
Abstract
Genetic diseases and congenital anomalies are the second most common cause of infant mortality in Brazil. In 2009, the Ministry of Health established the National Policy for Integral Attention in Clinical Genetics in the Brazilian Unified National Health System (UNHS). This policy is not yet regulated, and there is a fear that, in the name of the comprehensiveness of health care, genetic testing might be carried out without due care and criteria, increasing costs to the UNHS. Currently, only a small population has access to genetic testing, through teaching hospitals or private health care. The biggest challenge in Brazil, in this area, is to be able to set the right standards and assessment processes about clinical utility, testing priorities, dispersal of resources, and distribution of skilled professionals. Expanding access to users of the Brazilian UNHS will mean mining the technical, social, and ethical aspects about medical genetics services.
Introduction
G
Brazil: Population, History, and Demographics
The Federative Republic of Brazil is the fifth largest country in the world, in terms of geographical area, occupying a territory of approximately 8.5 million km2, bordering with every other South-American country, except for Chile and Ecuador (www.ibge.gov.br; 10/02/11).
The Brazilian population (about 190 million) is the result of the miscegenation between Amerindians, Europeans, Africans, and Asians. The autochthonous Amerindians were approximately 2.5 million individuals when European colonization began, with the arrival of about 500,000 Portuguese, almost all men, between 1500 and 1808 (Pimenta et al., 2006). The slave trade began in the mid-sixteenth century: until 1855, about 4 million Africans, mostly from regions that today are Angola, Congo, and Mozambique, were brought to Brazil (IBGE, 2007). The Brazilian population initially originated mainly from the initial mix between European men and Amerindian or African women. Finally, about 6 million immigrants arrived in Brazil between 1820 and 1975, mostly Portuguese and Italians (70%), and (in smaller number) Germans, Spaniards, Syrians, Lebanese, and Japanese (IBGE, 2007).
According to the latest census (2010), the country has 190,755,799 inhabitants, unevenly distributed in five main geographic regions (North, Northeast, Midwest, Southeast, and South) (Fig. 1), encompassing 26 states, 1 Federal District, and 5,565 municipalities. The national demographic density is 22.43 inhabitants/km2, ranging from 2.01 inhabitants/km2 in Roraima (North) to 444.07 in the Federal District (Midwest) and 365.23 in the Rio de Janeiro State (Southeast). In the last decade, the average growth rate of the population was 1.17% per year, with 84.4% corresponding to urban populations: In states such as Rio de Janeiro and São Paulo, the urban population reaches more than 95%. A megalopolis such as the city of São Paulo, with 11.253,503 inhabitants, is in contrast with small hidden villages, located mainly in the north, some reached only through precarious trails, or by plane or boat (www.ibge.gov.br; 10/02/11).
