
Abstract
Genomic instability in colorectal cancer (CRC) occurs as either microsatellite instability (MSI) or chromosomal instability. The present study was aimed at examining the MSI for the MLH1 and MSH2 genes in normal colon and polyps, if detected. Four segments of the colon were sampled in 102 subjects during colonoscopy. DNA samples were analyzed for the MSI status according to the Bethesda consensus panel. Family history of any type of cancer or for colon cancer was present in 44.8% and 9.4% of the individuals, respectively. Forty-eight percent of individuals were microsatellite stable for all five markers at all locations, 20% had low MSI status (MSI-L), and 32% had high MSI status (MSI-H). The frequencies of MSI markers differed significantly from each other (p=0.003). The most frequent positive marker was D17S250. This is the first study which revealed that MSI is present in endoscopically normal-looking colon of normal individuals and, more frequently, in individuals with family histories of CRC. The detection of very early-stage CRC is possible by MSI analysis of DNA mismatch repair genes in colon tissues. This study has revealed crucial information for the use of molecular tests in CRC screening, such as high frequencies of MSI in endoscopically normal colon, which might cause false positivity.
Introduction
C
The long duration of carcinogenesis, which takes about a decade, allows screening of asymptomatic individuals for CRC. It has been estimated that more than 50% of mortality due to CRC could have been prevented through screening tests (Walsh and Terdiman, 2003). However, the optimum screening protocol for CRC has yet to be determined. Advances in technology have created a competition between new stool tests detecting early genetic mutations and endoscopic imaging techniques capable of demonstrating the early histological changes in colon mucosa. Though both stool tests and endoscopic screening have their pros and cons, endoscopic screening seems to be the most efficient one. Although screening by sigmoidoscopy or colonoscopy can detect and remove adenomatous polyps, thereby reducing cancer risk, endoscopic screening is also partially effective, particularly for proximal colon cancers (Søreide et al., 2009). However, to the best of the authors' knowledge, the frequency of mutations of MMR genes in “endoscopically normal colon” has not been previously determined. The present study searched for MSI according to the Bethesda consensus panel (BAT25, BAT26, D2S123, D5S346, and D17S250) in four segments of endoscopic normal colon, polyp, or cancer if detected and also in blood samples. Furthermore, the correlations between MSI and clinical parameters were studied.
Materials and Methods
Patient selection
The Human Research Ethics Committee of Abant Izzet Baysal University approved the study (# 2007/100-48). All patients gave informed consents on molecular testing. Consecutive patients scheduled to undergo diagnostic colonoscopy were screened for the study criteria. The exclusion criteria were age under 40 years, acute gastrointestinal bleeding, previous diagnosis of inflammatory bowel disease or CRC, previous colon surgery, and incomplete colonoscopy for technical reasons. The peripheral venous blood samples of 3 mL were collected into EDTA-coated tubes. All colonoscopies were performed by one gastroenterologist, using the conventional endoscopy system of PENTAX EC-3885L
Adequate genomic DNA extraction using QIAamp Tissue and Blood Mini Kit (Qiagen) amplification was possible in 102 out of 108 individuals. Mean age was 56.3±14.9 years (58.4±14.8 for men and 53.6±14.7 for women, p>0.05). Most of the participants were men, with a female: male ratio of 47:55 (0.85). Demographic features are shown in Table 1.
Some patients had more than one diagnosis, so the total percentage exceeds 100%.
IBD, inflammatory bowel diseases; CRC, colorectal cancer.
MSI analysis
The assessment of MSI was done on colon tissue and peripheral blood. The D2S123, D5S346, D17S250, BAT25, and BAT26 were utilized for the determination of MSI in CRC specimens (Boland et al., 1998). The technical features of the primers are presented in Table 2.
Tm, annealing temperature; bp, base pair.
The amplification of the polymorphic markers was carried out by the polymerase chain reaction (PCR) in a 25-μL reaction volume (Promega) (Takara). PCR involved an initial denaturation at 95°C for 3 min, followed by 35 cycles of denaturation at 95°C for 30 s, annealing at 57°C-59°C for 30 s, and extension at 72°C for 30 s, with a final extension at 72°C for 4 min. PCR products were diluted 1.5:1 with a 95% formamide gel loading buffer. After denaturation at 95°C for 3 min, 7 μL of each sample were size fractionated by electrophoresis through a 6% polyacrylamide gel with 8.3 M urea by 1650 volt current for 3-5 h. Silver nitrate staining was applied to gels after electrophoresis, and they were photographed under white light.
