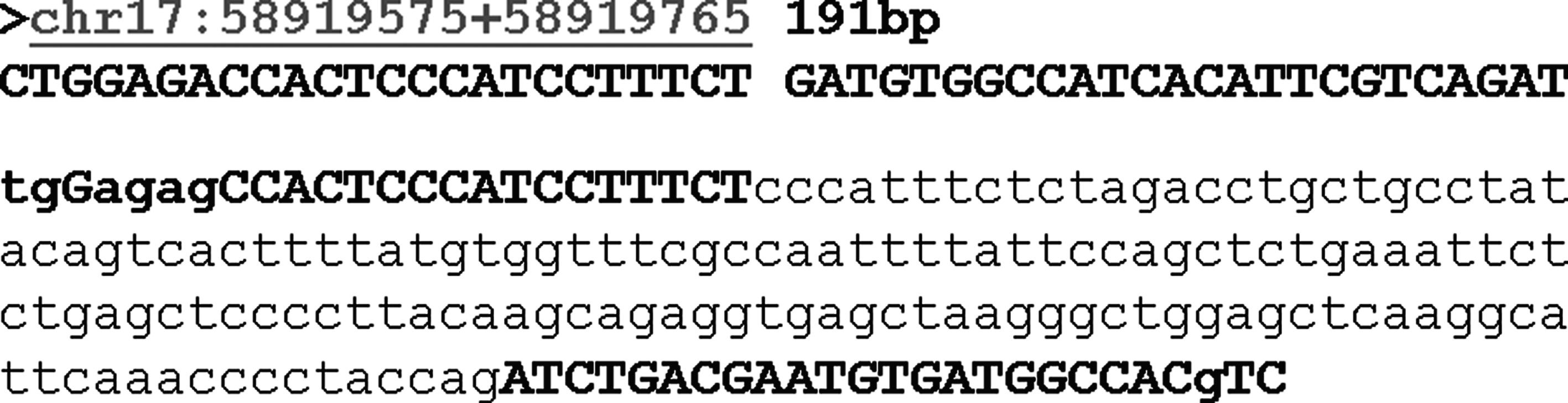
The detection principle of insertion/deletion polymorphism on angiotensin-converting enzyme gene with polymerase chain reaction.

The detection principle of polymorphisms M235T and T174M on the angiotensinogen gene with polymerase chain reaction-restriction fragment length polymorphism using, respectively, the two restriction enzymes SfaNI and NcoI (gray shades indicated the polymorphisms sites).
Statistical analysis
Interindividual differences were compared using the two-tailed t-test. Allele frequencies were calculated by a gene counting method using the HLA Stat2000 population software, which also calculated the differences in haplotype frequency between the cases and controls; and the Hardy-Weinberg equilibrium was tested by calculating the χ2 and p-values, using the H-Plus Haplotype Estimation software (http://qge.fhcrc.org/hplus). Fisher's exact test was used to assess intergroup significance between categorical variables, and Student's t-test was used to determine differences between continuous variables. Logistic regression was performed to estimate odds ratio (OR) and 95% confidence interval (CI). Statistical analyses were carried out using SPSS Windows version 13.0; statistical significance was set at p < 0.05.
Results
Clinical characteristics of study subjects
There were 341 patients (75.7% were men; mean age, 55.4 ± 10.6 years) and 316 healthy individuals (72.2% were men; mean age, 54.1 ± 9.4 years). Complete clinical history and CAD risk factors were taken for all study participants.
Mean systolic was higher among cases (p < 0.001), whereas comparable diastolic was seen in cases and controls, and a higher percentage of hypertensive subjects (p < 0.001) was seen in cases (p < 0.001). Also, the lipid profile was different between the two populations. However, the serum glucose was comparable between both groups. Mean BMI (24.4 ± 1.9 and 26.1 ± 3.1; p < 0.001) was lower in controls compared with cases. All characteristics of study subjects are summarized in Table 1.
Student's t-test (two-sided).
Pearson's chi-square test.
BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Allele and genotype analysis
In both (cases and controls) as well as both groups pooled together, the genotype frequencies were in agreement with Hardy-Weinberg equilibrium. The allele frequencies and the genotype distributions in the cases and controls for all four polymorphisms are shown in Table 2.
