
Abstract
The matrix metalloproteinase (MMP) family are key enzymes involved in the breakdown of the extracellular matrix in normal physiological processes, including tissue remodeling, and disease processes, such as arthritis and metastasis. The promoter polymorphism in the MMP2 gene may be responsible for multiple diseases related to extracellular matrix degradation. Therefore, we aimed to investigate the relationship between genotypes or haplotypes of -1575 G/A, -1306 C/T, -790 T/G, and -735 C/T promoter polymorphisms and coronary artery disease (CAD) with or without myocardial infarction (MI) history. This study included 298 patients with angiographically confirmed CAD and 299 age matched controls. Genomic DNA was isolated from whole blood and genotyping was performed by the polymerase chain reaction-restriction fragment length polymorphism method. No significant associations were found between -1575 G/A, -1306 C/T, and -790 T/G polymorphisms and CAD with or without MI history. However, the frequency of the -735 TT genotype was significantly lower in the controls than in the patients with MI alone when compared with the CC genotype (p = 0.021). Only the distribution of the ACGC haplotype in CAD patients exhibited a significant difference than that in controls (p < 0.05). The distribution of other haplotypes did not differ between CAD patients and controls. The present investigation is the first report to detect an association between MMP2 promoter polymorphisms and CAD with or without MI history in the Turkish population. Further case-control studies in CAD development might be contributed to clarify the role of these polymorphisms.
Introduction
Coronary artery disease (CAD), one of the major causes of mortality worldwide, is a complex, multifactorial, chronic, and highly frequent vascular disorder (Horne et al., 2007; Kim et al., 2007). Epidemiological studies have identified smoking, obesity, diabetes, hypertension, and hyperlipidemia as among the risk factors for CAD. However, in some individuals, CAD is not associated with conventional risk factors (Cam et al., 2005; Matyar et al., 2005). In this case, multiple genetic factors including mutations and polymorphisms have been associated with the risk of CAD (Jaramillo et al., 2006). According to previous studies, single-nucleotide polymorphisms of MMPs appeared to be genetic risk factors for atherosclerosis or CAD (Pollanen et al., 2001; Abilleira et al., 2006).
One of the potential candidate genes associated with CAD or MI is MMP-2 (also named as gelatinase A). The principle activity of MMP-2 is hydrolysis of gelatin and type IV collagen (Delgado-Enciso et al., 2008). The MMP-2 gene has been mapped to chromosome 16q13 and contains 13 exons encoding a 72-kDa protein (Price et al., 2001; Holla et al., 2005). The MMP-2 gene promoter region contains AP-2, p53, Sp1, and Sp3 transcription factor-binding sites (Qin et al., 1999). Genetic variants in the MMP-2 promoter region might affect gene expression and thus would be expected to impact on progression of pathological processes (Price et al., 2001). The -1575 G/A polymorphism in the promoter region of the MMP-2 gene affects binding of the estrogen receptor (Price et al., 2001; Harendza et al., 2003). The -1306 C/T polymorphism is located in the CCACC box of the Sp1-binding site and displays a strikingly lower promoter activity with the T allele (Price et al., 2001; Baltazar-Rodriguez et al., 2008). Another single-nucleotide variation is -790 T/G located in the inverted GATA-1 element (CTATCT) in the promoter region of MMP-2 gene. Yu et al. (2004) have described that another promoter C/T polymorphism at nucleotide -735 damages an Sp1-binding element and that promoter activity is significantly diminished by the T allele. So far, the few association studies that have been published have been based on one or a few MMP-2 promoter polymorphisms and have focused on a variety of diseases such as cervical neoplasm, severe chronic periodontitis, melanoma, CAD, breast cancer, coronary triple-vessel disease (TVD), nasopharyngeal carcinoma (NPC), and intrauterine growth restriction risk (Vasků et al., 2004; Cotignola et al., 2007; Gremlich et al., 2007; Horne et al., 2007; Zhou et al., 2007; Baltazar-Rodriguez et al., 2008; Delgado-Enciso et al., 2008; Gürkan et al., 2008). Therefore, the aim of the present study was to compare the distribution of genetic variants of the aforementioned polymorphisms in patients with CAD with or without MI history and control individuals. In addition, we also examined the association of MMP-2 gene haplotypes with CAD in the Turkish population.
