
Abstract
Background and Aim: Recurrent pregnancy loss (RPL) is a heterogeneous disorder that has been associated with antiphospholipid syndrome and other prothrombotic parameters. We aimed to investigate the prevalence of 12 thrombophilic gene mutations in RPL couples in the current results. Method: In a total of 543 Turkish women with RPL and 327 of their male partners (870 individuals with RPL), and a control group of 106 fertile couples (control) were analyzed for factor V leiden (FVL), factor V H1299R, factor II prothrombin G20210A, FXIII V34L, β-fibrinogen −455G>A, plasminogen activator inhibitor-1 (PAI-1), GPIIIa L33P (HPA-1 a/b L33P), methylenetetrahydrofolate reductase (MTHFR) C677T, MTHFR A1298C, ACE I/D, Apo B R3500Q, and Apo E genes. Results: The overall, heterozygous and/or homozygous point mutations in FVL - FVR2, ApoE2, PAI-1, MTHFR C677T - A1298C, and ACE genes were associated with RPL. There was no meaningful association between RPL and other studied genes. Conclusion: The homozygosity of 4G in PAI-1 and MTHFR C677T genes in women with RPL, and heterozygosity of FVL, FVR2, ACE, and ApoE2 genes in both parents play crucial role in RPL and should be considered as a risk factor in RPL. Current results showed that RPL is related to combined parental (not only maternal) thrombophilic gene mutations.
Introduction
R
In the present study, we compare the prevalence of 12 thrombophilic gene mutations in a series of patients with two or more consecutive, first-trimester losses and fertile couples with no history of miscarriages.
Material and Methods
Patients
The current study was performed in both gynecology clinics and genetic departments at Cumhuriyet University Hospital and Canakkale Onsekiz Mart University Hospital. All applications were approved by the local ethics committee of Cumhuriyet University and informed consent was obtained from all of the subjects. Eight hundred and seventy individuals (543 women and 327 men) with unexplained pregnancy losses and 106 fertile couples were analyzed in the current prospective case-control study between June 2004 and August 2010. The 543 women with a history of RPL, defined as two or more consecutive early RPL at 5-12 weeks of gestation (determined either by the ultrasound or last menstrual period) by a single spouse and with no history of full term pregnancies before or after the RPLs during the study period, were recruited as the RPL study group. Three hundred and twenty-seven RPL male partners were also included. Women and their partners (106 couples) with no history of pregnancy loss and at least one normal pregnancy, from the same two geographic areas, were used as a control group. Chromosome analyses were performed in all RPL and control couples. Women with RPL were examined by ultrasonography or hysterosalpingogram for detection of possible abnormalities of the genital tract and peripheric blood sampling made for immunologic risk factors including antiphospholipid antibodies, antinuclear antibodies, antithyroid antibodies, and lupus anticoagulant. The women who had anatomic abnormalities, endocrinologic dysfunction, autoimmune disease, and urogenital infections were excluded.
Genes
The target genes and their pathogenic mechanisms were stated in our previous results (Yenicesu et al., 2010). Twelve thrombophilic markers of thrombophilic genes; factor V G1691A (FVL) (Castoldi et al., 2000; Ozcan et al., 2001; Pihusch et al., 2001; Buchholz and Thaler, 2003; Behjati et al., 2006; Coulam et al., 2006; Vettriselvi et al., 2008; Yenicesu et al., 2010; Hopmeier et al., 2008), factor V H1299R (Kutteh et al., 1999; Castoldi et al., 2000; Buchholz and Thaler, 2003), factor II prothrombin G20210A (prothrombin G20210A) (Castoldi et al., 2000; Ozcan et al., 2001; Buchholz and Thaler, 2003; Coulam et al., 2006; Goodman et al., 2006; Jivraj et al., 2006; Vettriselvi et al., 2008; Meng et al., 2011), factor XIII V34L (FXIII V34L) (Pasrinen et al., 1998; Kohler et al., 1999; Kakko et al., 2002; Buchholz and Thaler, 2003; Dossenbach-Glaninger et al., 2003; Goodman et al., 2006; Coulam et al., 2006) β-fibrinogen −455G>A (β-fibrinogen) (Behague et al., 1996; Kohler et al., 1999; Pihusch et al., 2001; Kakko et al., 2002; Coulam et al., 2006; Meng et al., 2011), plasminogen activator inhibitor-1 (PAI-1) (Eriksson et al., 1995; Pasrinen et al., 1998; Sartori et al., 1998; Glueck et al., 2000; Dossenbach-Glaninger et al., 2003; Buchholz and Thaler, 2003; Wolf et al., 2003; Coulam et al., 2006; Meng et al., 2011), GPIIIa L33P (HPA-1 a/b L33P) (Nelen et al., 2000; Pihusch et al., 2001; Zetterberg et al., 2002; Bojesen et al., 2003), MTHFR C677T (Pasrinen et al., 1998; Kohler et al., 1999; Castoldi et al., 2000; Pihusch et al., 2001; Ozcan et al., 2001; Reznikoff-Etiévant et al., 2001; Finan et al., 2002; Bojesen et al., 2003; Buchholz and Thaler, 2003; Hohlagschwandtner et al., 2003; Wolf et al., 2003; Dudding and Attia, 2004; Behjati et al., 2006; Coulam et al., 2006; Jivraj et al., 2006; Ayadurai et al., 2009; Yenicesu et al., 2010; Meng et al., 2011), MTHFR A1298C (Nelen et al., 2000; Zetterberg et al., 2002; Coulam et al., 2006; Meng et al., 2011), ACE I/D (Fatini et al., 2000, 2003; Finan et al., 2002; Buchholz and Thaler, 2003; Hohlagschwandtner et al., 2003; Yenicesu et al., 2010), Apo B R3500Q (Hohlagschwandtner et al., 2003), and Apo E (E2, E3, and E4) (Goodman et al., 2009; Niu et al., 2009; Ozornek et al., 2010) were analyzed in the current results.
