
Abstract
A reciprocal translocation between chromosomes 9 and 22 creates oncogenic BCR/ABL fusion in the breakpoint region of the derivative chromosome 22. The aim of this study was to evaluate the importance of atypical fluorescence in situ hybridization (FISH) signal patterns in pediatric and adult acute lymphoblastic leukemia (ALL) cases. We evaluated t(9;22) translocation in 208 cases with ALL (294 tests), including 139 childhood and 69 adult cases by FISH technique using BCR/ABL extra signal (ES) probe. FISH signal patterns observed in pediatric ALL cases were as follows; Major-BCR/ABL (M-BCR/ABL) (1.4%), minor-BCR/ABL (m-BCR/ABL) (3.6%), trisomy 9 (4.3%), trisomy 22 (4.3%), trisomy or tetrasomy of both chromosomes 9 and 22 (2.9%), monosomy 9 (1.4%), monosomy 22 (0.7%), ABL gene amplification (1.4%), derivative chromosome 9 deletion (1.4%), and extra copies of the Philadelphia chromosome (1.4%). FISH signal patterns observed in adult ALL cases were as follows; M-BCR/ABL (5.8%), m-BCR/ABL (11.6%), two different cell clones with major and minor BCR/ABL signal pattern (2.9%), extra copies of Philadelphia chromosome (4.3%), derivative chromosome 9 deletion (1.4%), trisomy 9 (2.9%), tetraploidy (1.4%), monosomy 9 (1.4%), trisomy 22 (1.4%), and coexistence of both trisomy 22 and monosomy 9 (1.4%). Trisomy 9, trisomy 22, and polyploidy of chromosomes 9 and 22 were specific atypical FISH signal patterns for childhood B cell acute lymphoblastic leukemia (B-ALL) patients. However, monosomy 9 and ABL gene amplification were highly specific for childhood T cell acute lymphoblastic leukemia (T-ALL) patients. Our report presents the correlation between atypical FISH signal patterns and clinical findings of a large group of ALL cases.
Introduction
A
t(9;22) translocation, which is detectable in chronic myelogenous leukemia (CML) cases with a frequency of 95% (Mohr et al., 2001), can be observed in about 2%-4% of pediatric acute lymphoblastic leukemia (ALL) (Nashed et al., 2003), and in about 15%-30% of adulthood ALL cases (Faderl et al., 1998; Yahata et al., 2000).
Conventional cytogenetics methods are commonly used for characterization of the primary and secondary chromosomal aberrations in hematological malignancies. However, banding cytogenetics is not effective for detection of chromosomal aberrations in some situations such as poor chromosome morphology, few metaphases of tumor cells, and undetectable chromosomal abnormalities. Therefore, the fluorescence in situ hybridization (FISH) technique plays an important role in determination of specific chromosomal abnormalities in hematological malignancies (Nordgren A., 2003; Kolialexi et al., 2005). Different FISH probes with different properties can be used for determination of the t(9;22) translocation including; BCR/ABL dual color single fusion, BCR/ABL dual color/dual fusion, and LSI BCR/ABL extra signal (ES) probes. LSI BCR/ABL ES probe decreases the false-positive results, allows the determination of the minor BCR/ABL fusion, and simultaneously detects derivative 9q deletions. Thus, this probe is preferable for FISH studies in hematological malignancies (Mohr et al., 2001; Cohen et al., 2003).
In this report, we present typical and atypical FISH patterns observed during ES-FISH studies for t(9;22) detection in 208 ALL cases including 139 childhood and 69 adult cases.
Materials and Methods
Study population
139 newly diagnosed [diagnosis of ALL was made according to the morphological and cytochemical criteria of the French-American-British classification and immunophenotyping] pediatric ALL cases (83 male/56 female; ratio was 1.48:1) included in this study were recruited between 2003 and 2010. The mean age was 7.14 years ranging between 3 months of age and 18 years. Pediatric patients were treated according to ALL-BFM protocols. Sixty-nine newly diagnosed consecutive (between years 2003-2010) adult ALL cases (42 male/27 female; ratio was 1:0.64) were also evaluated by ES-FISH for BCR/ABL rearrangement. The mean age of the adult patients was 42.49 ranging between 19 and 76 years. Adult patients were treated mainly by Hyper-CVAD chemotherapy regimens and in Ph (+) patients tyrosine kinase inhibitors were added.
Conventional cytogenetics analysis
Cytogenetic investigations were performed on bone marrow cells using conventional GTG banding analyzes for all cases at the time of diagnosis. At least 25 metaphases were analyzed from each case. Karyotypes were described according to the International System of Human Cytogenetic Nomenclature (ISCN 2009).
