
Abstract
The prevalence of Fragile X Syndrome (FXS) is 1 in 4000 in males and 1 in 2500 in males and females, respectively, in the general population. Several screening studies aimed at determining the prevalence of FXS have been conducted in individuals with intellectual disabilities (IDs) with a prevalence varying from 1.15% to 6.3% across different ethnic groups. A previous study in Indonesia showed an FXS prevalence of 1.9% among the ID population. A rapid, effective, and inexpensive method for FMR1 screening, using dried blood spots capable of detecting an expanded FMR1 allele in both males and females, was recently reported. We used this approach to screen 176 blood spots, collected from Central Java, Indonesia, for the presence of expanded FMR1 gene alleles. Samples were collected from high-risk populations: 112 individuals with ID, 32 obtained from individuals with diagnosis of autism spectrum disorders, and 32 individuals with a known family history of FXS. Fourteen subjects carrying an FMR1 expanded allele were identified including 7 premutations (55-200 CGG repeats) and 7 full mutations (>200 repeats). Of the seven subjects identified with a full mutation, one subject was from a non-fragile X family, and six from were families with a history of FXS.
Introduction
F
The first population study of FXS performed in Indonesia, based on the screening of 176 subjects (92 males and 84 females), indicates a prevalence of 1.9% (Faradz et al., 1999). Special education needs schools, developmental disorders clinics, or health care centers are the most appropriate places for FXS screening in developing countries. In the past several years, the interest of FXS studies has turned treatment studies, both pharmacological and nonpharmacological intervention, and has emphasized the importance of early intervention for minimizing behavioral impairment and optimizing cognitive functioning. FXS, caused by immature branching of dendrites, results in lack of fragile X mental retardation protein (FMRP), an RNA binding protein important for synaptic plasticity (Zalfa et al., 2003). The awareness of fragile X-associated disorders, such as FXTAS and FXPOI, recently became more pronounced and reinforced the statement that FXS is a genetic disorder with broad clinical family involvement (Chonchaiya et al., 2009). Expanded clinical involvement, especially medical co-morbidity and neurobehavioral disorders that include thyroid dysfunction, high blood pressure, peripheral neuropathy, fibromyalgia, depression, and anxiety, has been reported as common among premutation females (Johnston et al., 2001; Hessl et al., 2005; Coffey et al., 2008; Bourgeois et al., 2009, 2010; Roberts et al., 2009; Hunter et al., 2010; Lachiewicz et al., 2010). Finally, lowered FMRP expression and/or elevated FMR1 mRNA, observed in premutation carriers, combined with environmental factors may lead to ASD and/or symptoms of attention deficit hyperactivity disorders (ADHD), social deficits, and learning disabilities in young premutation individuals (Tassone et al., 2000; Aziz et al., 2003; Goodlin-Jones et al., 2004; Farzin et al., 2006; Hagerman, Hoem et al., 2010).
Thus, to identify individuals with FXS and FMR1-associated disorders and to provide early intervention services for children, an FMR1-sensitive and -specific screening method for both males and females is needed in countries with a large population, such as Indonesia. Tassone et al. (2008) introduced a rapid, effective, and inexpensive method for screening both males and females for FMR1 allele sizes throughout the premutation and full-mutation range and is possible by using dried blood spots (Fernandez-Carvajal et al., 2009; Yuhas et al., 2009); thus, this method is suitable for large population screenings. Here, we present a high-risk screening in Central Java, Indonesia, including 176 subjects (92 males and 84 females) with ID and/or known family history of FXS.
Materials and Methods
Participants
Blood spots were collected from 92 males and 84 females (n=176), including 112 individuals with IDs, 32 with a diagnosis of ASD, and 32 individuals who were the relative of someone with a previous diagnosis of FXS. Samples were collected from Central Java, Indonesia. One hundred twelve subjects with ID were screened from special need schools, 26 of whom were from schools for children with autism, and 6 subjects were mothers of children with autism. This study was approved by the Institutional Review Board of the University of California Davis and the Medical Ethical Committee of the Faculty of Medicine, Diponegoro University.