Mutation analysis
Peripheral blood tissues containing ethylenediaminetetraacetic acid from patients and the control group were used for genomic DNA isolation. Total genomic DNA was extracted from peripheral blood samples by the Magna Pure Compact (Roche) and Invitek kit extraction techniques (Invitek®; Invisorb spin blood). Twelve thrombophilic genes (FVL, FV H1299R, prothrombin G20210A, FXIII V34L, β-fibrinogen −455G>A, PAI-1, GPIIIa L33P, MTHFR C677T, MTHFR A1298C, ACE I/D, Apo B, and Apo E) were simultaneously amplified in a biotin-labeled single multiplex amplification reaction (Viennalab®; PGX-HIV StripAssay) which is based on the reverse-hybridization principle automatically and by Real-Time PCR, LightCycler 2.0 methods (Roche). The multiple polymerase chain reaction (PCR) was performed in a Perkin Elmer 9600, and the profile consisted of an initial melting step of 2 min at 94°C, followed by 35 cycles of 30 s at 94°C, 30 s at 61°C, and 30 s at 72°C and a final elongation step of 7 min at 72°C. A high portion of samples was also analyzed by real-time PCR technique (LightCycler 2.0; Roche). Briefly, LightCycler FastStart DNA Master HybProbes, master mix (water, PCR-grade, MgCl2, stock solution, Primer mix, and HtbProbe mix), and DNA template were used for real-time amplification. The following were the amplification conditions for 45 cycles: denaturation at 95°C for 10 s, annealing for 5-20 s, extension at 72°C, melting curve step with denaturation at 95°C, annealing for 30 s, melting at 95°C, and a cooling step at 40°C for 30 s. The software program LightCycler 2.0 (Roche) was used for detection of the mutated and normal genotype profiles of target genes in the current RPL and control couples.
Statistical analysis
Statistical analysis was performed using SPSS version 16 (SPSS). The frequencies of homozygous and heterozygous thrombophilic gene mutations and the frequencies of allelic mutations in female and male participants in the two groups were compared using chi-square analysis. In calculating the allelic mutations, a heterozygous mutation was considered as one-gene mutation and a homozygous mutation was considered as two gene mutations. A value of p<0.05 was considered as statistically significant. The statistically significant mutation profiles are discussed in the current report.
Results
Thrombophilic gene mutations have been shown to be a risk factor for RPL. We have previously reported that 3 out of the 12 thrombophilic mutations studied, PAI-1 4G/5G, FVL, and homozygous MTHFR C677T, correlated significantly with RPL when compared with fertile controls. The current results show the 12 thrombophilic mutation profiles in RPL and fertile controls from two different populations in Turkey. The demographic details and outcomes of previous pregnancies of the study subjects in the RPL and control groups were summarized in Table 1. The mean age of the female partners experiencing RPL was 27.8±2.1 years and male partners was 29.8±2.2 years and the number of previous miscarriages ranged from 2 to 10. In control couples, the mean age of the women was 28.9±2.2 and men was 32.9±1.1 and no history of miscarriage was detected (Table 1). No structural and numerical chromosome abnormalities were detected in the RPL and control group individuals in the fully karyotype analyses. No significant differences in the prevalence of the factor II, factor XIII V34L (FXIII V34L), β-fibrinogen −455G>A, GPIIIa L33P (HPA-1 a/b L33P), and Apo B R3500Q mutations were found in RPL couples and controls.
p>0.05.
