
Abstract
Aims: Two single nucleotide polymorphisms in the methylene tetrahydrofolate reductase (MTHFR) gene, 677C/T and 1298A/C, encode the thermolabile isoforms of the MTHFR enzyme that adversely affect the folic acid metabolic pathway. In the present study, these polymorphisms were investigated for their associations with the risk and prognosis of the renal cell carcinomas (RCCs) in Pakistani patients. Results: The study included 168 RCC patients and 178 controls. The polymorphisms were analyzed by the polymerase chain reaction-restriction fragment length polymorphism method. Statistical analysis revealed that the C-allele and homozygous C genotype of the MTHFR 1298A/C polymorphism were significantly correlated with the risk of RCCs (odds ratio [OR]=1.60; 95% confidence interval [CI]=1.1-2.34 and OR=3.26; 95% CI=1.27-8.37, respectively). The combined genotype analysis showed that the 677CC+1298CC combination greatly increased the susceptibility to RCCs (OR=8.34; 95% CI=2.7-25.7). The 677CT+1298AA and 677CC+1298CA combinations were also associated with an increased risk of RCC (OR=3.21; 95% CI=1.3-7.8 and OR=2.45; 95% CI=1.3-4.6, respectively). The combined genotype effects were also evident in a semiparametric expectation-maximization-based haplotype analysis. Conclusion: The results presented here indicate that the two MTHFR gene polymorphisms are significantly associated with the risk of RCCs in a cohort of Pakistani patients and may be useful as susceptibility markers in other populations of the world as well.
Introduction
T
The thermolabile isoforms of the MTHFR enzyme that arise due to genetic variations have significantly reduced specific activities resulting in a decreased concentration of methylTHF. Consequently, uracil is misincorporated into the DNA and the uracil-repair pathway gets activated. This pathway may lead to single- or double-strand breaks responsible for chromosomal instability, which is a hallmark of cancers in general (Blount et al., 1999). Simultaneously, the decreased methylTHF concentration leads to an accumulation of homocysteine, which results in a decreased methionine concentration and an eventual defect in the DNA methylation process (Skibola et al., 1999).
The locus of the MTHFR gene is on chromosome 1p36.3 (Goyette et al., 1994) and the two single nucleotide polymorphisms (SNPs) that are responsible for the thermolabile isoforms of the enzyme are MTHFR 677C/T and MTHFR 1298A/C. In the first polymorphism (dbSNP: rs1801133), a thymine (T) at the conventional position 677 of the MTHFR gene replaces a cytosine (C) resulting in an alanine-to-valine missense substitution. In the second polymorphism, that is, MTHFR 1298A/C (dbSNP: rs1801131), at the conventional position 1298 of the gene, a cytosine (C) is substituted for an adenine (A) leading to a glutamic acid-to-alanine change (Wang et al., 2009).
These two polymorphisms have shown associations with various diseases such as cardiovascular diseases, hypertension, and cancers, including the leukemias, bladder cancer, and colorectal cancers (Online Mendelian Inheritance in Man [OMIM]; www.ncbi.nlm.nih.gov/omim/607093). In case of the association of these polymorphisms with the risk of renal cell carcinomas (RCCs), a recent study from Iran (Safarinejad et al., 2011) and two studies from Europe have been published. The study from Iran reports the individual associations of these polymorphisms with the risk of clear cell RCCs in men. In the case of the studies from Europe, one study reports an increased risk of kidney and bladder cancers with the MTHFR 677TT genotype (Heijmans et al., 2003). The other study reports that at least one variant T-allele for the MTHFR 677C/T polymorphism is associated with a higher risk of RCC; however, neither MTHFR 1298A/C, nor the haplotypes comprising these two markers show any association with the risk for RCC (Moore et al., 2008). Another study from Japan (Sakano et al., 2010) has shown that the MTHFR genotypes and haplotypes may serve as gender-specific markers for the prediction of the clinical course of clear cell RCCs. It should be emphasized that the genetic association studies depend a great deal upon the population from whom the cases and controls are selected. Therefore, it is of great importance that the associations of putative genes and their variants are investigated across different populations for validation. However, the reports regarding the associations of these two MTHFR polymorphisms with the risk of RCCs are still awaited from other parts of the world.
