
Abstract
Type 2 diabetes mellitus (T2DM) is a major cause of coronary artery disease (CAD) and is responsible for a great deal of morbidity and mortality in Asian Indians. Several gene polymorphisms have been associated with CAD and T2DM in different ethnic groups. This study will give an insight about the association of two selected candidate gene polymorphisms; paraoxonase1 (PON1) Q192R and apolipoprotein A5 (APOA5) −1131T>C were assessed in a cohort of South Indian patients having CAD with and without T2DM. Polymerase chain reaction-based genotyping of PON1 Q192R (rs662) and APOA5-1131T>C (rs662799) polymorphism was carried out in 520 individuals, including 250 CAD patients (160 with T2DM and 90 without T2DM), 150 T2DM patients with no identified CAD, and 120 normal healthy sex- and age-matched individuals as controls. The PON1 192RR genotype and R allele frequency were elevated in both CAD and T2DM patients when compared with controls; however, only CAD patients with T2DM showed a statistical significance (p=0.023; OR=1.49; 95% CI: 1.04-2.12) when compared with controls. The APOA5-1131CC genotype and C allele also showed a significant association between the CAD+T2DM patients when compared with CAD without T2DM and healthy controls (p=0.012; OR=1.71; 95% CI: 1.0-2.67). An additive interaction between the PON1 RR and APOA5 TC genotypes was identified between the T2DM and CAD patients (p=0.028 and 0.0382, respectively). PON1 and APOA5 polymorphisms may serve as biomarkers in the South Indian population to identify T2DM patients who are at risk of developing CAD.
Introduction
CAD is one of the major complications of T2DM and is responsible for high morbidity and mortality. CAD rates vary in different populations—the frequency of CAD in Asian Indians worldwide is 50%-400% higher than among people of other ethnic origin, irrespective of gender, religion, or social class (Enas and Senthilkumar, 2002). A demographic shift in population age profile combined with lifestyle resulting in an increase in cardiovascular risk factors is further accelerating the “heart disease” epidemic in India (Reddy, 1993). The impact of genetic factors on the development of CAD and myocardial infarction has been demonstrated in several studies (Topol et al., 2006).
Such associations have been established by a systematic screening using genome-wide association analysis or by selected candidate gene approach (Hegele, 2009). Recently, our group has shown a combined correlation of ACE (angiotensin-converting enzyme) and CETP (cholesterol ester transfer protein) gene polymorphism with cardiovascular disease in an Asian Indian patient cohort with and without type 2 diabetes (Ganesan et al., 2011). Gene polymorphisms are markers of biologic diversity and genotypic variations, which correlate with specific phenotypes sometimes associated with the development of human disease in different ethnic groups.
Possible candidate gene polymorphisms in CAD are those involved in lipid metabolism; thus, paraoxonase 1 (PON1) and apolipoprotein A5 (APOA5) genes were chosen in the present study to assess their association with CAD and T2DM in a South Indian cohort. PON1 is a high-density lipoprotein (HDL)-associated esterase that hydrolyses lipoperoxides. PON1 serves as a protective factor against oxidative modification of low-density lipoprotein (LDL), suggesting that it may play an important role in the prevention of the atherosclerotic process. PON1 level has been shown to be important in protecting against vascular disease, presumably because of the not-as-yet fully characterized role of the three PON proteins in the modulation of oxidative stress. However, epidemiologic, genetic, and biochemical studies support an antiatherogenic role of PON1.
The PON1 gene is a 26,857-bp gene with nine exons, is localized on chromosome 7q21.3 (Gene ID: 5444), and codes for a glycoprotein that is located on the surface of HDLs and plays a pivotal role in preventing LDL oxidation (Wang et al., 2003). This may be one of the mechanisms by which HDL protects against atherosclerosis and CAD. There is evidence that genetic variation in the PON genes influences paraoxonase activity. The Q192R polymorphism has been demonstrated to affect PON1 activity (Taskıran et al., 2009). Low PON1 activity and decreased paraoxonase serum levels due to some polymorphisms in PON1 gene have been associated with CAD (Leviev et al., 1997; Mackness et al., 1998). PON1-192R allele and RR genotype are significantly associated with CAD in patients from the North Indian population (Uttar Pradesh). This association was stronger in smokers, supporting the conclusion that low PON1 activity along with smoking enhances CAD risk (Agrawal et al., 2009). Large differences in PON1 genotype distribution between various populations may be the reason for the variation among CAD prevalence in ethnic groups (Koda et al., 2004).