RPL, recurrent pregnancy loss.
The frequencies of allelic mutations for FVL, FVR2, MTHFR C677T, MTHFR A1298C, PAI-1 5G/4G, ACE I/D, and Apo E in the RPL women (20.02%, 13.3%, 57.4%, 63.0%, 83.2%, 86.9%, and 35.0%), respectively, were higher than in the fertile control women (1.9%, 2.8%, 28.3%, 33.0%, 68.0%, 68.1%, and 21.7%) and they were statistically significant (Tables 2-6). The frequency of allelic mutation for FVL was 20.02% in the RPL women and 1.9% in the control fertile women (Table 2) (p<0.0001). The rest of thrombophilic gene mutations were the same as control women. The frequencies of allelic mutations for FVL, FVR2, MTHFR C677T, MTHFR A1298C, PAI-1 5G/4G, ACE I/D, and Apo E in the RPL men (19.2%, 17.8%, 55.6%, 56.0%, 89.3%, 81.3%, and 36.7%, respectively) were higher than in the fertile control men (2.9%, 0.0%, 25.5%, 35.0%, 64.1%, 67.9%, and 20.8%) and they were statistically significant (Fig. 1) (Tables 2-6).
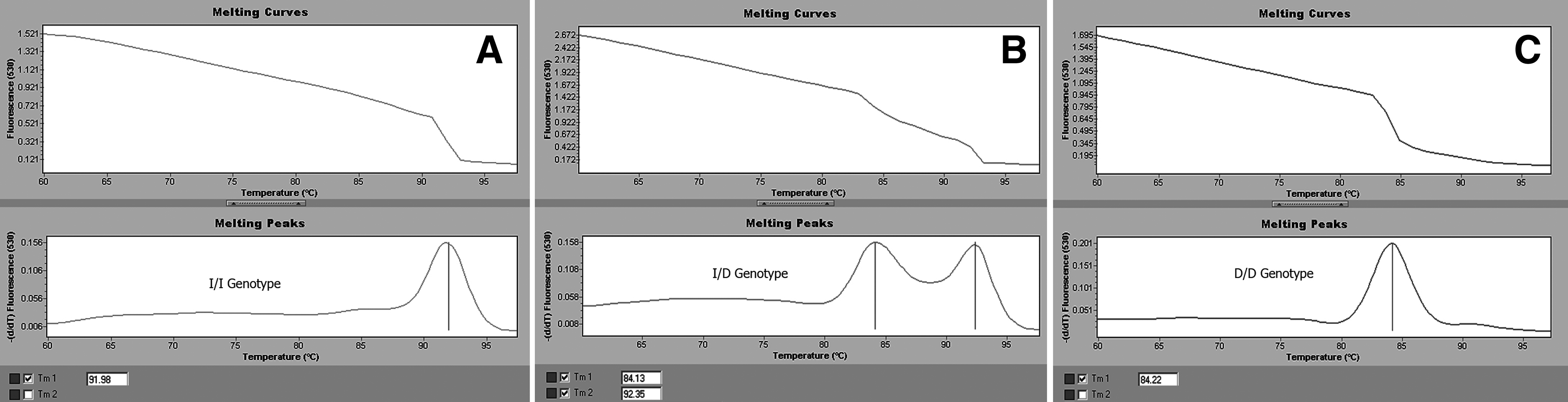
Real-time genotype profiles (melting curves and peaks) of ACE I/D polymorphism. Homozygous I/I genotype in normal healthy control case
Odds ratio for FVL=0.10 (0.03-0.24), p<0.0001.
Odds ratio for FVR2=0.08 (0.02-0.27), p<0.0001.
F, female; M, male; T, total; FVL, factor V leiden.
Odds ratio for C677T=0.36 (0.26-0.51), odds ratio for A1298C=0.36 (0.24-0.47).