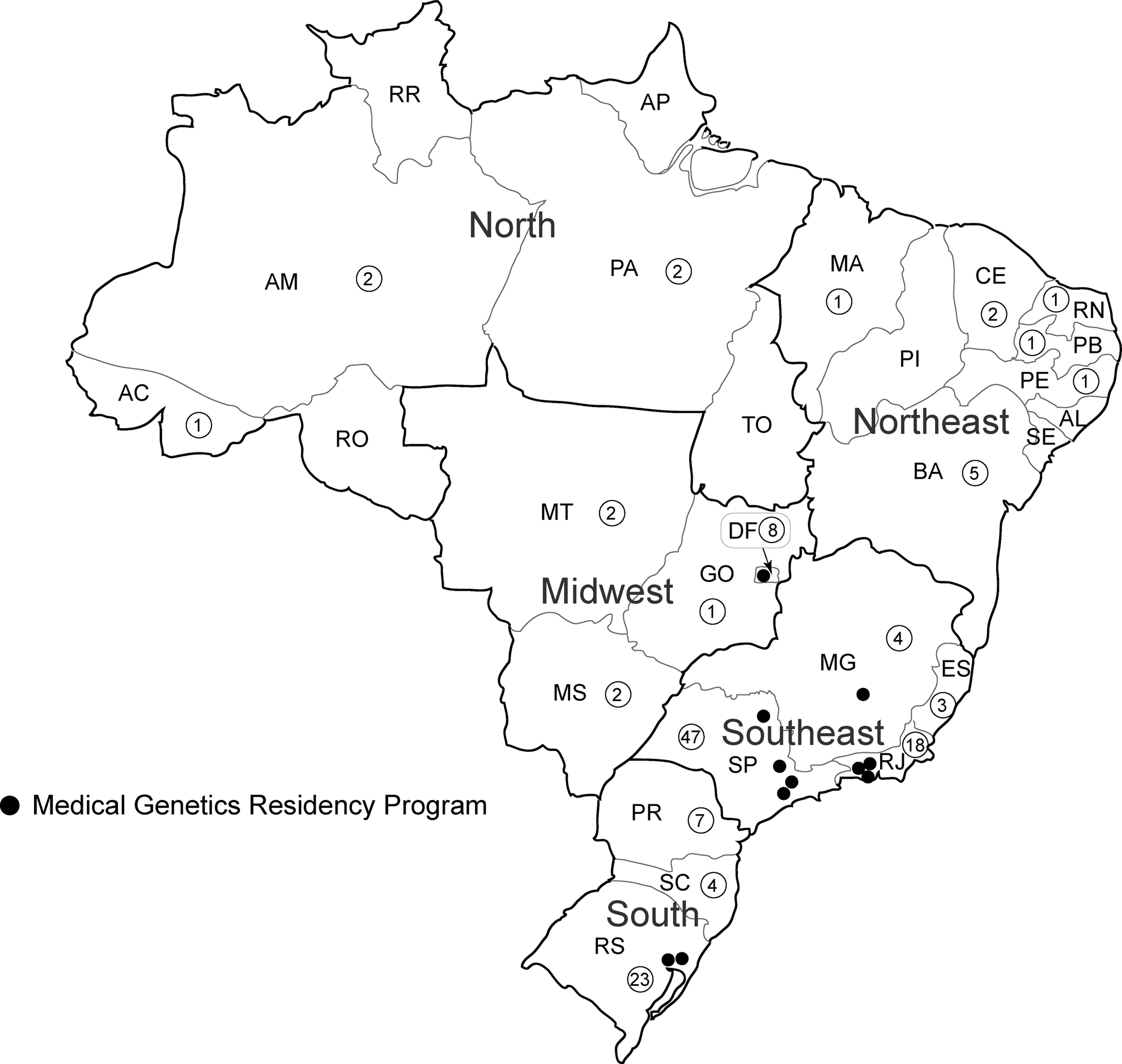
Map of Brazil with the distribution of the medical genetics specialists, members of the Brazilian Society of Medical Genetics (numbers inside the circles), and the Medical Genetics Residency Programs, by state.
In 2010, the male:female ratio was 0.96; 51% of the population was below the age of 30 years, but the proportion of people more than 35 years has been increasing, narrowing the base of the age group pyramid (www.ibge.gov.br; 10/02/11). In 2009, the life expectancy at birth was 72.9 years, and the fertility rate was 1.94. Illiteracy among people aged 15 years or older dropped (from 13.3%, in 1999, to 9.7%, in 2009), and infant mortality decreased considerably (from 47‰, in 1990, to 19.88‰, in 2010). Progress is observed in other indicators as well, such as a population with access to drinking water (93.5%), sewage (68.3%), and adequate garbage collection (98.5%) (IBGE, 2010).
In 2009, 48.2% of the people considered themselves white; 44.2%, pardos (mixed); 6.9%, black; and 0.7%, Native Indians or Asians. This distribution is uneven, as in the South, the white population reaches 78.5%; inversely, most pardos or mixed color people are found in the North (71.2%) and the Northeast (62.7%) (IBGE, 2010).
From 1964 to 1985, the country suffered military dictatorships; but, currently, after six consecutive free elections, the nation is emerging as a consolidated democracy and a political and economic region leader. It possesses a magnificent biodiversity and ample natural resources, including a large and well-developed agriculture in several regions, mining, manufacturing, and services. A competitive and diversified industrial production has been developing. However, the country still faces huge economic, political, and social problems, the paramount example being the highly unequal income distribution. Social and economic differences are evident, and the Southeast and South have the best human development index (HDI), while the Northeast is in the worst position. In 2008, the HDI of the São Paulo State was 0.833, whereas that of Alagoas was 0.667 (www.pnud.org.br/home/; 10/02/11).
The Brazilian Unified National Health System
The Brazilian Unified National Health System (UNHS) was established by the Constitution of 1988, so that the whole population would have access to health care. Earlier, public health care was restricted to employees who contributed to the national social security; those without jobs were assisted by philanthropic institutions, in most instances linked to the Catholic Church. The Brazilian UNHS had its ideological principles laid down in the Organic Law of Health of 1990—universality, comprehensiveness, and equity, together with four organizing principles—hierarchy, decentralization, regionalization, and popular participation (Paim et al., 2011).