The allelic patterns obtained from the colon and blood samples were compared with each other in order to confirm that the molecular alterations were specific to the colon tissue (Fig. 1).
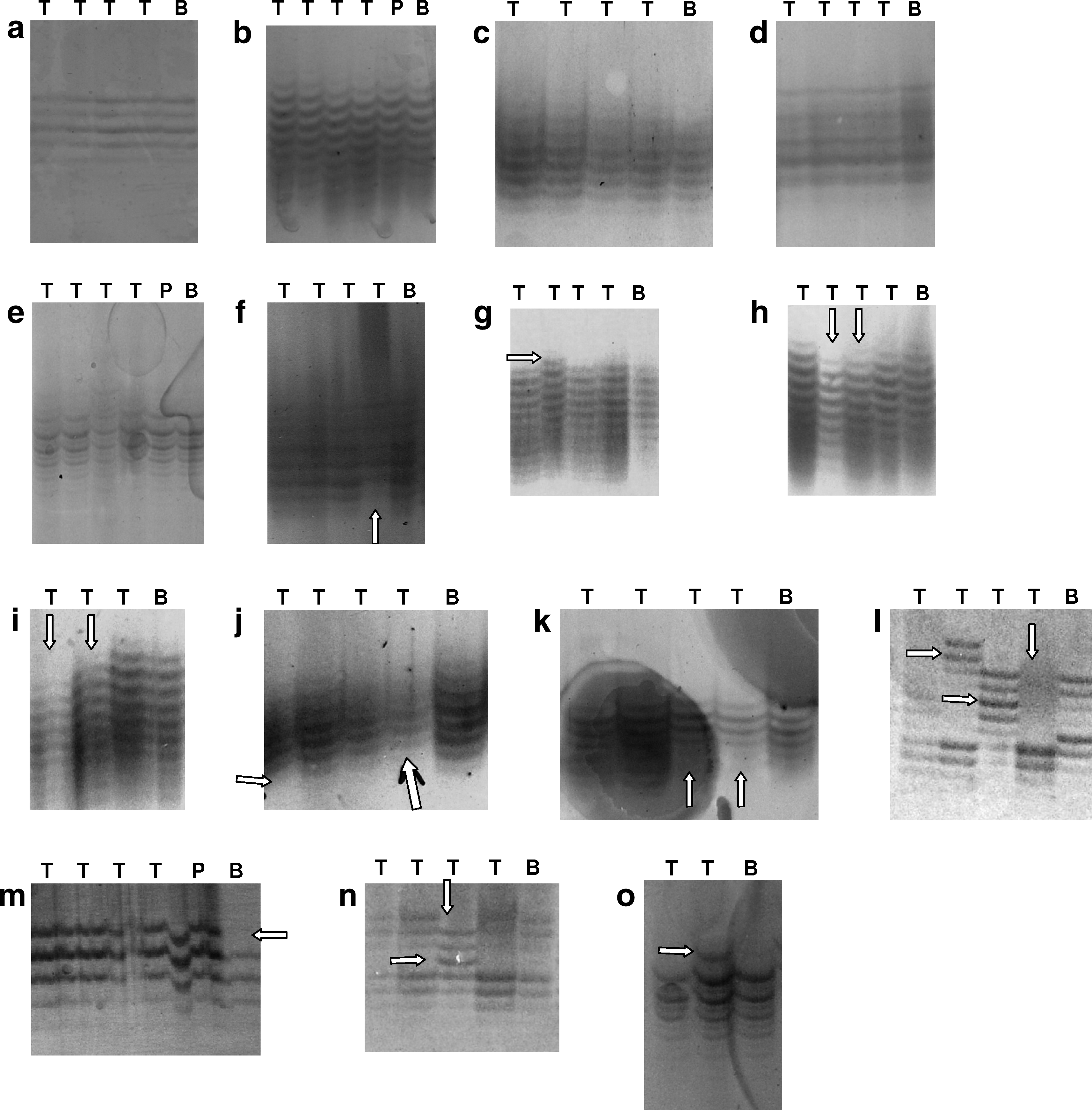
Microsatellite status in eight patients' colon tissues, polyps, and blood samples
MSI interpretation
Cases with no evidence of instability for any marker throughout the entire colon are considered microsatellite stable (MSS). The MSI is, by definition, classified as MSI-L if one marker at one region was positive and as MSI-H if more than one marker or regions of the colon was positive (Boland et al., 1998).