The gene APOA5 influences the level of plasma triglycerides, as demonstrated on mouse models and in human population studies (Eichenbaum-Voline et al., 2004). The associations between APOA5 concentrations, triglycerides, and CAD remain controversial (Szalai et al., 2004). APOA5 gene was found to be located proximal to the well-characterized APOAI/CIII/AIV gene cluster on human chromosome 11q23. The APOA5 gene is considered as a probable biochemical and genetic marker of increased triglyceride concentrations and also as a risk factor for coronary disease in some populations (Oliveira Sousa et al., 2008). It has now been clearly established that distinct polymorphisms in the APOA5 gene influence plasma triglycerides in human populations, although some differences between ethnic groups and between males and females were described (Hubacek, 2005). A single-nucleotide polymorphism −1131T/C in the APOA5 locus has been reported to be associated with high plasma triglyceride levels in two independent studies (Seda and Sedova, 2003). Therefore, this polymorphism was selected for evaluation in patients with T2DM, who have a tendency toward high plasma triglycerides and increased oxidative stress (Girona et al., 2008).
In this study, we assessed the frequency of PON1 and APOA5 gene polymorphisms in a cohort of South Indian patients having CAD with or without T2DM. This is a pilot study carried out to provide information whether these polymorphisms can be used as biomarkers for the prediction of genetic risk for CAD.
Materials and Methods
Patients and controls
Institutional ethical committee approval was obtained from the respective hospitals from which the patients were chosen for the study. Clinical details were also obtained from the clinical consultants and records of all the patients. The study was comprised of 150 T2DM, 90 CAD, and 160 CAD+T2DM patients and 120 controls. The controls were