Materials and Methods
Study population
The study included 298 patients with angiographically confirmed CAD (≥50% stenosis at least one coronary vessel) and 299 age-matched controls admitted to Gazi University, Faculty of Medicine. CAD subjects were classified into MI and non-MI subgroups. Presence or absence of a history of MI was done by combining data from the clinical history, after a thorough review of medical records including electrocardiogram, enzyme changes, and/or the typical sequelae of MI on ventricular angiography. The control subjects had undergone coronary angiography because of atypical chest pain after noninvasive cardiac examination. Insignificant coronary artery stenosis was excluded from this study. All participants were interviewed and data on smoking habits, hypertension, diabetes mellitus, hypercholesterolemia, and family history of CAD were recorded. Informed consent was obtained from all patients and controls according to the guidelines of our university ethics committee. The subjects were defined as hypertensive if their blood pressure was greater than 140/90 mm Hg or if they were receiving any antihypertensive medication. Diabetes mellitus was defined by previous diagnosis, a history of antidiabetic drug use, or fasting glucose levels above 126 mg/dl. The subjects were considered to be hypercholesterolemic if their low-density lipoprotein levels were above 130 mg/dl.
Genotyping
Genomic DNA was extracted from whole blood, anticoagulated with K2EDTA, using Heliosis® DNA extraction kit (Metis Biotechnology) according to the manufacturer's instructions.
The genomic DNA was amplified in a 50 μL reaction mixture containing 75 mM Tris-HCl (pH 8.8), 200 mM (NH4)2SO4, 0.1% Tween-20, 200 μM of each dNTP, 1 U of Taq DNA polymerase (Fermentas), 50 pmol of each set of primers, and different concentrations of MgCl2 and DMSO for each polymorphism (Table 1). Forward primers of four polymorphism and reverse primers of -1575 G/A and -1306 C/T polymorphisms were used as previously published (Vasků et al., 2004). Reverse primers for MMP-2-735 C/T and -790 T/G were designed by our research group (see Table 1 for the primer sequences and the annealing temperatures). The amplification cycle was carried out in an automated thermalcycler (Eppendorf). The standard amplification profile consisted of initial denaturation at 94°C for 5 min followed by 30 cycles of 30 s at 94°C, 1 min at 55°C-65°C (Table 1), 1 min at 72°C, and a final extension time of 5 min at 72°C. The polymerase chain reaction (PCR) products were separated on 2% agarose gel and visualized with a Kodak Gel Logic 100 Imaging System (Kodak Co.).
Note: Amplifications of -735 C/T and -790 T/G polymorphisms were performed with the same forward and reverse primers under the same PCR conditions. PCR amplifications of -1306 C/T and -1575 G/A polymorphisms were also performed with same forward and reverse primers under the same PCR conditions.
AT, annealing temperature; MC, MgCl2 concentration; RE, restriction endonuclease;
For the detection of MMP-2-735 C/T and -790 T/G polymorphisms, about 15 μL of the 195-bp PCR products were digested overnight at 37°C with 10 U of HinfI and PvuI (MBI, Fermentas) under appropriate buffer conditions, respectively. The fragments were separated on 3% and 4% agarose gels (1% standard agarose + 3% nusieve agarose) for about 45 min at 100 V and visualized with a Kodak Gel Logic 100 Imaging System (Kodak Co.), respectively. The length of the digested fragments is given in Table 1.
For the detection of MMP-2-1306 C/T and -1575 G/A polymorphisms, 408-bp PCR products were digested overnight at 37°C with 10 U of MaeI and Tsp45I (MBI, Fermentas) under appropriate buffer conditions, respectively. After digestion, the fragments were separated on 3.5% and 2% agarose gels containing ethidium bromide for about 45 min at 100 V and visualized with a Kodak Gel Logic 100 Imaging System (Kodak Co.), respectively. The length of the digested fragments is given in Table 1.