Screening methodology
Blood spots were collected from each subject on FTA cards (QIAcard FTA; Qiagen, Valencia, CA). Polymerase chain reaction (PCR) analysis was performed either directly on a punch from the dry blood spot, or from isolated DNA. Samples were prepared for PCR in two ways: washing the blood spots and DNA isolation. Washing a 2 mm blood spot disk was performed by using FTA purification reagents (Qiagen) using manufacturer's instructions. Briefly, three 5-min incubations with 200 μL of purification reagents were followed by two 5-min incubations with 200 μL of Tris-sodium EDTA buffer. Spots had been dried at room temperature for 1 h before they were directly introduced into the PCR mix (Tassone et al., 2008). For DNA isolation, two disks of 3 mm in diameter were punched from the blood spot, heated with digest solution at 57°C, and processed in a Qiaxtractor (Qiagen) according to the manufacturer's protocol. The PCR amplification was performed by using primer c and f conditions as previously described (Fu et al., 1991; Fernandez-Carvajal et al., 2009). The PCR products were visualized by using the Qiaxcel genetic analyzer (Qiagen) or by capillary electrophoresis (CE) (ABI 3100; Applied Biosystems, Carlsbad, CA). Results from the Qiaxcel genetic analyzer were analyzed as described in Fernandez-Carvajal et al. (2009). The CE results were analyzed by using the ABI Peak Scanner software (Applied Biosystems). DNA samples from men that did not yield a band after the first round of PCR, or DNA samples from females that yielded only one normal band with primers c and f, were subjected to a secondary, chimeric-CGG-primer-based PCR screening, as previously described (Tassone et al., 2008; Chen et al., 2010). The PCR amplicons were subjected to visualization on an agarose gel (Tassone et al., 2008) or by (CE) (Chen et al., 2010).
Follow-up FXS molecular diagnosis
Diagnosis of FXS was confirmed on DNA isolated from peripheral blood leucocytes by using standard procedures; PCR and Southern blot analysis were performed as detailed in Tassone et al. (2008).
Results
One hundred seventy-six blood spots (144 from populations with ID/ASD and 32 from known fragile X families) were screened for the presence of an expanded FMR1 allele. One full mutation (one male) (1/144) was identified within the ID population, and six full mutations (six females) and seven premutation individuals (two males, five females) were identified in families with a history of FXS (Fig. 1). Thus, prevalence of FXS full mutation in this high-risk population from Central Java, Indonesia, is 4.0% (1.1% in males and 7.1% in females; 95% confidence interval (2.0%, 8.1%) in agreement with reports from previous studies in other populations) (Sutherland, 1985; Syrrou et al., 1998; de Vries et al., 1999; Faradz et al., 1999; Pouya et al., 2009). However, the FXS full mutation was 0.72% (1/139) in the ID populations alone.

The FMR1 gene allele size distribution in both genders ranged between 10 and 51, with a modal number of 30 CGG repeats (25.0%), followed by 29 CGG repeats (21.2%). Interestingly, 3% and 3.4% of the alleles contained 35 and 36 CGG repeats, respectively, as previously reported in an Asian population (Zhong et al., 1994; Chiang et al., 1999; Faradz et al., 2001). Allele size distribution is shown in Figure 2.

Allele size distribution from the 176 subjects (92 men and 84 women) screened. The most common alleles in this population were 30 and 29 CGG repeats. An increased prevalence for 35 and 36 CGG repeats was also observed.
Follow-up studies to confirm FXS diagnosis were performed on those subjects found to be carriers of an FMR1 expanded allele during the blood spot screening process. Additional family members of those who had screened positive were also tested for the FXS mutation. Fragile X diagnosis was confirmed in one full mutation subject among the ID group, in addition to an uncle and a cousin. Among three families with known cases of FXS, 14 expanded alleles were identified. Confirmatory diagnosis was performed by Southern Blot/PCR analysis as depicted in Figure 3. Detailed results of individuals with an expanded FMR1 allele from known fragile X families are presented in Table 1.