age and sex matched and normal healthy individuals without any clinical symptoms of diabetes or CAD. All the CAD patients who were recruited for the study were already on treatment with antihypertensive and antithrombotic agents (statins and ecosprin), and the T2DM patients were on either oral hypoglycemic drugs or insulin; hence, the results of biochemical evaluation were not correlated with genotypes for concern regarding treatment bias.
Genetic analysis
Genomic DNA was isolated from peripheral blood leucocytes according to a standard protocol (Miller et al., 1988). The sequence-specific primers (F: 5′ AAACCCAAAT ACATCTCCCAGAAT 3′ and R: 5′ GCTCCATCCCACATCTTGATTTTA 3′) for Q192R polymorphism in PON1 gene were used for polymerase chain reaction (PCR) amplification (Shao-Yong et al., 2005). The PCR products were analyzed on agarose gel and then digested with Hinf1 restriction enzyme overnight at 37°C. Digested samples were subjected to electrophoresis on 2% agarose gel and analyzed in Gel Doc under UV light (Fig. 1).
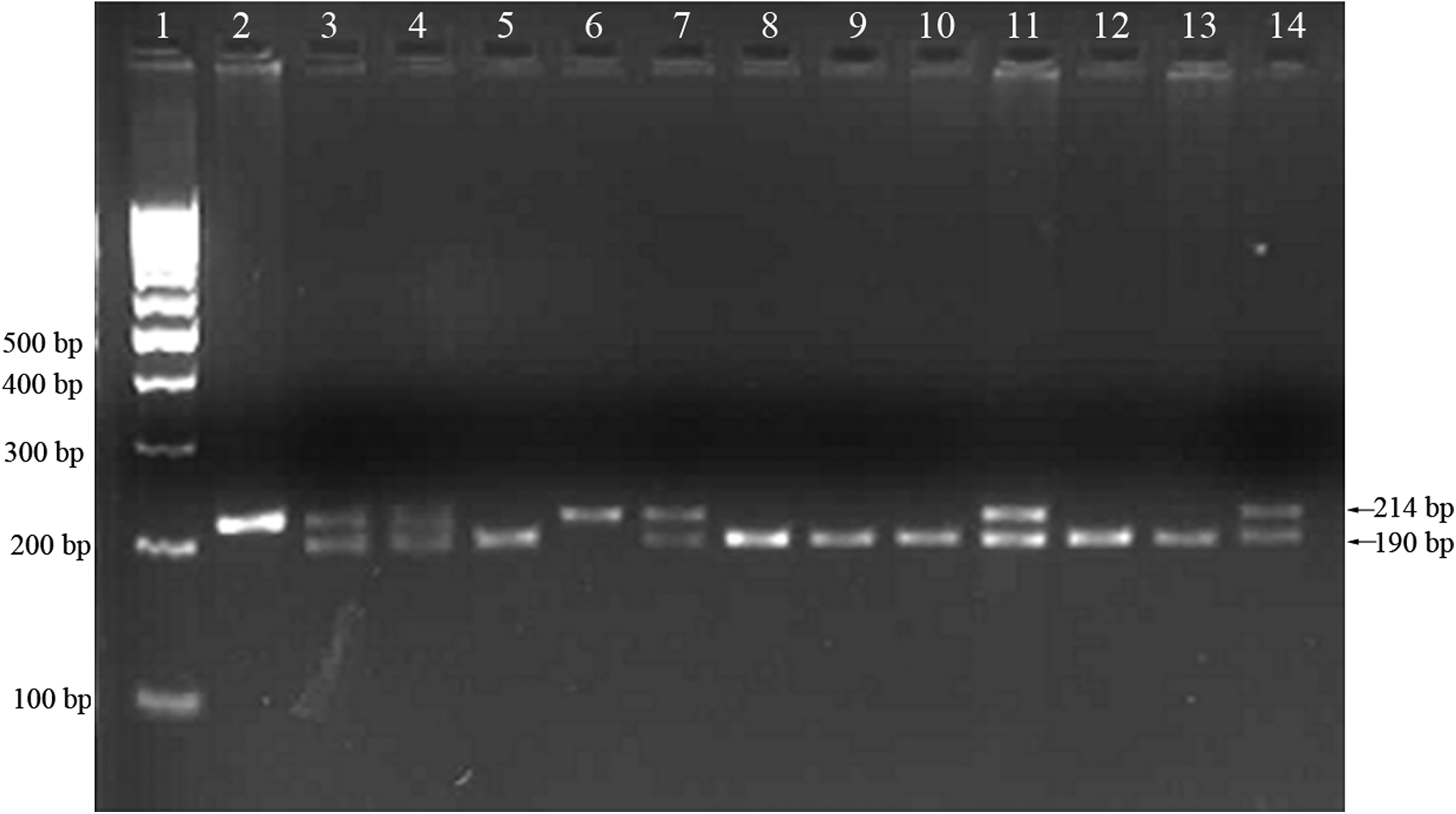
The polymerase chain reaction products after restriction digestion were electrophoresed on 3% agarose gel. Lane 1: 100-bp DNA ladder; lanes 2 and 6: band of 214 bp (QQ genotype); lanes 3, 4, 7, 11, and 14: heterozygous with two bands of 214 and 190 bp (QR); lanes 5, 8, 9, 10, 12, and 13: single band of 190 bp (RR genotype).
The DNA samples were genotyped for −1131T/C APOA5 polymorphism by the ARMS PCR method with the use of specific primers previously described (Chandak et al., 2006). PCR was performed according to the following conditions: initial denaturation at 95°C for 3 min, followed by 35 cycles of denaturation at 95°C for 1 min, annealing at 59°C for 1 min, and extension at 72°C for 1 min, with a final 2 min extension at 72°C. The PCR products were run on a 2% agarose gel and analyzed in Gel Doc under UV light (Fig. 2).