The present study is the first attempt to investigate whether the MTHFR 677C/T and MTHFR 1298A/C polymorphisms can serve as the susceptibility and/or prognostic markers for RCCs in a Pakistani population. Further, genotype combination analysis and haplotype analysis were performed for an assessment of the combined effect of these two polymorphisms on the risk and prognosis of RCC in our population.
Materials and Methods
Subjects
This case-control study included 346 participants, with 168 patients and 178 controls. The RCC patients had undergone an operation for tumor resection at the Sindh Institute of Urology and Transplantation (SIUT) between March 2009 and November 2010. The controls had no clinical history of RCC as ascertained from their medical records.
Sample collection and tumor classification
About 5-8 mL blood samples were collected with informed consent from the participants by venipuncture and stored at 4°C in the vacutainers containing either ethylenediaminetetraacetic acid or anticoagulant citrate dextrose (ACD). The project was approved by the institutional ethical review committee.
The tumor specimens were classified on the basis of histology and graded according to the World Health Organization recommendations. The tumor node metastasis (TNM) staging recommended by the Union International Contre le Cancer and the Robson staging were carried out. The histological results were confirmed by a second blind evaluation.
DNA extraction and genotyping
The standard phenol-chloroform method (Sambrook and Russell, 2001) was used for DNA extraction. The MTHFR 677C/T polymorphism was genotyped according to a modification of the method of Frosst et al. (1995). Briefly, the target fragment was amplified in a total reaction volume of 25 μL containing 65 ng of the genomic DNA, 0.35 μM of the forward (5′-TGAAGGAGAAGGTGTCTGCGGGA-3′) and the reverse (5′-AGGACGGTGCGGTGAGAGTG-3′) primers, 1× PCR buffer II (Applied Biosystems Inc.), 2.5 mM Mg++, 200 μM dNTPs, and 1.0 U Taq polymerase. The thermal cycling conditions were a 5-min initial denaturation at 94°C, followed by 35 cycles of 94°C for 1 min, 63°C for 1 min, 72°C for 1 min, and the final extension at 72°C for 10 min. Twenty microliters of the amplified products were digested overnight with 10 U of HinfI enzyme (Fermentas, Life Sciences) in 2.0 μL of the recommended buffer at 37°C. The digested products were run on 10% polyacrylamide gel, stained with ethidium bromide, and visualized under the UV light. The genotypes were distinguished on the basis of two major bands: a 198 bp band for the C-allele and a 175 bp band for the T-allele. The homozygous C (CC) and homozygous T (TT) genotypes were represented by 198 and 175 bp bands, respectively; whereas, the heterozygous CT genotype showed both the 198 and 175 bp bands.
The MTHFR 1298A/C polymorphism was genotyped according to the protocol adapted from Weisberg et al. (1998). The DNA fragment was amplified with the forward (5′-CTTTGGGGAGCTGAAGGACTACTA-3′) and the reverse (5′-CACTTTGTGACCATTCCGGTTTG-3′) primers using the same PCR and thermal cycling conditions as described previously. Subsequently, 20 μL of the amplified products were digested overnight at 37°C with 2.5 U of the MboII enzyme (Fermentas, Life Sciences) in 2.0 μL of the recommended buffer. The digested products were run on 10% polyacrylamide gels, stained with ethidium bromide, and visualized under UV light. The genotypes were differentiated from each other on the basis of the two major bands that were an 84 bp band for the C-allele and a 56 bp band for the A-allele. Thus, homozygous C (CC) and homozygous A (AA) genotypes were represented by 84 and 56 bp bands, respectively. The heterozygous AC genotype showed both the 84 and 56 bp bands.