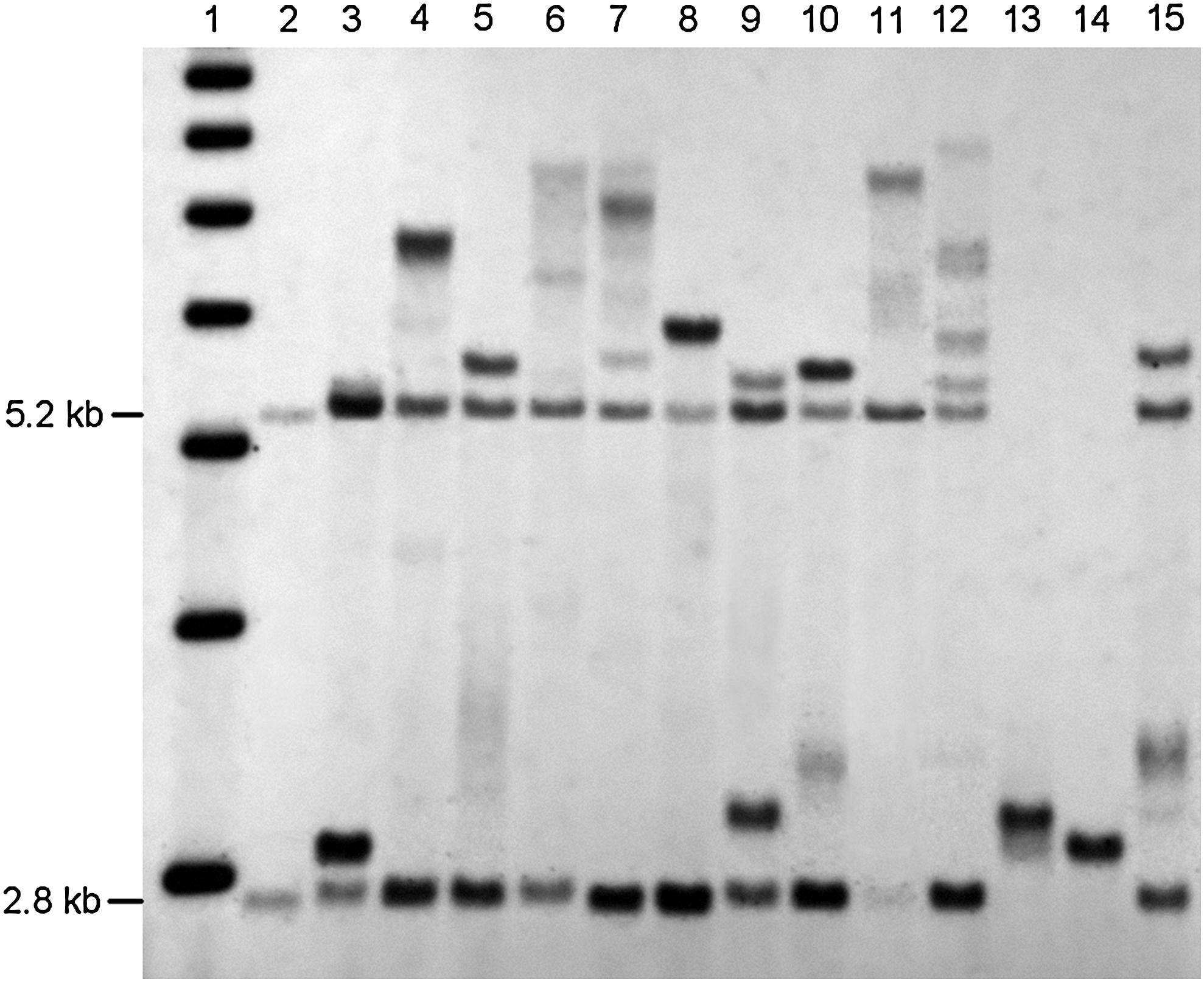
Diagnosis of FXS was confirmed by Southern Blot analysis in 13 subjects identified through the blood spot screening. DNA was digested with Eco RI and Nru I, and stB 12.3 probes were used (Tassone et al. 2008). The 1 kb ladder markers is show in lane1. Lane 2: normal female control showing a normal unmethylated band (2.8Kb) and normal methylated band (5.2Kb). Lanes 3, 5, 9, 10, and 15: premutation females. Lanes 4, 6, 7, 8, 11, and 12: full mutation females. Lanes 13 and 14: premutation male.