Universality ensures that all people, regardless of ethnic background, gender, creed, occupation, social class, or place of residence, are entitled to health care. Comprehensiveness means ensuring the provision of cohesive and continuous actions, both preventive and curative, at the individual and collective planes, required in every situation for all levels of care. Equity is a principle of social justice that aims at reducing inequalities, investing more where the needs are larger (Paim, 2009).
The UNHS is a hierarchical system of several interconnected units, each with its assignments: (1) at the first level are the basic health units or the family health units, which everyone can directly access; (2) then, there are more complex services, such as polyclinics and hospitals, to where, whenever necessary, people will be referred from the basic health units or family health units; (3) in case of emergency or urgency, people will seek the nearest emergency room (Paim, 2009).
The UNHS is ruled by federal, state, and municipal governments; over time, municipalities should assume an increasingly important role in the provision and management of health services, conducting the negotiations with suppliers and promoting health policies. Smaller municipalities, however, suffer from the lack of human, financial, and material resources, and the population is insufficient for maintaining a hospital or more complex specialist services; thus, the decentralization of services also implies regionalization. In a huge country such as Brazil, it is necessary to organize the services carefully to provide access to all types of care, while avoiding redundancy and waste (Paim, 2009).
As a part of ensuring the effectiveness of public health policies, and as a means of exercising social control, channels were created for popular participation in the management of the UNHS, at all levels (municipal, state, and federal). Users participate in the management of the UNHS through the National Health Conference, which takes place every 4 years, and through the Local Health Councils, which are permanent collegial bodies. At the Local Health Councils parity is the rule, which is that users occupy half of the vacancies; the government, a fourth; and health workers, the other fourth (Paim, 2009).
The problems faced by all those who need to use the health services of the UNHS are many: queues, delay in getting a medical appointment, and scarcity of beds in public hospitals, mainly at Intensive Care Units. In spite of all these problems, encountered on a daily basis, we should not lose sight that the creation and implementation of the UNHS was and still is a great achievement toward citizenship with regard to the Brazilian population (Paim, 2009).
In addition to the UNHS, cooperatives and companies may also provide health care. Currently, about 20% of the Brazilian population also resort to some private health care (Pietrobon et al., 2008). This Supplementary Health System is regulated by the Ministry of Health, through the National Health Insurance Agency (ANS, Agência Nacional de Saúde Suplementar), which controls these health plans to assure public interest.
Evolution of Medical and Clinical Genetics in Brazil
There are no known estimates about the incidence and prevalence of heritable diseases in Brazil. It is estimated that 5% of live births have congenital anomalies, the cause of which is, at least partially, determined by genetic factors (Horovitz et al., 2005). At present, the country is facing an epidemiological transition, with a significant improvement of health indicators at the population level, as diseases caused by malnutrition, poor sanitary conditions, and external pathogens are being controlled. Heritable diseases and congenital anomalies are now responsible for an increasing proportion of childhood deaths (Marques-de-Faria et al., 2004; Horovitz et al., 2005;): The conditions presented in Chapter XVII of the International Classification of Diseases—congenital malformations, deformations, and chromosomal anomalies—are, since 2005, the second most common cause of infant mortality in all Brazilian regions (www.datasus.gov.br; 10/02/11).
In this context, heritable diseases arise as a public health problem and require special attention. In 2004, a Clinical Genetics Working Group was created, consisting of members of the Brazilian Society of Medical Genetics, members of the Brazilian Society of Genetics, and representatives of the Ministry of Health, to elaborate a proposal for the inclusion of genetics in UNHS. In January 2009, the Ministry of Health of Brazil introduced, through Ordinance No. 81, the National Policy for Integral Attention in Clinical Genetics in UNHS, the main goal of which is to structure a network of services, hierarchic and regionalized, to allow comprehensive care in clinical genetics, and to improve access to this specialized field by the general population (Ministério da Saúde, 2009a).
This policy was approved by the government and published in the Federal Official Gazette of Brazil, thus becoming effective immediately after its publication; nevertheless, as often happens, it left some relevant practical aspects for later additional legislative measures, which have not yet been published. Three major barriers are identified: (1) insufficient skilled human resources that actually provide this service to all the population; (2) lack of standardized criteria for the treatment of diseases for which it is available; and (3) fear that, in the name of comprehensiveness of health care, genetic testing could be carried out without clear criteria, significantly raising costs for the UNHS.