Statistical analysis
Statistical analyses were performed using the SPSS statistical package for windows (version 15.0; SPSS, Inc.). The distribution of genotypes for each polymorphism was assessed for deviation from the Hardy-Weinberg equilibrium by using the chi-square test (χ2 test) with one degree of freedom. The frequencies of the alleles and genotypes in the patients and controls were compared by χ2 test or Fisher's exact test when necessary (expected values below 5). Crude odds ratios (ORs) were calculated together with their 95% confidence intervals (95% CIs) to estimate the relative risk of CAD or MI. A value of p < 0.05 was considered statistically significant. Arlequin software version 2.0 (Genetics and Biometry Laboratory, University of Geneva, Geneva, Switzerland) (Excoffier et al., 2005) and SNPStats (Sole et al., 2006) were used to estimate MMP-2 haplotype frequencies using the expectation maximization algorithm (Excoffier and Slatkin, 1995). The pairwise linkage disequilibrium values calculation was calculated using Haploview version 4.0 (www.broad.mit.edu/mpg/haploview) (Barrett et al., 2005).
Results
The baseline characteristics of the patients group with CAD with or without MI history and the control subjects are shown in Table 2. Statistically significant differences were found between CAD patients with or without MI history (CAD+MI) and control subjects in terms of all demographic and clinical characteristics, except age, hypercholesterolemia, and diabetes mellitus. Also, statistically significant differences in smoking habits, hypercholesterolemia, hypertension, and family history were found in the CAD without MI history (CAD) group, as opposed to the control group. When compared between the CAD with MI history (MI) and control groups, statistically significant differences were found in age, gender, smoking habit, and hypertension (Table 2).
p-Values <0.05 and <0.001 are shown in bold.
For the less-frequent alleles (23.2% for −1575 G/A, 20.9% for -1306 C/T, 23.9% for -790 T/G, and 11.4% for -735 C/T) with p = 0.05, the study had a power of >80 for all polymorphisms. In the controls and all CAD+MI cases, the genotype frequencies for the -1575 G/A, -1306 C/T, and -790 T/G polymorphisms did not deviate from the Hardy-Weinberg equilibrium (p > 0.05). In addition, -735 C/T genotype distribution did not deviate from the Hardy-Weinberg equilibrium in the control group (p = 0.07). However, -735 C/T genotype distribution was deviated from the Hardy-Weinberg equilibrium in the CAD+MI and MI groups (p = 0.01). Hardy-Weinberg equilibrium chi-square and p-values are presented in Table 3. This deviation was not likely to have been due to a laboratory error, because 50 randomly chosen samples were genotyped a second time with consistent results.
The genotype distributions and allele frequencies of the MMP-2 polymorphisms for the CAD+MI and control subjects are shown in Table 4. When we compared the genotype distributions of the -1575 G/A, -1306 C/T, -790 T/G, and -735 C/T polymorphisms between patients and controls, we found that the GG, CC, TT, and CC genotypes were more common in cases and controls, respectively. However, no appreciable association was found between these polymorphisms and CAD (p > 0.05).
Calculations were performed CC versus CT+TT.
Reference genotype/allele.
Calculations were performed TT versus TG+GG.
Calculations were performed CC versus CT+TT.
Calculations were performed GG versus GA+AA.
OR, odds ratio; CI, confidence interval.
When compared between the CAD or MI groups and control subjects, GG, CC, TT, and CC genotypes were more frequent in cases and controls for the -1575 G/A, -1306 C/T, -790 T/G, and -735 C/T polymorphisms, respectively. The genotype distributions and allele frequencies of -1575 G/A, -1306 C/T, and -790 T/G polymorphisms were similar in patients and controls. Therefore, no significant relationship was found between the two groups for these polymorphisms (p > 0.05) (Tables 5 and 6). However, the genotype distribution of the MMP-2-735 C/T polymorphism had borderline significant difference between patients with MI and controls (p = 0.054). The frequency of -735 TT genotype was lower in controls than in MI patients (2.3% vs. 7.1%). Moreover, the OR for TT genotype was 3.12 (95% CI: 1.13-8.62, p = 0.021) when compared with CC genotype (Table 6).
Reference genotype/allele.