Statistical analysis
The demographic, clinical, and laboratory data were entered, coded, and processed using STATA 11® software. Departures from Hardy-Weinberg equilibrium (DA) and associations between the categorical variables were determined by the Pearson χ2 goodness-of-fit test. When Hardy-Weinberg equilibrium did not hold, Cochran-Armitage trend test was used to assess the association between the polymorphisms and the risk of RCCs. A semiparametric method that was based on the expectation-maximization (EM) algorithm was used for the maximum likelihood estimation of the haplotype frequencies (Marchenko et al., 2008). The correlation coefficient (r2) and likelihood ratio test were used for the calculation and assessment of linkage disequilibrium between the two loci. Odds ratios (ORs) with 95% confidence intervals (CIs) were used in order to measure the allelic, genotypic, and haplotypic risks for RCC. The p-values<0.05 were considered to be significant for all the analyses.
Results
The characteristics of the participants were analyzed. In summary, the mean age of cases was 64+12 years whereas the mean age of controls was 46+6 years, and the male-to-female ratio was 2.7:1 and 2:1 in the cases and the controls, respectively.
Nonsignificant allelic and genotypic associations of the MTHFR 677C/T polymorphism with the RCCs
Figure 1 is a representative gel for the distinction between C and T alleles of the MTHFR 677C/T polymorphism. Table 1 lists the genotypic and allelic frequencies for the polymorphism and the results of the statistical analyses for an association with the RCC risk. The genotypes (CC, CT, and TT) were in Hardy-Weinberg equilibrium for both the cases (χ2=0.406; DA=−0.0074; p-value=0.52) and the controls (χ2=0.088; DA=0.0032; p-value=0.77).
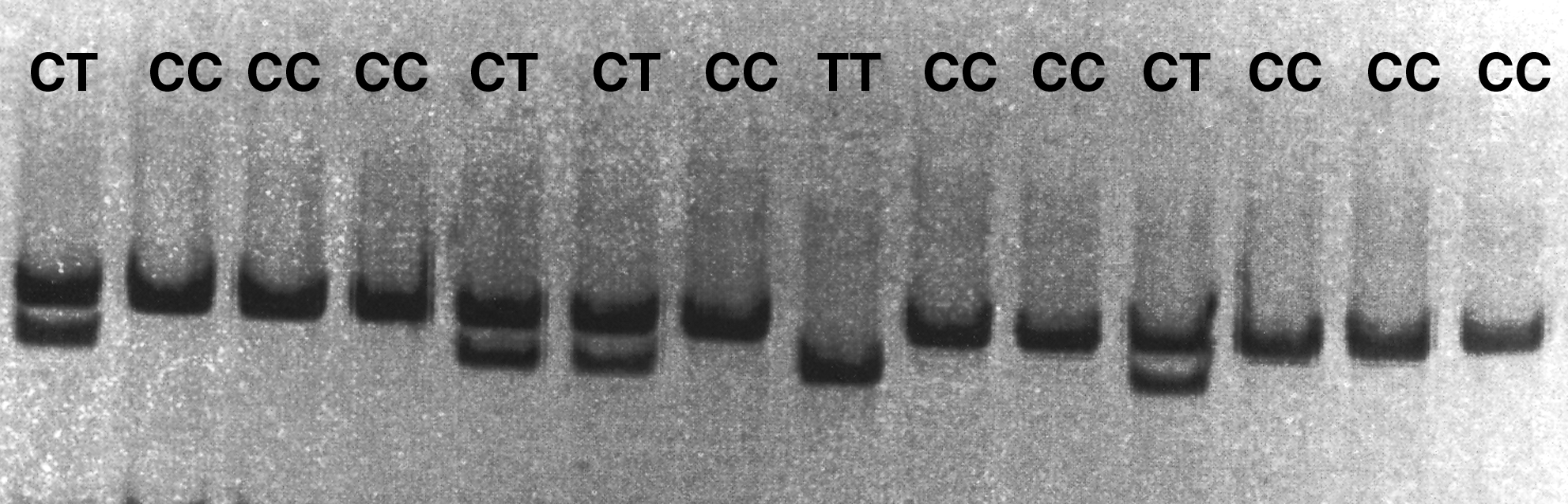
MTHFR 677C/T genotyping on 10% polyacrylamide gel after digestion with 10 U of HinfI restriction enzyme. MTHFR, methylene tetrahydrofolate reductase.