Clinical genetic services in Brazil began developing in the 1960s, almost always linked to Postgraduate Human and/or Medical Genetics courses, and to an increasing interest in the detection of certain genetic diseases or groups of diseases. These services were still mostly linked to hospitals and academic institutions of high complexity15. In 2004, a survey conducted by the Brazilian Society of Medical Genetics identified 64 genetic services: 37 (58%) in the Southeast (75.7% in the São Paulo State only), 17 (26%) in the South, 7 (11%) in the Northeast, and 3 (5%) in the Midwest. At the time, none was registered for the North region. The types of services offered were quite variable, some being very comprehensive (clinical care, laboratory, and research), while some provided only genetic counseling (Marques-de-Faria et al., 2004; Castilla and Luquetti, 2009).
At present, there are still no genetic services acting consistently with primary health, along with the basic health or family health units. In 1997, the number of procedures and professionals involved in genetic counseling in Brazil was insignificant. It was estimated that most patients and families suffering from a genetic disease were unaware of their medical condition and had not been adequately investigated to pinpoint the genetic risk factors involved (Brunoni, 1997; Brunoni, 2002).
Nevertheless, in August 2011, the Brazilian Society of Medical Genetics registered 135 genetics specialist members of its society: 121 (89.6%) physicians, 8 (6%) biologists, four (3%) biomedical professionals, one (0.7%) biochemist, and one (0.7%) psychologist. In addition to the small number of professionals, there is also a great disparity in their distribution, as 72 (53.3%) live in the Southeast, 34 (25.2%) in the South, 13 (9.6%) in the Midwest, 11 (8.2%) in the Northeast region, and only 5 (3.7%) in the North region (www.sbgm.org.br; 08/02/11) (Fig. 1). The geographical spread of genetics professionals and services relates to the population density and HDI, though in the more remote, poorer, and less densely populated areas (particularly in the North and Northeast), there is a greater shortage of professionals. Undoubtedly, the small number of medical genetics specialists serves as an obstacle for a generalized implementation of the National Policy for Integral Attention in Clinical Genetics in UNHS.
In 2009, a survey conducted by the Ministry of Health showed that there are other medical specialties which face recruitment difficulties due to lack of training programs and/or applying candidates (e.g., psychiatry, neurology, anesthesiology, and pediatrics) (NESCON, 2009). Based on this survey, in 2010, the Ministry of Education established the National Program to Support Training of Medical Specialists in Strategic Areas, which provides scholarships for medical residents in priority areas of the UNHS. Medical genetics, however, was not contemplated in this program (Ministério da Saúde, 2009b).
There are only 11 Medical Genetics residency programs in the country, offering a total of 21 new positions every year; except for one program associated with the University of Brasilia (Midwest), all the others are in the South or the Southeast (Fig. 1). The Brazilian Society of Medical Genetics believes that the nonrecognition and formalization of clinical genetics as a medical specialty in the public health system prevents the creation of new clinical genetics centers and is a disincentive for the new physicians specializing in this area.
Decision About Prioritization of Genetic Testing in Brazil
Recently, the European Society of Human Genetics (ESHG) published recommendations about genetic testing for common diseases of a complex inheritance. For the genetic tests whose clinical utility is uncertain, the ESHG suggests no incorporation or exclusion from coverage in the health system (Becker et al., 2011). This is the case with most susceptibility genetic tests for common diseases, often made available prematurely, without evidence of benefit, effectiveness, and clinical utility (Rogowski, 2006; Rogowski et al., 2009; Grosse et al., 2010).
In the common disorders that have a monogenic etiology in about 5% to 10% of the cases, such as breast and ovarian cancer and hereditary nonpolypomatous colorectal cancer, the ESHG recommends the selection of patients at a higher risk through family history, which will increase the predictive value of genetic testing (Becker et al., 2011).
In some specific situations, molecular testing for somatic mutations and pharmacogenetic tests should also be incorporated, provided there is evidence of clinical utility and cost effectiveness (Becker et al., 2011). This applies, for example, to the case of testing for the human epidermal growth factor receptor 2 (HER2) gene in patients with invasive breast cancer, as randomized studies proved that the use of the trastuzumab (Herceptin®), a monoclonal antibody that blocks the receptor in question, improves the response rates to chemotherapy, decreasing the time of tumour progression and improving survival in HER2-positive patients (Wolff et al., 2007).