Calculations were performed CC versus CT
Calculations were performed TT versus TG
Calculations were performed CC versus CT
Calculations were performed GG versus GA + AA.
OR, odds ratio; CI, confidence interval.
p-Values <0.05 are shown in bold.
Calculations were performed CC versus CT+TT.
Reference genotype/allele.
Calculations were performed TT versus TG+GG.
Calculations were performed CC versus CT+TT.
Calculations were performed GG versus GA+AA.
OR, odds ratio; CI, confidence interval.
Linkage disequilibrium was observed in four MMP-2 promoter polymorphisms (Fig. 1). The estimated population frequencies for the MMP-2 haplotypes in the CAD+MI and control groups are shown in Table 7. Only nine haplotype combinations were found in the CAD+MI and control groups. As expected, haplotype distribution indicates that the G-1575/C-1306/T-790/C-735 (GCTC) haplotype was the most frequent in both the patient and control groups. Only the distribution of ACGC haplotype in CAD+MI patients exhibited a significant difference than that in controls and the ACGC haplotype was more frequent in patients than in controls (OR: 6.02, 95% CI: 1.34-27.08, p = 0.008) (Table 7).
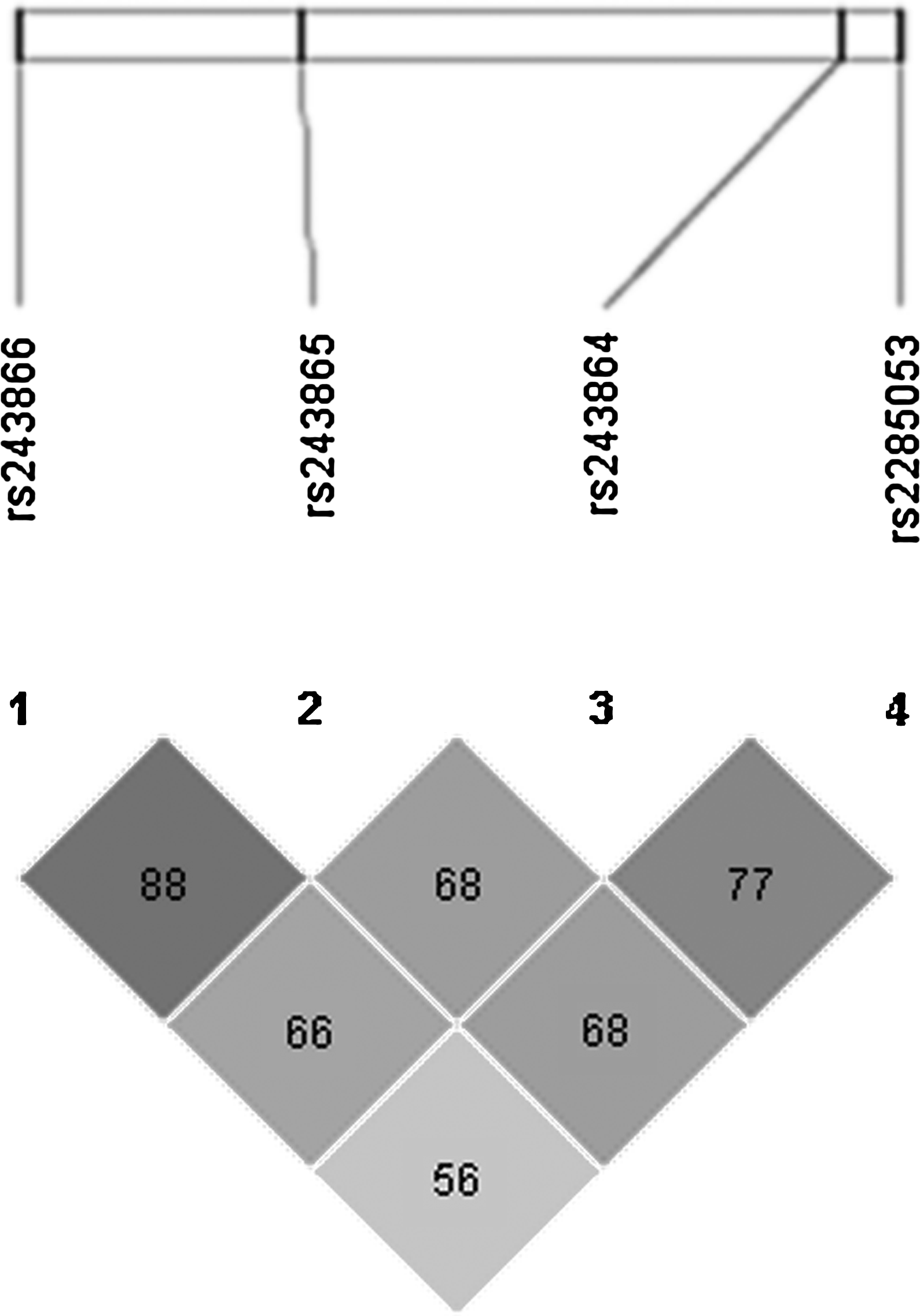
Linkage disequilibrium comparisons of four promoter polymorphisms in settlement order in the MMP2 gene.