Chi-square test and ORs (95% CI) for the risk of RCCs.
No results were obtained for seven samples (one from control and six from case group).
MTHFR, methylene tetrahydrofolate reductase; RCC, renal cell carcinoma; ORs, odds ratios; CI, confidence interval.
The tests for association, that is, both the χ2 test and the OR, revealed that neither the genotypes nor the alleles for this polymorphism were significantly associated with the risk of RCC (Table 1).
Significant allelic and genotypic associations of the MTHFR 1298A/C polymorphism with RCCs
Figure 2 presents a gel image for the distinction of A allele from C allele in case of the MTHFR 1298A/C polymorphism. The genotypic and the allelic frequencies for this polymorphism are given in table 2.
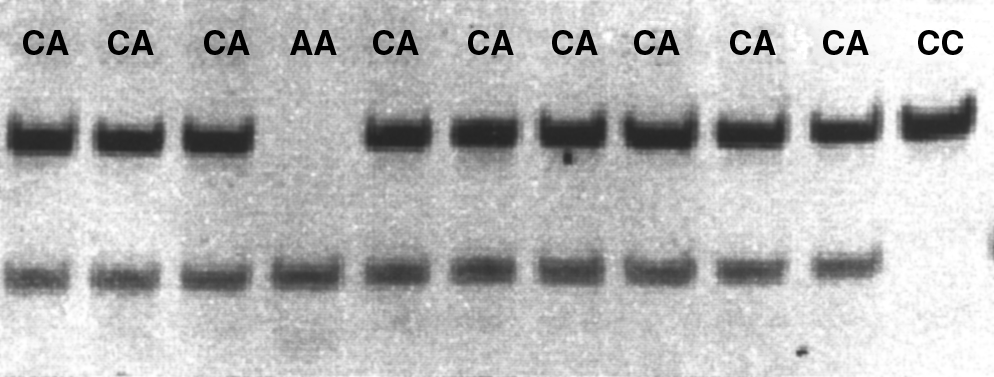
MTHFR 1298A/C genotyping on 10% polyacrylamide gel after digestion with 2.5 U of MboII restriction enzyme.
Chi-square test and ORs (95% CI) for the risk of RCCs.
No results were obtained for six control samples.
Statistically significant result.
The genotypes (AA, AC, and CC) were not in Hardy-Weinberg equilibrium for both the cases (χ2=13.95; DA=−0.071; p-value=0.002) and the controls (χ2=19.72; DA=−0.077; p-value<0.00001). Although it has been suggested that the allelic associations with a phenotype are not valid when Hardy-Weinberg equilibrium is violated (Sasieni, 1997; Song et al., 2005; Balding, 2006), the recent guidelines (Little et al., 2009) recommend that the allelic associations may be acceptable provided a plausible explanation for the deviation is given. It is a well-established fact that the conditions underlying Hardy-Weinberg equilibrium are rarely met in populations that consist of multiple ethnic groups with a documented history of consanguinity such as the population in this study (65.5% consanguinity) (Khan et al., 2011). Tests for association revealed that the C-allele of the MTHFR 1298A/C polymorphism was significantly correlated with the risk of RCC (χ2=6.11; p-value=0.01) having an OR of 1.60 (95% CI=1.1-2.34) (Table 2).
In case of the genotypes, homozygous C (CC) was found to be highly associated with the risk of RCC (χ2=6.75; p-value=0.0001) having an OR of 3.26 (95% CI=1.27-8.37) (Table 2).
Additionally, the results of the Cochran-Armitage trend test, which does not rely on the assumption of Hardy-Weinberg equilibrium, confirmed the above-mentioned associations (Table 2).