Statistical analysis
Statistical analysis was undertaken using SPSS 16.0 software package. The Friedman test was used to determine the frequency distribution, to compare the means of two groups, and to compare more than two parameters. The Wilcoxon-W test was used to compare two parameters within a group, and the Mann-Whitney U was used to compare two parameters between two groups. p<0.05 was considered significant.
Results
Microsatellite status
Out of 102 individuals, 52 (51%) were MSS for all five markers in all four regions of the colon, whereas the frequency of MSI-L and MSI-H were 19 (19%) and 31 (30%), respectively. Mean ages of individuals with MSS and of MSI were comparable (58.7±15.2 and 53.9±14.4 years, respectively; p=0.111). The presence of microsatellite alterations was not related to a family history of cancer (p=0.188) or CRC (p=0.208). Similarly, microsatellite status was not related to a family history of cancer or CRC either (p=0.632 and p=0.069, respectively). Both presence and status of microsatellite alterations were also independent of smoking (p=0.580 and p=0.362, respectively).
Microsatellite status was stable in most of the women, whereas half of the men had MSI-H (p=0.000) (Fig. 2). This variation in the microsatellite status of genders was independent of smoking (p=0.855), family history of cancer (p=0.135), or family history of CRC (p=0.742).
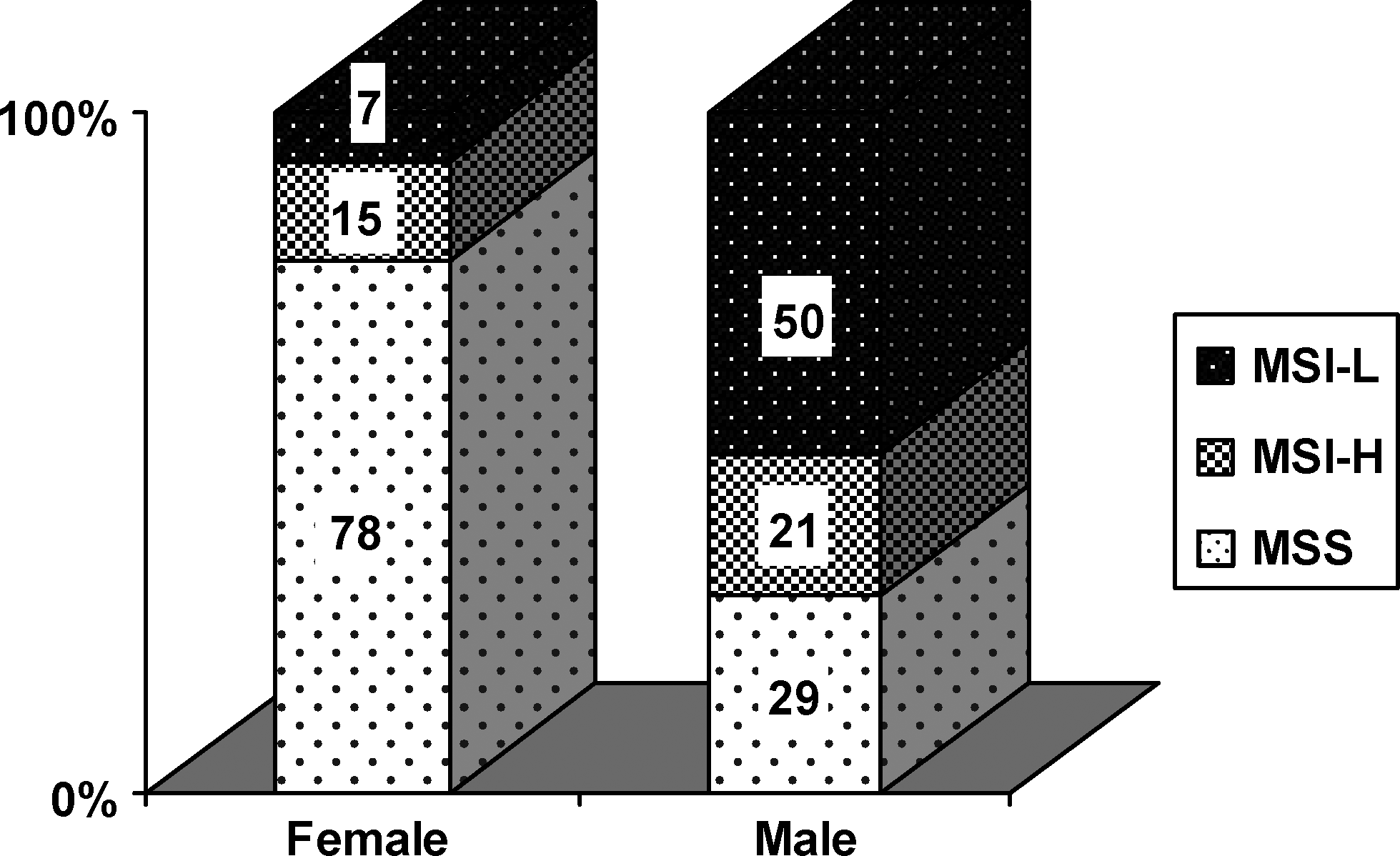
Microsatellite status with regard to gender. MSI-L, low MSI status; MSI-H, high MSI status; MSS, microsatellite stable.
MSI markers
The distribution of positive primers among 19 individuals with MSI-L was D17S250 in 8 cases, BAT25 and D5S346 in 4 cases, D2S123 in 2 cases, and BAT26 in 1 case. The regions for MSI-L were more frequently located at the proximal colon; AC (10 cases), TC (2 cases), DSC (5 cases), and the rectum (2 cases).