p-Values <0.05 are shown in bold.
Calculations were performed GT versus TC, GC, TT.
Reference haplotype.
OR, odds ratio; CI, confidence interval.
Discussion
Dysregulation of MMP-2 expression has been demonstrated in CV diseases (Tyagi et al., 1996; Tsakiris et al., 2004; Nilsson et al., 2006). In two previous studies, higher levels of MMP-2 and MMP-9 were reported in patients presenting with acute coronary syndrome than in a stable effort angina group (Kai et al., 1998; Zeng et al., 2005). Hojo et al. (2001) showed that plasma levels of MMP-2 increase gradually after the onset of acute MI with maximum elevation on day 21 after onset. A possible increment of circulating levels of MMPs in unstable coronary plaques shown by these clinical studies is a consistent evidence of MMP expression near the surface of atherosclerotic plaques (Galis et al., 1994; Orbe et al., 2003). Therefore, the atherosclerotic plaque itself may be the intracoronary source of elevated plasma MMPs (Hlatky et al., 2007). The polymorphisms within the MMPs gene promoter could be one possible cause of its elevated expression. However, in our previous report, we did not find any association between the MMP-9-1562 C/T polymorphism and CAD in the Turkish population (Alp et al., 2009). On the other hand, there are few previous studies investigating the role of MMP-2 genetic polymorphisms in CV diseases (Lamblin et al., 2002; Vasků et al., 2004; Hinterseher et al., 2006; Armstrong et al., 2007; Bauters et al., 2007; Horne et al., 2007; Lin et al., 2007). Therefore, we investigated MMP-2 promoter polymorphisms in a Turkish population of patients with CAD or MI.
In our study, the genotype frequencies for the -1575 G/A, -1306 C/T, and -790 T/G polymorphisms did not deviate from the Hardy-Weinberg equilibrium in both the controls and cases. The -735 C/T genotype distribution was in Hardy-Weinberg equilibrium in the control group, whereas it deviated from Hardy-Weinberg equilibrium in the CAD+MI and MI groups (p > 0.05). Hardy-Weinberg equilibrium deviations in cases are primarily due to association effects (Nielsen et al., 1998). Excess heterozygotes and low frequency of the TT genotype would be possible explanations for this deviation.
The -1575 G/A polymorphism is located in the 5′ half-palindromic binding site (TGACC) for the estrogen response element in the MMP-2 promoter region (Harendza et al., 2003). Harendza and coworkers indicated that the -1575G/A transition significantly diminishes estrogen receptor binding and MMP-2 transactivation. Additionally, the -1575G allele also had an independent additive effect with the -1306C allele (Harendza et al., 2003; Beránek et al., 2008). To date, only five studies have investigated the relationship between the -1575 G/A polymorphism and disease associated with ECM regulation. In the first study, Holla et al. (2005) demonstrated that the -1575 G/A polymorphism did not contribute significantly to the periodontitis susceptibility and severity in European Caucasians. In the second study, Xu et al. (2007) showed that the -1575G allele is associated with the risk and invasive phenotype of colorectal cancer in a Chinese population. In another study, Beránek et al. (2008) did not find any association between the -1575 G/A polymorphism and proliferative diabetic retinopathy (PDR) in the Czech population. Vasku et al. (2009) showed that there was no relationship between psoriasis and the -1575 G/A polymorphism in the Czech population. With respect to CV diseases, only two studies have been performed. Hua et al. (2009) found a significant relationship between the -1575 G/A polymorphism and systolic heart failure in the Han Chinese population. However, Vasků et al. (2004) indicated that the -1575 G/A polymorphism was not associated with TVD in the Czech population. Similarly, our results showed no association between this polymorphism and CAD or MI in the Turkish population.