Significant associations of the unique combinations of MTHFR 677C/T and MTHFR 1298A/C genotypes with the risk of RCCs
The genotypes of two polymorphisms yielded nine possible combinations (Table 3). Analysis was done for each combination for an association with the risk of RCCs. As shown in table 3, the homozygous C genotype for MTHFR 677C/T in combination with the homozygous C genotype for MTHFR 1298A/C, that is, 677CC+1298CC, greatly increased the risk of RCC when compared with the reference combination of the wild-type genotypes 677CC+1298AA, having an OR of 8.34 (95% CI=2.7-25.7). The two other combinations that were highly associated with an increased risk of RCC were 677CT+1298AA and 677CC+1298CA with an OR of 3.21 (95% CI=1.3-7.8) and 2.45 (95% CI=1.3-4.6), respectively.
Statistically significant.
NA, not applicable.
Interestingly, despite the observation of Hardy-Weinberg disequilibrium at one locus, this pattern of association was also reflected in the semiparametric haplotype analysis based on an EM algorithm for the estimation of haplotype frequencies (Table 4). As shown in table 4, the 677C*1298C and 677T*1298A haplotypes demonstrated significant risks for RCCs with an OR of 2.21 (95% CI=1.5-3.2) and 2.7 (95% CI=1.5-4.8), respectively.
OR calculated using the logistic regression model.
Statistically significant result.
Nonsignificant associations of the MTHFR 677C/T and MTHFR 1298A/C polymorphisms with the prognosis of RCCs
The two main histological categories of the RCCs were the clear cell RCCs (67.1%) and the papillary RCCs (18.6%). The overall statistical analyses revealed no significant associations of the MTHFR polymorphisms, either separately or in combination, with the prognostic markers of RCCs such as tumor size, grade, and stage (data not shown).
Discussion
The present study reports specific associations between the polymorphisms in the MTHFR gene and the risk of RCCs. When the two polymorphisms were evaluated separately, a significant correlation was observed between the MTHFR 1298A/C polymorphism and susceptibility to RCCs. To the best of our knowledge, this is the first study showing that the MTHFR 1298A/C polymorphism is an independent risk marker of the epithelial renal cancers that include the clear cell, papillary, and chromophobe RCCs. A recent study from Iran that was based on male subjects only has reported the independent associations of this marker and the MTHFR 677C/T polymorphism with the increased susceptibility to clear cell RCCs (Safarinejad et al., 2011). On the other hand, a study published from the central Europe reported no association of the MTHFR 1298A/C polymorphism with the risk of renal cancers; however, the T-carrier genotypes for the MTHFR 677C/T polymorphism increased the risk of RCCs (Moore et al., 2008). In the present study, the MTHFR 677C/T polymorphism could not be established as an independent risk marker of the RCCs. These differences in the associations of the MTHFR polymorphisms with the risk of RCCs are similar to the variations in reports regarding the correlations between these polymorphisms and other cancers such as acute lymphoblastic leukemias (ALL), gastric cancers, and colorectal cancers (Skibola et al., 1999; Curtin et al., 2004; Alcasabas et al., 2008; Boccia et al., 2008; Zanrosso et al., 2009; Koppen et al., 2010). These observations highlight the importance of conducting specifically designed association studies in the different populations across the world so that the universal or population-specific patterns in the genetic risks can be distinguished.
The differences in the prevalence of the MTHFR polymorphisms have been observed in various ethnic groups across the world. In the case of MTHFR 677C/T polymorphism, a wide range of differences have been reported in the T-allele frequencies with the highest in the Mexicans (57%) and the lowest in the American blacks (12.6%; Wilcken et al., 2003). In this study, the T-allele frequency in the controls (18%) was in agreement with an inferred frequency from an earlier study conducted in Pakistan that investigated the MTHFR polymorphisms in glaucoma (Micheal et al., 2009). It was also within the frequency range, that is, 17.6%-42.4%, which has been reported for Asia (Botto and Yang, 2000). On the other hand, the C-allele frequency of the MTHFR 1298A/C polymorphism in the controls was much higher (35%) when compared with the frequencies that have been reported earlier for Asians (11%-17%) (Zintzaras, 2006). Interestingly, in a recent report from India (Chandy et al., 2010), the frequency of this allele was 43%.