Among 31 individuals with MSI-H, one primer was positive in more than one region of the colon in 18 (58%) individuals, and two primers and three primers positivity was detected in 12 (39%) and 1 (3%) individuals, respectively (Table 3). D17S250 was the most frequent positive primer, and unlike the other primers, it was usually positive in more than one region of the colon.
The molecular alterations were sequentially shown in four regions of the colon; namely ascending colon, transverse colon, descending-sigmoid colon and rectum. “−” and “+” implies MSS and MSI, respectively.
No., the patients' identification number; F, female; M, male; CD, could not be done; MSS, microsatellite stable; MSI, microsatellite instability.
Polyp and cancer tissues
During colonoscopies, 5 patients with CRC and 26 patients with polyp were detected. The mean age of patients with polyp (62±13.4 years) was similar to that of patients with CRC (67±8.2 years, p=0.62). All the patients with CRC were men. On the other hand, half of the patients with polyp were women. Although all patients with CRC were MSS at endoscopic normal colon segments, 12 patients (62%) with polyp were MSI, and half of them had MSI-H. The molecular analyses could be done in seven polyps, but not in the cancer tissues. Out of seven, three polyps were MSS in polyp tissues, and the colon tissues had MSS (one), MSI-L (one), and MSI-H (one). The other four polyps were positive for each of different primers (D2S123, BAT25, D5S346, and D17S250). The colon tissues of these polyps were either MSS (two) or had MSI-H (two). All MSI-H were detected in the segments of the colon where polyps were localized. Among the remaining 19 patients whose polyp tissue could not be analyzed, endoscopic normal colon tissues in 12 (46%) patients were MSI (6 MSI-L and 6 MSI-H) (Table 4), usually in the same region with the polyp (1 MSI-L and 2 MSI-H).
The molecular alterations were shown sequentially from four regions of the colon; namely ascending colon, transverse colon, descending-sigmoid colon and rectum. “−” and “+” signifies MSS and MSI, respectively.