Genotype and allele frequencies.
p determined with Yates chi-square test.
ACE, angiotensin-converting enzyme; AGT, angiotensinogen; AT1R, angiotensin II type 1 receptor; CI, confidence interval; Ins/Del, insertion/deletion; OR, odds ratio.
ACE and AGT (M235T and T174M) polymorphisms genotype frequencies were significantly different between cases and controls. Yates chi-square test leads to simulated p-values: 0.049, 0.047, and 0.037, respectively.
The Ins/Ins genotype is significantly higher in cases compared with controls (p = 0.02, OR = 1.9, 95% CI = 1.07-3.49).
For the AGT T174M polymorphism, a higher frequency of homozygotes MM (risky genotype) was observed in cases compared with controls, p = 0.001, with the OR and 95% CI are 1.8 and 1.12-2.94, respectively. Similarly, for the AGT M235T polymorphism, a higher frequency of the TT homozygotes (risky genotype) was observed in patients compared with controls, p = 0.026, OR = 1.7, and 95% CI is 1.03-2.82.
For AT1R, the genotypes frequencies were similar in cases and controls.
Risk factors for MI
Predictors of CAD were determined by performing multinomial regression, with the dependent variable being CAD and the independent potentially confounding variables being BMI; hypertension; total cholesterol; triglycerides; homozygous ACE Ins/Ins, AGT 174 T/T, and 235 M/M; and heterozygous ACE Ins/Del, AGT 174 T/M, and 235 M/T genotypes (Table 3). Only BMI (OR = 0.801; 95% CI = 0.663-0.968) and total cholesterol (OR = 0.273; 95% CI = 0.169-0.442) were the identified acquired risk factors associated with CAD (Table 3).
Determined by chi-square test.
Haplotype distribution
The 174M/M235 haplotype was present at lower frequencies in patients with CAD compared with controls (p = 0.04 vs. 0.774), thereby conferring a disease protection to this haplotype (Table 4). The prevalence of the other haplotypes was comparable between both groups.
Determined by the HLA Stat2000 software.
p determined by chi-square test.
Discussion and Conclusion
Since the report of Cambien et al. (1992), several studies have examined the role of ACE Ins/Del polymorphism in CAD. In addition to its association with MI in American (Ludwig et al., 1995) and Japanese (Nakai et al., 1994) subjects, the Del/Del genotype has been reported to be more frequent in European (Tiret et al., 1993) and Scandinavian (Bohn et al., 1993) children; in (Badenhop et al., 1995) grandchildren of Australians with a history of coronary events; in Irish subjects with a fatal MI (Evans et al., 1994); in French patients with noninsulin-dependent diabetes and clinical coronary heart disease (Ruiz et al., 1994); and in low risk Welsh subjects with coronary heart disease (Mattu et al., 1995). Despite these reports, other studies failed to observe any association of this genotype with MI or angina, or both, in Scandinavian (Bohn et al., 1993), American (Lindpaintner et al., 1995),, or New Zealand (Katsuya et al., 1995) subjects.
However, the present study showed that there is a significant association for the ACE Ins/Del polymorphism considered between CAD and control groups, and the risk of developing the disease is increased among Ins/Ins genotype carriers, thus suggesting that the ACE Ins/Del polymorphism may contribute to CAD outcome.
Our data also agree with other reports (Steeds et al., 2001; Hernandez et al., 2002) demonstrating that the AT1R gene A1166C polymorphism is not associated with CAD. Indeed, that the risk of developing CAD was not increased in any of the three AT1R genotypes suggests that this polymorphism is not a risk factor for CAD.
In spite of several studies (Ishigami et al., 1995; Katsuya et al., 1995) that demonstrated a significant association between coronary heart disease and the M235T polymorphism, in 12 studies combined, the T allele was not associated with atherosclerotic cardiovascular complications (Staessen et al., 1999). Our data join the first ones, so there was an association between CAD and AGT M235T polymorphism demonstrating that 235T/T genotype seems to be a risk factor for CAD.
The T174M polymorphism was demonstrated to be in complete linkage disequilibrium with the M235T variant (Jeunemaitre et al., 1992). It was associated with hypertension (Jeunemaitre et al., 1992) and examined for association with other cardiovascular disorders (Marre et al., 1997). In fact, our results join 12 studies with 4952 subjects which found that the overall frequency of the M allele of T174M variant was 11% (Staessen et al., 1997) and the MM homozygous made up 1.2% of all subjects examined. Besides, in our study, the M/M genotype seems to be a risk factor for CAD.