The frequency of allelic mutation for FVL was 19.2% in the RPL men, but there was no mutation in the control men (p<0.0001). The frequencies of allelic mutations for FV H1299R, prothrombin G20210A, β-fibrinogen −455G>A, MTHFR A1298C, and Apo E were similar in the RPL and control men (Table 2). The total frequencies of allelic mutations in RPL subjects were 19.7% (176/870), 15.0% (131/870), 56.7% (489/870), 60.3% (525/870), 85.5% (744/870), 84.8% (738/870), and 35.6% (310/870) for FVL, FVR2, MTHFR C677T, MTHFR A1298C, PAI-1 4G/5G, ACE I/D, and Apo E, respectively. The total frequencies of allelic mutations in fertile couple subjects were 2.0% (5/212), 1.4% (3/212), 26.9% (57/212), 34.0% (72/212), 66.0% (140/212), 68.3% (145/212), and 21.3% (45/212) for FVL, FVR2, MTHFR C677T, MTHFR A1298C, PAI-1 4G/5G, ACE I/D, and Apo E, respectively (Tables 2-6). To further define the relationship between some specific target genes and RPL, we also evaluated the allelic frequencies of 4G for PAI-1, D for ACE, C677T and A1298C for MTHFR, and E4 for Apo E in two different populations of women experiencing RPL.
The frequency of E3/E2, E3/E4, and E2/E4 profiles for Apo E was 20.9%, 12.8%, and 1.9%, respectively, in the RPL couples, and 10.9%, 10.4%, and 0.0% in fertile couples (Table 6). While ApoE3 allele frequency was 0.81 in RPL and 0.89 in fertile couples, the ApoE2 frequency was 0.11 for RPL and 0.06 for fertile couples (Table 6) (p<0.0001). ApoE4 allele frequency was detected as 0.08 for RPL and 0.05 for fertile couples in both studied populations. The frequencies of heterozygous mutations for PAI-1, MTHFR C677T, MTHFR A1298C, ACE I/D, and Apo E were significantly higher in RPL couples when compared with fertile control couples (p<0.0001). The frequency of homozygous mutation for PAI-1 was significantly higher in RPL men compared with control men (p<0.0001) (Table 4). The frequency of homozygous mutation for MTHFR C677T was 15.9% in the RPL men, but no homozygous mutation was detected in the control men (p<0.0001) (Table 3).
The presented preliminary results showed that ApoE2 allele profile may contribute to the thrombophilic risk factors for RPL. Increased T allele frequency of C677T polymorphism in MTHFR gene was detected in RPL patients (0.36) when compared with fertile couples (0.13) (Table 3). The second common mutation for the MTHFR gene is A1298C, resulting in a 40% reduction in the enzyme activity. Also the present results showed increased C allele frequency of A1298C mutation in RPL patients (0.37) when compared with the fertile couples (0.17). Differences in both common mutated alleles in the MTHFR gene were statistically significant (p<0.0001). An insertion-deletion mutation is a 287-bp fragment loss in intron 16 of the ACE gene and is associated with enhanced conversion of angiotensin I to angiotensin II in plasma. For the ACE I/D gene, the frequency of heterozygous and homozygous mutations in RPL couples was significantly higher than the fertile couples (p>0.001) (Fig. 1; Table 5). D allele frequency was detected as 0.62 for RPL and 0.44 for fertile couples. The difference was statistically significant (p<0.0001) (Table 5). Current results also showed increased 4G allele frequency in RPL (0.55) when compared with healthy controls (0.38) (Table 4).
Discussion
The present study compares the prevalence of 12 thrombophilic gene mutations in a total of 870 individuals (543 women and 327 men) with RPL and 106 fertile couples (212 individual) from different regions (Sivas and Canakkale) of Turkey. The current results of RPL patients from two different populations showed that combined parental thrombophilic gene mutations play a crucial role in RPL. The thrombophilic mutations such as G1691A of factor V gene (FVL), FVR2, C677T of MTHFR gene (MTHFR C677T), ACE I/D, PAI-1 5G/4G, and ApoE2 are most extensively associated to RPL in the current study. Homozygous profile for the 4G allele of the PAI-1 gene is associated with overexpression of the gene and most possibly plays a crucial role in RPL as claimed by some researchers (Behague et al., 1996; Dizon-Townson et al., 1997; Hashimoto et al., 1999; Kohler et al., 1999; Younis et al., 2000; Pihusch et al., 2001; Kakko et al., 2002; Dossenbach-Glaninger et al., 2003; Coulam et al., 2006; Meng et al., 2011; Buchholz and Thaler, 2003). In the current results increased 4G allele frequency was detected in the RPL patients (0.55) when compared with fertile controls (0.38) (Table 4).