C* New FXS case from ID and or autism population.
M, male; F, female; FXS, fragile X syndrome; ID, intellectual disability.
Discussion
A number of studies have been carried out in populations of individuals with IDs, with a prevalence varying from ∼1% to 6.3% (Sutherland, 1985; Syrrou et al., 1998; de Vries et al., 1999; Faradz et al., 1999; Pouya et al., 2009). A previous study in Indonesia showed an FXS prevalence of 1.9% among the ID population (Faradz et al., 1999).
We present the first blood spot screening for FXS in a high-risk population in Indonesia by using a new approach that is capable of screening for FMR1 mutations throughout premutation and the full mutation range in both males and females. This screening approach is affordable, effective, and less time consuming compared with the standard diagnostic methods for FXS, and, therefore, feasible for large population screening. Results of this screening found 1 full mutation allele out of 139 subjects (0.72%) with ID, which is lower than the prevalence previously described in another study (1.9%) (Faradz et al., 1999) among 254 children with ID, likely due to their smaller sample size.
The most common alleles contain 30 and 29 CGG repeats, which is concordant with our previous studies (Faradz et al., 2001) among a Chinese population (Zhong et al., 1994) and among a non-Caucasian population (Kunst et al., 1996; Faradz et al., 2001). An allele frequency of 28 CGG repeats was also common in the Asian population. In 1999, Chiang et al. reported 45% of individuals carrying an allele of 28 CGG repeats, among a representative Chinese population (Chiang et al., 1999). Interestingly, a minor peak was found in 3% and 3.4% of alleles with higher CGG-repeat numbers (35 and 36). A previous study done in Indonesia reported a frequency of 8.7% for alleles with 36 CGG repeats, whereas higher frequencies were reported for alleles with 34, 35, and 36 CGG repeats in an Asian population (Zhong et al., 1994; Chiang et al., 1999; Faradz et al., 2001).
A recent report showed evidence of broad clinical involvement in FMR1 gene mutations reported among premutation and gray zone alleles (Hall et al., 2006; Loesch et al., 2009) including Idiopathic Parkinson's diseases, ASD and ADHD, FXPOI, and FXTAS (Tassone et al., 2000; Jacquemont et al., 2003; Goodlin-Jones et al., 2004; Jacquemont et al., 2004; Sullivan et al., 2005; Toft et al., 2005; Kraff et al., 2007; Cilia et al., 2009). Thus, a robust screening method is needed to accommodate future directions of early intervention and anticipation. We have performed our novel blood spot screening method on a high-risk population in Indonesia to demonstrate the validity of this screening tool for the diagnosis of FXS, which is especially valuable in locations where genetic testing is virtually inaccessible.
Footnotes
Acknowledgments
This work was supported by the National Institutes of Health (R01 HD02274; FT). The authors thank all the participants and their families for their contributions. They also thank Lidia Tilehun for her technical assistance. The first author is the addressee of an Excellent Scholarship Program of The Bureau of Planning and International Cooperation, Ministry of National Education, Government of Indonesia.
This work is dedicated to the memory of Matteo.
Disclosure Statement
No competing financial interests exist.