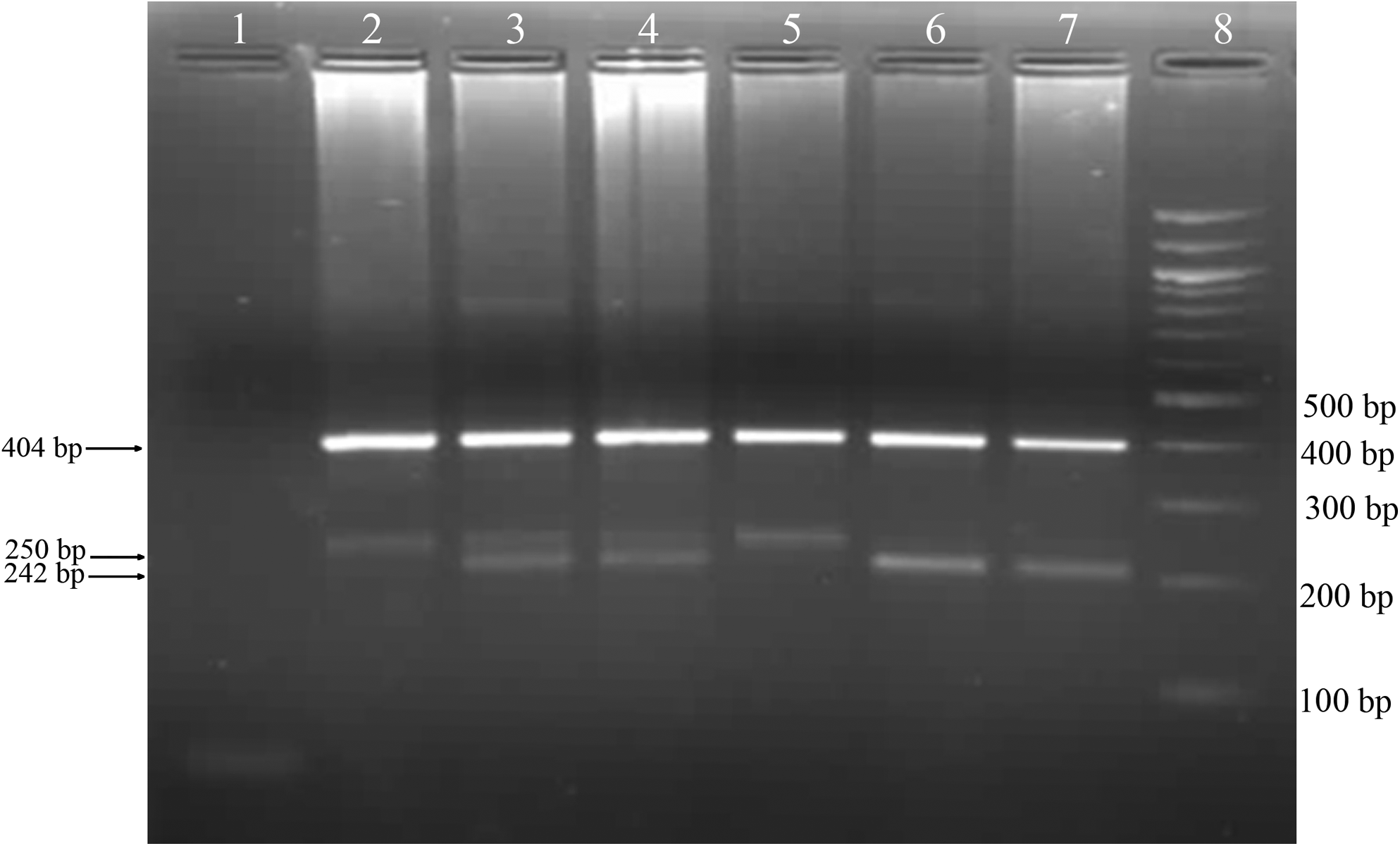
Agarose gel electrophoresis (3% agarose gel) showing genotypes at −1131T>C polymorphism in the APOA5 gene. Lane 1: negative control; lanes 2 and 5: TT genotype; lanes 3 and 4: heterozygous TC genotype; lanes 6 and 7: CC genotype; lane 8: 100-bp DNA ladder.
Statistical analysis
To analyze deviation from the Hardy-Weinberg equilibrium, the observed and expected genotype frequencies were compared with the use of the Markov simulation-based goodness-of-fit test (Schaid et al., 2002). Pearson's chi-square and Yates corrected chi-square tests were used to analyze the statistical significance of the difference in allelic distribution of various polymorphisms in different patient groups and the controls. Odds ratios were calculated to assess the strength of the association. Two-tailed p-values of <0.05 were considered statistically significant (PEPI version 4 <C> JH Abramson and PM Gahlinger 1993-2001).
Results
In this case-control study, we assessed the frequency of PON1 (rs 662) and APOA5 (rs662799) gene polymorphism occurrence in patients with CAD and with or without T2DM from the city of Hyderabad in South India.