Distribution of MSI markers in the colon segments
The ratio of positivity for D17S250, BAT25, D5S346, BAT26, and D2S123 were 29.3%, 13.2%, 10.1%, 7.9%, and 6.4%, respectively, among the individuals who could be analyzed. The most frequent positive marker was D17S250 (p=0.003). The frequency of D17S250 was significantly higher than other markers in the AC (p=0.002) and TC (p=0.001), but not in the DSC (p=0.144) or rectum (p=0.151). Among the individuals who could be analyzed, MSI frequency was 41.9% in the AC, 25.0% in the TC, 28.0% in the DSC, and 24.1% in the rectum. Therefore, the AC was statistically the most common region of MSI (p=0.009). The ratio of positivity for each primer in different segments of the colon is shown in Figure 3. Although BAT26 was frequently detected in the rectum (31%), there was no statistically significant difference in the positivity of primers in the rectum (p=0.336).
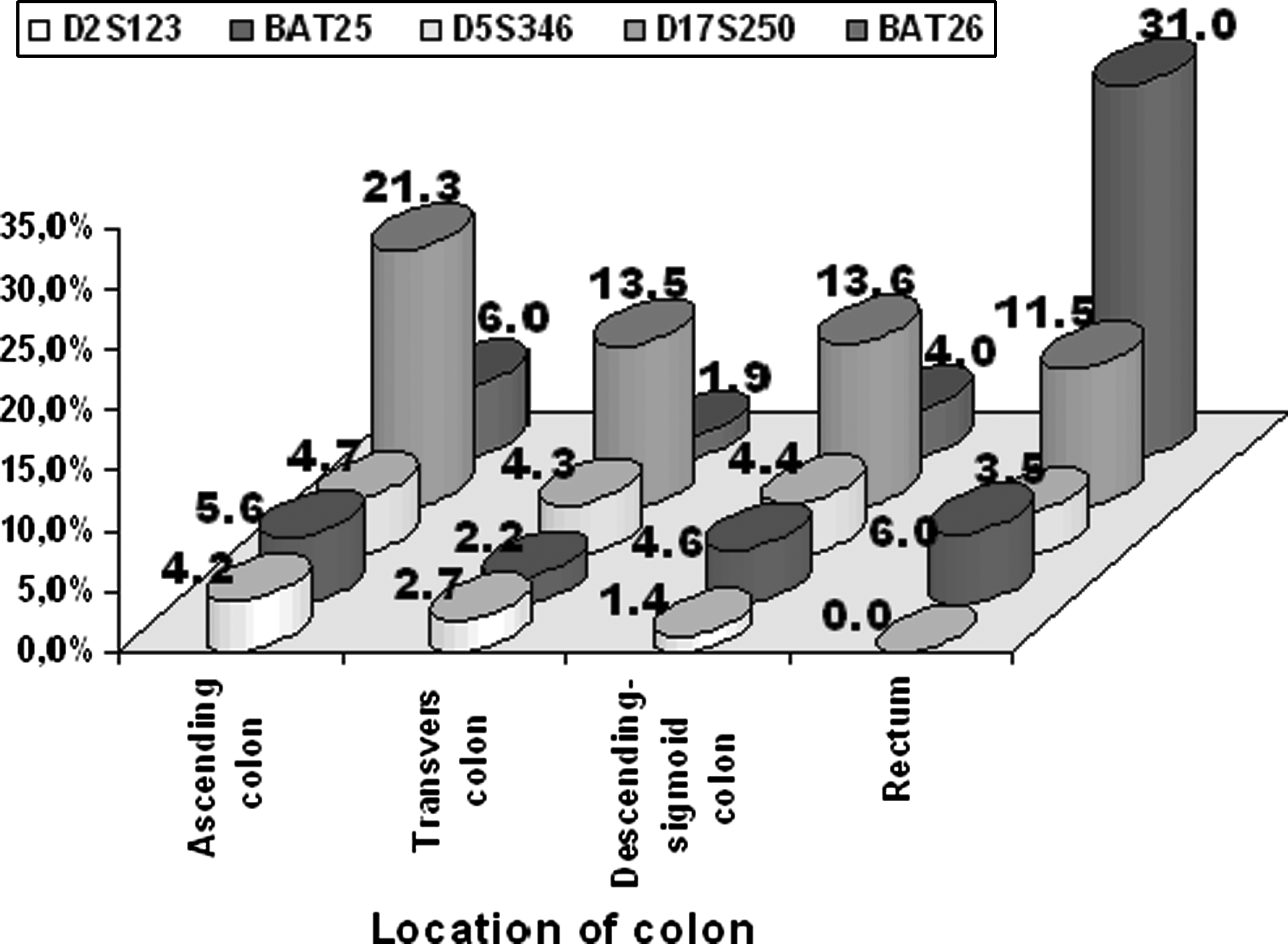
Ratio of each primer's positivity according to the segments of the colon.