FISH analysis
We performed FISH studies (294 tests) using LSI BCR/ABL ES probe according to the manufacturer's instructions (Vysis, Downer Grove, IL). Data were collected using a fluorescence microscope (Zeiss Axioplan) equipped with a CCD camera (Photometrics Sensys) run by MacProbe software v.4.1. A total of 200 interphase nuclei were analyzed for the presence of fusion signals by two different observers for each case. The FISH pattern of Ph negative nuclei with the use of BCR/ABL ES probe consists of the following signals; two green (BCR) and two orange (ASS-ABL) signals. The expected hybridization pattern of M-BCR/ABL positive nuclei consists of one fusion (BCR/ABL), one green and two orange signals (ABL on intact chromosome 9 and ASS on derivative chromosome 9). The expected hybridization pattern of m-BCR/ABL is; two fusion (one on the derivative chromosome 9 and the other on the derivative chromosome 22), one green (BCR), and one orange (ABL on intact chromosome 9) signal. Other signal patterns were considered as atypical FISH signal patterns.
Results
Typically, major and minor-BCR/ABL fusion signal patterns were observed in 2 (1.4%) and 5 (3.6%) of the 139 pediatric ALL cases, respectively. Atypical signal patterns observed in 25 pediatric ALL cases were as follows: trisomy 9 in six cases (4.3%), trisomy 22 in six cases (4.3%), trisomy or tetrasomy of both chromosomes 9 and 22 in four cases (2.9%), monosomy 9 in two cases (1.4%), monosomy 22 in one patient (0.7%), ABL gene amplification in two cases (1.4%), derivative chromosome 9 deletion in two patients (1.4%), and extra copies of the Philadelphia chromosome in two patients (1.4%) (Table 1; Fig. 1). Poliploidy, trisomy 22, and trisomy 9 were strictly associated with B cell acute lymphoblastic leukemia (B-ALL) immunophenotype, whereas monosomy 9 and ABL amplification were associated with T cell acute lymphoblastic leukemia (T-ALL) in childhood ALL cases. Trisomy 9 and trisomy 22 FISH signal patterns seem to be associated with good prognosis, whereas poliploidy and ABL amplification were associated with poor prognosis in childhood ALL.
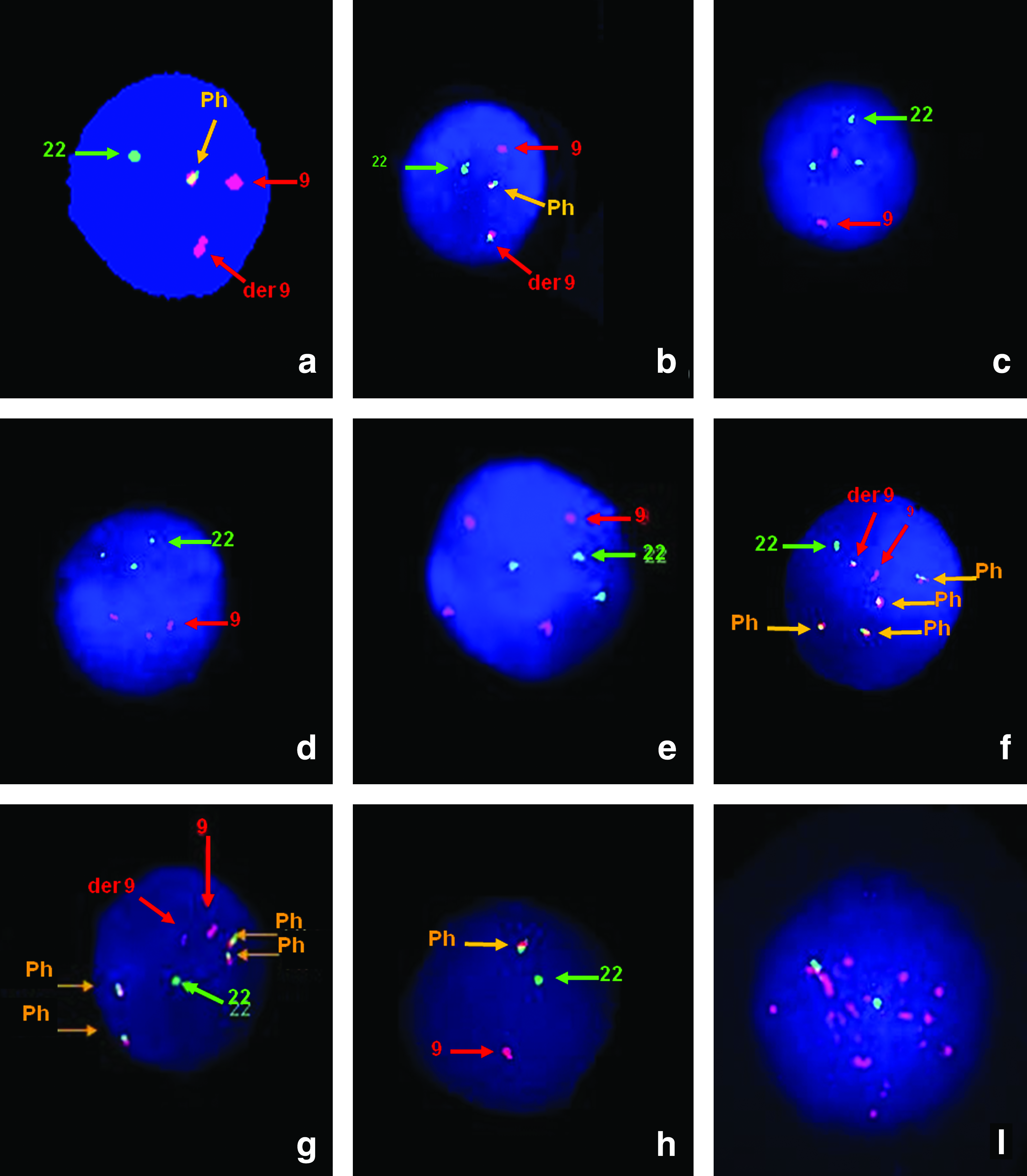
Red signal indicates ASS/ABL locus on chromosome 9, green signal indicates BCR locus on chromosome 22.
Typically BCR/ABL fusion was observed in 12 of 69 adult ALL cases (17.4%). Eight of these cases had m-BCR/ABL (11.6%), whereas four cases (5.8%) had a M-BCR/ABL signal pattern. Two different cell clones with major and minor BCR/ABL signal pattern were observed in two patients (2.9%). Atypical FISH signal patterns observed in ten adult ALL cases (14.4%) were as follows: extra copies of Philadelphia chromosome in three cases (4.3%), derivative chromosome 9 deletion in one case (1.4%), trisomy 9 in two cases (2.9%), tetraploidy in one case (1.4%), monosomy 9 in one case (1.4%), trisomy 22 in one case (1.4%), and trisomy 22 and monosomy 9 in one case (1.4%).