Our previous results showed that heterozygous mutations of FVL, FXIII V34L, GPIIIa L33P, ApoE4, and prothrombin G20210A and homozygous mutations of PAI-1 and MTHFR C677T were associated with RPL (Yenicesu et al., 2010). Current results also show the involvement of similar genes but different mutation rates for some of the studied thrombophilic genes that were reported in our previous report. It was found that the heterozygous mutations in FVL, FVR2 and the homozygous mutations of PAI-1 and MTHFR C677T and A1298C, ACE and Apo E (E2) genes were higher in couples with RPL in the current presented results. Current wide scale results showed us that not only FVL and FII G20210A point mutations are major inherited risk factors associated with RPL (Younis et al., 2000; Reznikoff-Etiévant et al., 2001; Finan et al., 2002; Rey et al., 2003; Dudding and Attia, 2004; Kovalevsky et al., 2004; Goodman et al., 2006; Yenicesu et al., 2010) but also some other specific parental thrombophilic gene mutations, such as FVL, FVR2, MTHFR, PAI-1, ACE, and ApoE2, have a crucial role in RPL. Altintas et al. have reported the frequencies of carriers of FVL in patients with RPL and controls were 7.9% and 7%, respectively (Altintas et al., 2007). Some reports suggested that there were no statistical differences in the prevalence of FVL and/or prothrombin G20210A between the patient and control groups (Dizon-Townson et al., 1997; Hashimoto et al., 1999; Kutteh et al., 1999; Pickering et al., 2001; Rai et al., 2001; Vettriselvi et al., 2008).
Other reports did not show any significant difference in the prevalence between recurrently aborting patients and controls for MTHFR mutations (Kutteh et al., 1999; Pihusch et al., 2001; Coulam et al., 2006). In our previous and current reports, expression of homozygous mutation in MTHFR C677T and heterozygous mutation in A1298C in couples with RPL were higher and conflicting with some other population reports (Blumenfeld and Brenner, 1999; Mtiraoui et al., 2006). Current results showed increased T allele frequency in C677T codon and C allele frequency in the second common mutation of A1298C codon in MTHFR gene in RPL couples. Homozygous 4G has been associated with PAI-1 concentrations higher than those associated with the insertion genotype (5G/5G), and hence with reduced fibrinolytic activity (Margaglione et al., 1997). The 4G mutation frequency was detected as 0.55 in current RPL and 0.38 in fertile couples. The difference was statistically significant (p<0.0001).
Some reports show association between the ACE D/D genotype and increased risk of thrombosis (Heby, 1995; Vaughan, 1998; Fatini et al., 2003; Mello et al., 2003). Similar results were detected in the current study. D allele frequency was detected as 0.62 for RPL and 0.44 for fertile couples. The difference was also statistically significant (p<0.0001) in RPL couples when compared with the current fertile couples. Fatini et al. also claimed the homozygous D allele in ACE gene polymorphism to be a stronger risk factor for RPL (Fatini et al., 2000; Fatini et al., 2003). On the other hand Buchholz et al. reported that the homozygosity for the D allele of ACE results in elevated PAI-1 concentration and thus is associated with an elevated risk of RPL in Caucasians (Buchholz and Thaler, 2003). Goodman et al. reported that 21.7% of patients with RPL had ApoE4 genotype profiles, when compared with the control women of 5.4% (Goodman et al., 2009) (p=0.036). Current results showed Apo E as a risk factor for RPL and ApoE2 gene frequency was statistically significant (not ApoE4) in our RPL couples when compared with the fertile couples (p<0.0001).
The embryonic phase recurrent miscarriages of current couples were associated with a significantly higher incidence of maternal heterozygosity for FVL, ApoE2, MTHFR, PAI-1, and ACE with combined parental mutations of ApoE2, ApoE4, MTHFR, PAI-1, and ACE genes. Our results support previous findings demonstrating combined mutagenic effects of thrombophilic gene mutations in RPL (Pasrinen et al., 1998; Castoldi et al., 2000; Ozcan et al., 2001; Dossenbach-Glaninger et al., 2003; Behjati et al., 2006; Jivraj et al., 2006; Hopmeier et al., 2008). Similar results that gained from large scale of RPL patients were also reported by Coulam et al. (2006) and Ayaduria et al. (2009). Not only maternal mutation profiles but also paternal combined specific gene mutations may contribute to RPL according to the presented results. So, it may be suggested that the combination of two or more thrombophilic gene mutations should be considered in the evaluation of high-risk conditions in couples with RPL.
Conclusion
Briefly, the homozygosity of 4G in PAI-1 and MTHFR C677T genes in women with RPL, and heterozygosity of FVL, FVR2, ACE, and ApoE2 and ApoE4 genes in both parents play crucial roles in RPL and should be considered as risk factors in RPL. Current results showed that the maternal mutated thrombophilic genes' profiles mainly have a potential risk for RPL but paternal mutation profiles in specific genes may also have a combined effect on RPL phenomenon. Study of mutations in a wide range of thrombophilic genes associated with the disease might be clinically useful as a marker to assess a couple's risk for RPL.
Footnotes
Disclosure Statement
No competing financial interests exist.