PON1 Q192R polymorphism frequency was assessed and its three identified genotypes are presented in Figure 1. The 214-bp product corresponds to RR genotype, 214 and 190 bp bands correspond to heterozygous QR genotype, and 190 bp bands correspond to QQ genotype; 33.3% of controls had QQ genotype, 55.0% had QR, and 11.7% had RR (Table 1). The RR genotype and R allele were higher in all the patient groups compared with controls. However, the chi-square test revealed significant differences in allele distributions between the control group and the diabetic group as well as between T2DM patients with CAD (p=0.029, 0.023; Table 1). The R allele was also significantly associated with CAD+T2DM (OR=1.49; 95% CI: 1.04-2.12).
Values are given as n (%).
Controls.
Type 2 diabetes mellitus patients without coronary artery disease.
Type 2 diabetes mellitus patients.
Coronary artery disease patients.
Coronary artery disease patients with and without diabetes mellitus.
Patients with coronary artery disease and type 2 diabetes mellitus.
a versus c: p=0.029; OR=1.40; 95% CI: 1.02-1.92.
a versus f: p=0.023; OR=1.49; 95% CI: 1.04-2.12.
T2DM, type 2 diabetes mellitus; CAD, coronary artery disease.
Genetic APOA5-1131 T/C polymorphism, which has been known to be associated with the rise in triglyceride level by 20%, was studied and evidenced after genotyping by the 4-primer method (Ward et al., 2003). The frequency of APOA5-1131 T/C polymorphism was assessed and the following genotypes were identified: TT (250 bp), CC (242 bp), and heterozygous TC genotype (250 and 242 bp). Figure 2 also shows the common 404 bp outer band, which was used as the PCR control. The genotype distribution was in Hardy-Weinberg equilibrium. In healthy controls, TT genotype was present in 58.3%, TC in 34.2%, and CC in 7.5% (Table 2).
Values are given as n (%).
Controls.
Type 2 diabetes mellitus patients without coronary artery disease.
Type 2 diabetes mellitus patients.
Coronary artery disease patients.
Coronary artery disease patients with and without diabetes mellitus.
Patients with coronary artery disease and type 2 diabetes mellitus.
c versus d: p=0.034; OR=1.52; 95% CI: 1.01-2.30.
a versus f: p=0.034; OR=1.50; 95% CI: 1.01-2.22.
d versus f: p=0.012; OR=1.71; 95% CI: 1.10-2.67.
The analysis of interactions between PON1 and APOA5 gene polymorphisms revealed a statistically significant association (p=0.0382) between RR and TC genotypes in CAD+T2DM cases and controls. These results suggest the existence of interactions between the studied gene polymorphisms of PON1 and APOA5 and the risk for CAD in T2DM patients (Table 3).
Values are given as OR (95% CI), p-value.
p<0.05 (TC and RR genotypes of APOA5 and PON1 genes interact together in causing the disease).
Discussion
The prevalence of CAD in urban India is similar to that observed in more affluent overseas Indian populations (Enas and Senthilkumar, 2002). Diabetes and dyslipidemia are two major risk factors for CAD, which are associated with high oxidative stress. The analysis of PON1 192 QR polymorphism has revealed that the high-activity allele (R) is associated with a more atherogenic lipid profile than the low-activity allele (Q). In the present study, the PON1 192R allele frequency in all of the patients (T2DM, CAD, and T2DM+CAD) was found to be higher when compared with controls. However, the differences were statistically significant only in CAD+T2DM patients when compared with controls (p=0.04). The PON1 RR genotype was associated with a ninefold increase in the risk of CAD development in Egyptians, whereas the PON1 QR genotype had a fourfold increase (Mohamed et al., 2010). They have also provided evidence of a significant association between the R allele of the PON1 polymorphism and the development of arterial disease. A study carried out in China suggests that PON1 Q192R polymorphism was not independently associated with CAD but increased the risk of CAD among individuals with T2DM (Mendonça et al., 2008).
PON1-192R allele and RR genotype are significantly associated with CAD in patients from a North Indian population. This association was stronger in smokers, supporting the thesis that low PON1 activity along with smoking enhances CAD risk. Further studies with larger sample size are required to confirm these associations in different Indian populations (Agrawal et al., 2009). The PON1 is exclusively associated with HDL cholesterol, which has an antioxidant activity. At present, PON1 status, that is, its activity and concentration, is considered to be more important than the polymorphism alone in the prevention of CAD. Its activity has been found to be affected by a number of pharmacological agents, diet, and other factors, thereby becoming a promising target for pharmacological intervention (Gupta et al., 2009). PON1 activity is heavily influenced by PON1-Q192R polymorphism. A Norfolk prospective population study shows that PON1 activity inversely correlates with CAD risk in an HDL-dependent manner, because of its close association with the HDL particle. These data strongly suggest that low PON1 activity is not a causal factor in atherogenesis (Birjmohun et al., 2009).