Further, in this study, conventional risk factors were highly prevalent in patients, as expected (Vogel and Motulsky, 1997; Wilson and Culletton, 1998), especially BMI and triglycerides. However, some variations in risk factors were expected due to their independent nature.
These results were further supported by regression analysis, which demonstrated, after controlling for other variables, that only BMI and triglycerides were identified as dependent acquired risk factors for CAD.
The AGT M235T polymorphism was in strong linkage disequilibrium with the T174M polymorphism. Such allelic association was expected due to the vicinity of their chromosomal location. We observed associations between AGT haplotypes and risk of CAD. Those who are homozygous for the 174M/M235 haplotype have lower risk than others. This last haplotype seems to be a protective factor against CAD.
In fact, there have been many reports regarding the association between RAS gene polymorphisms and CAD or AMI, but the results are inconsistent. So many of these studies used several new approaches with multilocus data to reappraise this issue in different populations.
Especially in a study that was the first to demonstrate epistatic, high-order gene-gene interactions between RAS gene polymorphisms and CAD, T174M, M235T, G-6A, A-20C, G-152A, and G-217A polymorphisms of the AGT gene were genotyped among homogeneous Taiwanese population (Tsai et al., 2007). They found that the AGT gene haplotype profile was significantly different between the cases and controls (χ2 = 31.6, p = 0.030) in haplotype analyses. Further, significant three-locus (G-217A, M235T, and Ins/Del) gene-gene interactions were detected by a multifactor-dimensionality reduction method (highest cross-validation consistency 10.0, lowest prediction error 40.56%, p = 0.017) and many even higher order gene-gene interactions by multilocus genotype disequilibrium tests (16 genotype disequilibria exclusively found in the controls, all of which included at least two genes among the AGT, ACE, and AT1R genes) (Tsai et al., 2007). These results are compatible with the concept of multilocus and multigene effects in complex diseases that would be missed with conventional approaches.
In summary, our results demonstrate a significantly higher risk of CAD associated with the ACE Ins/Ins, AGT 235 T/T, and 174M/M genotypes. However, the AT1R A1166C polymorphism is not associated with CAD in the Tunisian population. Predictive testing using a single gene variant may have limited or little usefulness, whereas a multivariate analysis may be more adequate to dissect genetic risk factors.
Further, the assessment of RAS activation in clinical practice is routinely carried out by plasma renin activity measurement based on determination of angiotensin I, generated in vitro, under controlled conditions, from the endogenous AGT. Usually, the amount of generated angiotensin I is linearly related to active renin concentration; although in some pathophysiological conditions there are no correlations between angiotensin I and angiotensin II (such as in pregnancy and in patients with arterial hypertension or under ACE-inhibitors [ACE-i] treatment) (Arnal et al., 1991).
However, the circulating levels of renin cannot be considered a suitable prognostic marker in CAD, because the renin assay is strongly affected by the pharmacological treatment (including diuretics, ACE-I, and angiotensin II antagonists) (Kjaer and Hesse, 2001). Also, circulating levels of renin are not strictly related to the activation of tissue RAS in patients with CAD. Indeed, the decrease in angiotensin II after treatment with ACE-i can stimulate renin release, which, in turn, can increase AGT consumption and so angiotensin I production. Therefore, the use of plasma renin activity, as an index of RAS activation, could be sometimes unreliable depending on both enzyme and substrate levels.
On the other hand, several studies indicated that the determination of angiotensin II should be a helpful complementary tool for a better assessment of the RAS activity and for the monitoring of pharmacological intervention in patients with CAD.
Finally, integration of these results and genetic screening results with established acquired risk factors may have greater utility.
Footnotes
Acknowledgments
This study received financial support from the Secretariat of the State for Scientific Research, Technology, and Competencies Development in Tunisia, through funding of Research Program Contract (2004-2008), the Research Unit of Hematological and Autoimmune Diseases, Faculty of Pharmacy, University of Monastir (UR99/08-50).
Disclosure Statement
No competing financial interests exist.