Price et al. (2001) demonstrated that the common C→T transition at position -1306 interrupts an Sp1-type promoter site (CCACC box). Transient transfection experiments showed that the -1306T allele displayed a strikingly lower promoter activity. This lower promoter activity may contribute to some diseases associated with ECM regulation, such as cancer, diabetic retinopathy, periodontitis, CAD, and MI. For instance, -1306 C/T variation contributes to the development of squamous cell cervical cancer especially in women and breast cancer in the Mexican population (Holla et al., 2005; Baltazar-Rodriguez et al., 2008; Beránek et al., 2008; Delgado-Enciso et al., 2008). However, there was no association between breast cancer and the -1306 C/T polymorphism in the Swedish population (Lei et al., 2007). Zhou et al. (2007) revealed that the -1306 C/T polymorphism of MMP2 gene was significantly associated with susceptibility to NPC in Chinese populations. In another study, Gremlich et al. (2007) demonstrated that the -1306 C/T polymorphism was related with an increased risk for intrauterine growth restriction. There are a few association studies between CV disease and the -1306 C/T variation in different populations. For example, Lamblin et al. (2002) reported that the -1306 C/T polymorphism was not associated with aneurysmal CAD in the French population. Vasků et al. (2004) noted that the T allele of the -1306 C/T polymorphism did not seem to be associated with the TVD in the Czech population. Additionally, the -1306 C/T polymorphism did not contribute to the development of abdominal aortic aneurysm (AAA), carotid artery intima-media thickness, MI, and CAD in German and American populations (Lamblin et al., 2002; Armstrong et al., 2007). In another study, left ventricular remodeling after MI was not associated with -1306 C/T variation in the French population (Bauters et al., 2007). In concert with these findings we did not find any relationship between this polymorphism and CAD or MI in the Turkish population as well.
The -790 T/G variation maps to a degenerate site of the core GATA-1 consensus region (Price et al., 2001). Three different transcription factors could be found to interact with the T allele sequence (gut-enriched Krueppel-like factor, S8, and Evi1 [ectopic viral integration site 1 encoded factor]) but not in the -790G allele, according to a special database (Transfac Matrix Table - MatInspector V2.2) (Vasků et al., 2004). The binding of these transcription factors may affect the MMP-2 gene expression levels in cells. There are a few association studies related to ECM-dependent diseases. Vasku et al. (2009) showed that the genotype distributions were significantly different in psoriasis patients compared with controls. Holla et al. (2005) showed that decreased frequency of the -790 GG genotype was observed in patients with chronic periodontitis compared with healthy controls. Hovewer, Beránek et al. (2008) found that there was no association between the -790 T/G polymorphism and PDR. In another study, Vasků et al. (2003) demonstrated that the T allele is significantly more frequent in patients with coronary TVD and chronic heart failure in the Czech population. According to Vasků et al. (2003), TT genotype was significantly more frequent in patients with angina pectoris. However, Hua et al. (2009) reported that there was no relationship between the -790 T/G polymorphism and systolic heart failure in the Han Chinese population. We found that the TT genotype was more frequent in patients with CAD or MI as well as controls. Therefore, we did not find any relationship between the -790 T/G polymorphism and CAD or MI in the Turkish population. These differences may result from the different CV diseases investigated and also the ethnicities of the study populations.