PONs may exert antiatherogenic action by reducing lipid peroxidation. A previous study (Gluba et al., 2010) suggests that PON1 192Gln/Arg polymorphism influenced the risk of premature MI. The association between PON1 genotype (192 Gln/Arg) and serum LDL cholesterol levels may be explained by PON participation in reverse cholesterol transport. There are very few studies concerning PON1 in India, but none of them has dealt with PON1 polymorphism. A study on North Indian patients with CAD and T2DM revealed that low plasma PON1 activity may be an independent risk factor for CAD in a northwestern Indian Punjabi population (Singh et al., 2007). More studies involving large number of patients from other ethnic groups from India are required to determine the role of PON1 activity and gene polymorphisms in the pathogenesis of CAD.
A study conducted on a Turkish population suggests that PON1 Q192R genetic variants are associated with CAD. PON1 Q192R in CAD patients seems to be connected with the number of diseased vessels, hypertension, and hyperlipidemia. Relative risk for CAD in PON1 192RR carriers was 80% higher than in the population having different genotypes (Mendonça et al., 2008; Ozkok et al., 2008). Another study showed that in CAD patients, oxidative stress was high, and it was most evident in the RR-phenotype group. The QQ phenotype is associated with the lowest oxidative stress status level and also with a better capacity of antioxidative protection (Kotur-Stevuljevic et al., 2008; Mirdamadi et al., 2008).
The metabolic syndrome, a major cluster of risk factors for CAD, shows increasing prevalence worldwide. In T2DM patients, the prevalence of hypertriglyceridemia is increased. APOA5 is considered to be a genetic modulator of triglyceride concentration (Cabré et al., 2009). Another study (Hubacek et al., 2004) reported that the APOA5 polymorphism (-1131T>C) affected plasma triglycerides in a Czech population. Their study suggests that variations in the APOA5 gene not only plays a role in genetic determination of triglyceride levels, but also increases the risk of CAD. The frequency of the APOA5 polymorphism (-1131T>C) varies considerably across different ethnic groups. The prevalence of the −1131C allele in American Caucasians was 6.4%, in the Japanese population it reached 34% (Nabika et al., 2002; Pennacchio et al., 2002), whereas in our controls it was 7.5%. In a recent study conducted in a northern Chinese Han population, the allele frequency of APOA5-1131C polymorphism in the premature coronary heart disease group was significantly higher than that in the control group (Yu et al., 2007). The APOA5-1131T>C polymorphism was associated with higher very low-density lipoprotein (VLDL)-TGs in diabetic patients in a Spanish population (Girona et al., 2008). The decreased APOA5 was implicated in insulin resistance-related hypertriglyceridemia in obese people (Huang et al., 2010). In our study, we observed that the frequency of CC was not different between controls and patients with CAD but without T2DM; however, it showed a significant association with CAD+T2DM. This suggests that in our population the APOA5 gene polymorphism confers a risk of CAD in T2DM patients.
Conclusions
CAD remains the principal cause of death in many countries despite changes in lifestyle and the development of new pharmacologic approaches, indicating the importance of identifying genetic and environmental factors in the pathogenesis of these diseases. One of the important risk factors for developing CAD is T2DM. Our study indicates that genetic biomarkers can be used to identify individuals at risk of developing CAD in T2DM patients as well as to provide appropriate medical management to prevent this dreaded complication of diabetes.
Our data suggest that T2DM individuals with PON1 192R and APOA5-1131 C alleles have a high risk of developing CAD. Hence, these gene polymorphisms individually or in combination can be proposed as candidate biomarkers for CAD in T2DM patients in the South Indian population.
Footnotes
Acknowledgments
The authors acknowledge all the individuals who participated in this study. Support from Osmania University and Council for Scientific and Industrial Research (CSIR) is duly acknowledged.
Disclosure Statement
There is no commercial or proprietary interest on any product or company.