Discussion
CRC is characterized by multiple chromosomal and epigenetic abnormalities. MSI is one of the molecular mechanisms leading to genomic instability (Ashktorab et al., 2005), and it is an important factor for early diagnosis, prognosis, and treatment of CRC. D17S250, D5S346, D2S123, BAT25, and BAT26 are called Bethesda markers and have been proposed for MSI analysis in CRC (Boland et al., 1998). This study searched the MSI by using Bethesda markers in four regions of endoscopic normal colon in 102 individuals. Half of the individuals had MSI, two-thirds of whom were MSI-H. D17S250 was the most frequently altered locus (p=0.003), mainly in the AC (p=0.002) and the TC (p=0.001).
MSI is caused by a failure of the MMR system in correcting errors of DNA replication that occur during normal regeneration of tissue (Lim et al., 2006). The repetitive sequences are designated as “microsatellites.” MSI is characterized by the presence of novel alleles in the DNA of cancer tissues that are absent in the matched microsatellite region of normal tissue (Thibodeau et al., 1993). Several malignancies can be detected by microsatellite analyses including renal cell carcinoma (Eisenberger et al., 1999), uterine cervical carcinoma (Rha et al., 2001), and squamous cell carcinoma of the head and neck (Spafford et al., 2001). The MSI status in CRC has notable biological significance, in terms of both prognosis and response to chemotherapy (Risio et al., 1996; Lim et al., 2004). Koshiji et al. (2002) performed fecal MSI analysis for detection of CRC. Traverso et al. (2002) showed that analysis of fecal BAT26 during colonoscopy was a practical method. The National Cancer Institute (NCI) established guidelines for the evaluation of MSI (Boland et al., 1998). The present study, by using NCI guidelines, revealed that MSI is an important phenomenon in CRC and can be frequently detected even in endoscopic normal colon tissues. Forty-nine percent of individuals depicted MSI in their colon, and two-third of them had MSI-H status. In other words, early detection of individuals with CRC might be possible by MSI analysis of MMR genes from different regions of normal colon tissue taken during colonoscopy. We believe that this can serve as a screening strategy for CRCs.
MSI is reflected as alterations in the patterns of polymorphic, short, tandem repeat segments (microsatellites) dispersed throughout the human genome (Arzimanoglou et al., 1998). MSI is a hallmark of DNA MMR deficiency that, in turn, appears to be primarily due to inherited and/or acquired/somatic alterations in the MMR genes, such as hMLH1 and hMSH2 (Dietmaier et al., 1997). Therefore, it is assumed that MSI reflects an underlying genomic instability resulting from inactivation of both alleles at a DNA repair gene locus (Lazar et al., 1994). Thus, the presence of MSI correlates with the absence of either hMLH1 or hMSH2 (Ashktorab et al., 2005). The familial cases inherited a single mutation in a DNA MMR gene and MSI develops after the loss of activity of the other allele at the same locus (Han et al., 1995). The nonfamilial CRC cases demonstrating MSI presumed to have somatic inactivation of both alleles of a single DNA MMR gene locus in target colon epithelium (Borrensen et al., 1995). It was reported that up to 86% of tumors in patients with HNPCC exhibit MSI (Aaltonen et al., 1993), whereas, 80%-85% of sporadic CRCs lack MSI (Ashktorab et al., 2005). The analyses of 77 Turkish patients with sporadic CRC showed that 39% had loss of MLH1 expression, and 7% had loss of MSH2 expression (Erdamar et al., 2007). Tunca et al. (2010) reported that MSH2 is a founder mutation in Turkish HNPCC patients and was identified in 5 of 28 (18%) families but not in the control group. In our study, both MSI-H and MSI-L states in normal colon were independent from family histories of cancer (p=0.188) or CRC (p=0.208) or smoking (p=0.580).