In the present study, in both the patients and the controls, the MTHFR 677C/T genotypes were in Hardy-Weinberg equilibrium whereas the MTHFR 1298A/C genotypes were not. Although these results are in agreement with the above-mentioned study from Pakistan (Micheal et al., 2009), they have incorrectly reported that the MTHFR 1298A/C genotypes were in Hardy-Weinberg equilibrium, since based on their own data (overall controls: χ2=18.43; p-value<0.001, Pathan controls: χ2=5.25; p-value<0.01, and Punjabi controls: χ2=18.8; p-value<0.001). It is clear that these are not in Hardy-Weinberg equilibrium as seen in our study.
Another important observation reported for the first time in the present study is the association of the unique genotype combinations of the MTHFR polymorphisms with RCC risk. The synergistic effect of heterozygosity, that is, 677CT+1298AC, has been reported to elevate the risk of neural tube defects (van der Put et al., 1998). However, other studies have investigated such correlations with the ALL and the homocysteine levels and reported no significant associations (Skibola et al., 1999; Castro et al., 2003). In our study, significant OR as high as 8.34 (95% CI=2.7-25.7) was observed for the risk of RCCs when the two polymorphisms occurred in 677CC+1298CC combination. The finding that five individuals with 677TT+1298AC and four with 677CT+1298CC combinations is in agreement with an earlier observation that although T and C alleles are found predominantly in the trans-configuration, they may also exist in cis-configuration (Dekou et al., 2001). This supports a proposition, based on a study from North America, that most probably the two polymorphisms arose independently on the two separate chromosomal strands and that recombinations may occur, despite the small distance between these chromosomal loci (Hanson et al., 2001). However, double crossovers have not been observed as indicated by the absence of the homozygous combination 677TT+1298CC in our study as well as the earlier published work (van der Put et al., 1998; Rady et al., 1999; Dekou et al., 2001; Hanson et al., 2001; Castro et al., 2003; Chandy et al., 2010).
One study from Asia (Sakano et al., 2010) has reported that these MTHFR polymorphisms may serve as the gender-dependent prognostic markers for the clear cell RCCs. They reported that the MTHFR 1298A/C polymorphism was strongly associated with the severity of the disease in men, whereas the 677T*1298A haplotype was significantly associated with poor survival in women. The study from Iran (Safarinejad et al., 2011) has reported a strong correlation between the 677TT genotype and the tumor stage and grade in the clear cell RCCs in men. However, an overall analysis for the association of these polymorphisms with the clinical parameters of tumor size, grade, and stage did not reveal any significant trends in our study.
The corroboration between the analysis of genotype combinations and a semiparametric haplotype analysis supports the suggestion that the current widely used statistical models maybe considered robust enough to capture the subtle genetic trends in complex disorders, especially in the evolutionarily unique populations (Marchenko et al., 2008; Little et al., 2009).
In summary, the present study proposes that the combined genotypes of the MTHFR 677C/T and MTHFR 1298A/C polymorphisms may serve as strong predictive markers for the risk of RCC in the Pakistani populations. In addition, the MTHFR 1298A/C polymorphism is potentially an independent susceptibility marker for the risk of RCC. The observed patterns of associations of the MTHFR polymorphisms underscore the importance of conducting genetic investigations across different populations in achieving the goal of personalized medicine for cancer treatment. Further studies with larger sample size are needed from the South Asian region to confirm these observations and utilize the potential of these polymorphisms for the early diagnosis and prevention of RCCs.
Footnotes
Acknowledgments
This study was supported by core grant of the SIUT. The authors extend their special thanks to patients who participated in this study.
Disclosure Statement
No competing financial interests exist.