The -735 C/T substitution of the MMP-2 gene destroys an Sp1-binding element, which leads to altered transcription of the gene (Price et al., 2001). The -735CC genotype was significantly associated with lung and nasopharyngeal cancer risk in nonsmokers and smokers in the Chinese population (Zhou et al., 2005, 2007). In the Turkish population, the -735 C/T polymorphism was not associated with susceptibility to severe chronic periodontitis (Gürkan et al., 2008). Holla et al. (2005) showed that the frequency of the -735 C/T polymorphism was similar in patients with chronic periodontitis and healthy controls. In another study, Beránek et al. (2008) indicated that there was no association between the -735 C/T polymorphism and PDR. Armstrong et al. (2007) showed that the -735 C/T polymorphism was not associated with carotid artery intima-media thickness in the German population. In the Czech population, Vasků et al. (2003, 2004) found that the -735 C/T polymorphism was not associated with coronary TVD but was associated with chronic heart failure. In our study, we did not find a relationship between the -735 C/T polymorphism and CAD+MI or CAD in the Turkish population. However, the genotype distribution of the MMP-2-735 C/T polymorphism had borderline significant difference between patients with MI and controls (p = 0.054). The frequency of the -735 TT genotype was lower in controls than in MI patients (2.3% vs. 7.1%). Moreover, the homozygote TT genotype had about a threefold increased risk of developing MI compared with homozygote CC subjects (Table 6).
In previous studies, the -735CC/-1306CC haplotype was proposed as a susceptibility factor for esophageal and lung cancers (Yu et al., 2004; Zhou et al., 2005). In Chinese populations, Zhou et al. (2007) found that the C-1306-C-735 haplotype was significantly associated with increased susceptibility to NPC. In Czech populations, although the haplotype GCGC was identified only in healthy subjects, the haplotype GCTC was more frequent in the TVD patients (Vasků et al., 2004). As expected, in our study, the haplotype distribution indicates that the G-1575/C-1306/T-790/C-735 (GCTC) haplotype was the most frequent. But only the distribution of ACGC haplotype in CAD patients exhibited a significant difference than that in controls (p < 0.05). Moreover, we found that ACGC haplotype carriers had about sixfold increased risk of developing CAD compared with GCTC haplotype.
In conclusion, this is the first study that investigated the relationship between -1575 G/A, -1306 C/T, -790 T/G, and -735C/T MMP-2 promoter polymorphisms and CAD with or without MI in a Turkish population. This is the first report to detect an association between an MMP-2 promoter polymorphism and CAD with or without MI in a Turkish population. We emphasize that the limitation of the present study is the sample size because of the exclusion of mild CAD patients (<50% stenosis in one or more epicardial vessels). Several participants in the control group were also excluded because of abnormal clinical characteristics. Only borderline significant differences in the MMP-2-735 C/T polymorphism were found between the MI and control groups (p = 0.054). This polymorphism of the MMP-2 gene may contribute to the susceptibility to MI in the Turkish population. Apart from that, we did not find any significant association between MMP-2 promoter polymorphisms and CAD with or without MI history. Moreover, ACGC haplotype carriers were found to have an increased risk for CAD development (p < 0.05). Discrepancies in our results and other studies may be due to the different molecular mechanisms of CAD development or different ethnicities of study populations. However, these polymorphisms can explain only a small part of the genetic susceptibility to CAD. Thus, further large-scale case-control studies might contribute to better understanding of the role of these polymorphisms in CAD in the Turkish population. Besides, further studies in larger series of different populations and additional association polymorphism studies are needed to characterize the molecular mechanisms of susceptibility to CAD. If confirmed by other studies, knowledge of genetic factors contributing to the pathogenesis of CAD as presented here could lead to improved treatment and screening of this disorder.
Footnotes
Acknowledgment
This study was partially supported by the Gazi University Research Fund as a project with code number 11/2004-84.
Authors Contribution Statement
S.M. was manager of the project and contributed of the manuscript at writing. EA, A.Y., and S.M. designed the genetic study. E.A. and A.Y. established and performed genotyping, analyzed the data, performed statistical analysis, and drafted the manuscript. S.M., R.Y., and A.C. revised the data and the manuscript. M.T., R.Y., and A.C. collected the blood samples and the clinical data. All authors have read and approved the final version of the manuscript.
Disclosure Statement
No competing financial interests exist.