Breivik et al. (1997) indicated that MSI in CRC was related to gender and age. MSI was found to be more frequent among younger male and older female patients. Ashktorab et al. (2005) argued that being a woman might influence the pathway of CRC development. They showed that the odds ratio for female patients having MSI-H was 11.7 times higher than male patients among African Americans, although the reason for this gender difference was unknown. Estrogen plus progestin preparations were associated with a decreased risk of CRC. In women with MSI-L or MSS tumors, there was a 40% reduction in CRC risk, whereas there was no clear association with MSI-H tumors (Newcomb et al., 2007). We found that the presence of MSI was related to male gender, but not to age (p=0.111). MSI-H was detected in 50% of the men and 7% of the women, a 7.14-fold difference in favor of men. Additionally, this male predominance in MSI-H status was independent of family histories of cancer or CRC and smoking (p=0.000).
Colon cancers associated with HNPCC are more often right-sided, and constitute 47.8% of all cancers and 74.6% of CRCs (Luo et al., 2005; Jeon et al., 2008). A Swedish national investigation in 2001 showed that 51% of all CRC was located in the proximal colon (Hemminki and Li, 2001). Kazama et al. (2005) and Lim et al. (2006) showed that positive MSI status has been associated with proximal location of the lesion (polyp or tumor) in the colon. Consistent with this, MSI was significantly associated with proximal colon location in our study. The frequencies of MSI in the AC, TC, DSC, and the rectum were 41.9%, 25.0%, 28.0%, and 24.1%, respectively. So, the AC and the TC were statistically the most frequent regions (p=0.002 and p=0.001, respectively), in agreement with Fitzgibbons et al. (1987) and Hemminki and Li (2001). This proximal predominance of MSI together with CRC lends support to the recommendation to use total colonoscopy rather than sigmoidoscopy for CRC screening.
Microsatellites have been widely considered as an ideal genetic marker for MSI indicating the loss of function of MMR genes (Luo et al., 2005). The diagnosis of MSI in CRC is based on the molecular analysis of five microsatellite markers, including two mononucleotide repeats (BAT-25 and BAT-26) and three dinucleotide repeats (D2S123, D5S346, and D17S250) (Boland et al., 1998). However, it has been argued that the analysis of a single mononucleotide repeat such as BAT-26 (De la Chapelle, 1999; Lim et al., 2006) may be sufficient for this purpose. The comparison of the five microsatellites in HNPCC patients highlighted the high informativeness of mononucleotide repeats (BAT-25 and BAT-26) for MSI analysis (Salto-Tellez et al., 2005). The present study revealed a different frequency pattern for markers. Since D17S250 was the most common marker, we concluded that D17S250 is the most informative marker. The high rate of MSI-H among individuals with normal colonoscopy also implied that all five markers are important and should be used for early diagnosis of CRC, contrary to De la Chapelle's argument (1999).
The German HNPCC Consortium (2006) suggested that screening for MMR deficiency should not be applied routinely in adenomas with the goal to identify HNPCC patients. MMR-proficient adenomas can also be found, although the mutator pathway is detectable in adenomas in most HNPCC patients. The analyses of MSI status in 18 adenomas from 17 HNPCC patients were detected in 83% MSI-H and 6% MSI-L (Giuffrè et al., 2005). This is the first time that the MSI status of nearby normal colon tissue to polyp has not been analyzed. Although a small number of polyps could be analyzed in this study, MSI was present in 57% of the polyps and 50% of their normal colon, which was usually in the same region of colon with polyp. Therefore we thought that the presence of polyp is a marker of MSI at nearby normal colon tissue.
The present study is the first one revealing the high frequency of MSI in endoscopically normal colon, especially in the proximal segments. The identification MSI appears to be important for early detection of individuals with CRC risk. We believe that data acquired in this study will contribute to defining the country profile of CRC by early identification of genetically predisposed individuals and the risk groups with acquired genetic disorders. We believe that a multi-center study including larger number of individuals from different nationalities should be conducted in order to determine the role of MSI in CRC pathogenesis and also to be able to interpret the results of molecular analysis used as a screening test for CRC.
Footnotes
Acknowledgments
The authors thank the patients for participation in this research, Dilek Dogruer for excellent technical assistance and Hatip Aydin for statistical analysis. In addition, this work was supported by the Abant Izzet Baysal University Fund with project number BAP-2008.08.03.272.
Disclosure Statement
All authors have no conflict of interest or financial interest in this work.