Conventional cytogenetic analysis failed in 23 out of the 36 cases with atypical FISH signal pattern. Five patients had normal karyotype and FISH findings were in accordance with conventional cytogenetic results in eight cases. Atypical FISH signal patterns were used as disease specific molecular cytogenetic markers for monitoring the disease after applying chemotherapy regimens. FISH studies were done on bone marrow samples obtained during remission/relapse situations in 14 cases with ALL patients.
Discussion
FISH is a fast and cost-effective technique to evaluate BCR/ABL fusion in hematological malignancies including ALL and CML. Major and minor BCR/ABL fusions can be discriminated from each other as they create different signal patterns in ES-FISH studies (Lee et al., 2001). We observed BCR/ABL fusion with a frequency of 7.9% and 21.7% in pediatric and adult ALL patients, respectively. Philadelphia chromosome detection frequency was recorded as approximately 2%-4% and 30% for childhood and adult ALL patients in the literature (Westbrook et al., 1992; Yahata et al., 2000). Our findings were in concordance with the literature.
In addition to the discrimination of the major and minor BCR/ABL fusions, extra copies of the BCR/ABL fusion, derivative chromosome 9 deletions, isochromosome 9q, polysomies and monosomies of chromosomes 9 and/or 22, ABL gene amplifications were detected by ES-FISH as atypical interphase FISH patterns.
In our study, the most common two atypical FISH signal patterns were trisomy 9 and trisomy 22 in childhood ALL. This finding is concordant with the previously published reports (Nordgren et al., 2002; Harrison et al., 2005; Pérez-Vera et al., 2008). The other atypical FISH signal pattern is derivative chromosome 9q34 deletion. Recently, two reports have clearly showed that incidence of derivative chromosome 9q34 deletion both in childhood and adult ALL is similar to that observed in CML (Specchia et al., 2003; Robinson et al., 2005). Our findings also support these findings. Amplification of ABL signals in pediatric T-ALL is a very rare phenomenon being first reported by Kim et al., (2004). Three research groups have reported that ABL amplifications could be observed with a frequency of 1%-5.8% in T-ALL patients (Barber et al., 2004; Graux et al., 2004; Harrison et al., 2005). Molecular studies have revealed that these amplifications associated with the formation of a NUP214-ABL1 fusion. We present two further pediatric T-ALL patients with ABL gene amplification in this report indicating that ABL gene amplification is a different entity in pathogenesis of T-ALL.
Atypical signal patterns and their frequency showed differences between adult and childhood ALL cases. Different from childhood ALL patients, extra copies of BCR/ABL fusion, derivative chromosome 9 deletions, and trisomy 9 were the most frequent atypical signal patterns observed in adult ALL patients. This result clearly shows that childhood and adult ALL have different cytogenetic routes. Primo et al., (2005) showed that existence of secondary Philadelphia chromosome is a frequent genetic alteration in adult BCR/ABL positive ALL patients with a frequency of 30%. Monosomy 9, trisomy 22, coexistence of trisomy 9 and monosomy 22 might be observed in bone marrow samples obtained from adult ALL patients. We detected two adult ALL patients having both of the major and minor BCR/ABL signal patterns in different cell clones. Coexistence of the p210 and p190 transcripts have been reported in a frequency 3% of adult patients with ALL (Gleissner et al., 2002). The exact mechanism of the coexpression of these two transcripts in adult ALL is not known. However, Van Rhee et al. (1996) speculated that coexpression of both transcripts might result from alternative splicing of M-BCR/ABL or acquisition of a second Philadelphia chromosome with a different breakpoint (van Rhee et al., 1996). However, our cases had two different cell clones displaying major and minor BCR/ABL signal patterns. Resembling our case, Agirre et al. (2005) have reported a CML patient coexpressing both transcripts derived from two different cell lines presenting major and minor BCR/ABL FISH signal pattern. In our case, after treatment only the cells with p190 FISH signal pattern were detected with a frequency of 12% whereas no cells with p210 FISH signal pattern were observed. In the case reported by Agirre et al., (2005) follow-up findings were similar to our findings showing that cells with p190 transcript were more resistant to apoptosis.
Distribution of atypical FISH signal patterns according to immunophenotype of the ALL in our study population are also interesting and showed some specific associations between these parameters. Our results showed that trisomy 9, trisomy 22, and polyploidy of chromosomes 9 and 22 were highly specific and very frequent atypical FISH signal patterns for childhood B-ALL patients whereas monosomy 9 and ABL gene amplification were most common for childhood T-ALL patients. As seen in Table 2, clinical follow-up of the patients suggest that some of these atypical FISH signal patterns might be important in prognosis. Trisomy 9 and trisomy 22 FISH signal patterns seem to be associated with good prognosis, whereas poliploidy and ABL gene amplification were associated with poor prognosis in childhood ALL. Also, trisomy 9 and coexistence of both M-BCR/ABL and m-BCR/ABL FISH signal patterns might be poor prognostic markers in adult ALL.
No metaphase obtained.
NF, no follow up; FISH, fluorescence in situ hybridization; ALL, acute lymphoblastic leukemia; CML, chronic myelogenous leukemia; B-ALL, B cell acute lymphoblastic leukemia; T-ALL, T cell acute lymphoblastic leukemia.
Conventional cytogenetic analysis of bone marrow cells has limitations for detection of chromosomal abnormalities due to low mitotic index and poor quality of metaphases in ALL (Zemanova et al., 2005). In this study, we observed atypical FISH signal patterns of chromosomes 9, 22 or Philadelphia chromosomes during FISH analysis in 23 ALL patients where cytogenetic analysis were unsuccesful. Determination of these atypical signal patterns allowed us to monitor treatment outcomes in our cases indicating the importance of the atypical FISH signal patterns observed during FISH analysis.
As a result, in addition to detection of minor and major BCR/ABL fusions with improved specificity in minimal residual disease, ES-FISH system allows us to detect the other numerical and structural aberrations of chromosomes 9 and 22 as atypical signal patterns. Frequencies of these atypical FISH signal patterns were strictly associated with the ages of the patients and immunophenotype of the leukemia cells. These atypical FISH signal patterns are important molecular cytogenetics markers for monitoring the disease progression. Our results suggest that these atypical FISH signal patterns also might be important prognostic markers for patients. In order to clarify the prognostic significance of these atypical FISH signal patterns, studies with larger cohorts and follow-up of the cases with atypical signal patterns are needed.
Footnotes
Acknowledgment
This study was supported by Akdeniz University Scientific Research Project Management Unit.
Disclosure Statement
The authors of this paper have no conflicts of interest, including specific financial interests, relationships, and/or affiliations relevant to the subject matter or materials included.