The ESGH proposes equity in access to genetic testing, prioritizing those who need it the most. Therefore, it recommends that, for developing countries such as Brazil, the priority is to offer genetic diagnosis for children and adults with physical, sensory, or intellectual disabilities that are monogenic and highly penetrant, followed by programs on prevention of the related morbidity and mortality. If the clinical utility of a genetic test is proved, as is the case with most monogenic diseases, then the governments of developing countries have the additional responsibility of avoiding a gap in access between those who can and those who cannot pay, offering them within the public health system (Becker et al., 2011).
For the prevention and control of common diseases, much is to be gained by raising the standards of living (as balanced nutrition and avoidance of deleterious environmental agents, such as smoking) and improved access to primary health care (Becker et al., 2011).
In Brazil, the advances in medical genetics and genetic testing are not yet accessible by the vast majority of the population, as those tests are not routinely available through the UNHS. Only a small segment of the population has access to these, through teaching hospitals, where testing is often offered in the research context, or through private care, in a situation of social injustice. The distribution of teaching hospitals over the various regions of the country is roughly equivalent to the population density and the HDI in the country, with 46.72% of the hospitals being located in the Southeast and 23.77% in the South, where both the population density and the HDI are higher. The Brazilian Association of University and Teaching Hospitals (ABRAHUE, www.abrahue.org.br; 12/12/11) has 122 teaching hospitals registered, spreading across 22 of the 27 federal units (only five of the seven states in the North of Brazil do not have any teaching hospitals). All teaching hospitals provide their services to the UNHS, with no restrictions, depending only on their capacity, technological capabilities, and scope of care. In general, genetic tests will be available in all those teaching hospitals that have genetics services.
In April 2008, the Brazilian National Health Insurance Agency increased the minimum coverage for beneficiaries of private health care, whose plans had been purchased after 1 January 1999, including a new version of the Procedures Roll and Health Events, comprising 24 procedures in medical genetics, adding some genetic tests, such as karyotype with bands and molecular analysis of DNA, provided there was a criterion for its use. This measure benefited about 40 million Brazilians who have private health insurance, but clearly increased the inequity in health care for medical genetics and genetic testing.
In 2004, a directive from the Federal Council of Medicine (CFM, www.cfm.org.br; 12/12/11 - an organ with the constitutional duty of supervising and regulating medical practice in Brazil) and the Brazilian Medical Association (AMB, Associação Médica Brasileira) titled “Medical Genetics: Laboratory Testing for Diagnosis of Symptomatic Disease” stated that genetic testing for diagnosis in symptomatic patients should be conducted whenever the result had the potential to be appropriate for their clinical management (Raskin et al., 2004); however, decisions about taking a genetic test were left to the physician and the patient, without any further regulation. That is, even if the test has no clinical utility, it can be performed in a private laboratory, and the cost can be reimbursed by private health insurance.
The lack of regulation of genetic testing in the Brazilian UNHS has also generated several cases where the public health system was forced, by a court order, to reimburse a test performed at a private laboratory, based on the principle of the comprehensiveness of the UNHS, regardless of its being really useful, appropriate, or prioritary.
In 2001, a previous guideline of the CFM and the AMB specifically addressed predictive genetic testing. For these tests, three different situations were recognized: (1) predictive testing for late-onset diseases for which there is no treatment, such as neurodegenerative diseases—the recommendation here was to conduct testing only in adults who seek it spontaneously, when subjected to pre- and post-test consultation, including psychosocial evaluation and genetic counseling; (2) predictive testing for diseases for which therapeutic or preventive measures are available, either to prevent, delay, or minimize disease symptoms, as is the case in the several inborn errors of metabolism, such as Gaucher disease, homocystinuria, and alpha1-antitrypsin deficiency—under these circumstances, the recommendation is to test persons of any age because of the benefits derived; (3) predictive testing to assess the susceptibility for complex diseases, such as diabetes or hypertension—the recommendation here is against testing because of questionable predictive value (Lopes-Cendes et al., 2001).
Despite all difficulties in integrating clinical genetics in the Brazilian UNHS, genetic tests are already in the market and are offered, albeit unevenly, to patients either in the private health sector or through research in universities and main hospitals. A draft of a bill is still pending in the House of Representatives, in Brasilia (PL 4097/2004), which would establish the conditions for the realization and analysis of genetic testing in humans. A practical aspect still waiting to be regulated involves the specific requirements for genetics labs, the offer of genetic tests, including their selling direct-to-consumer (DTC) (for which no concrete legislation exists as yet). Nevertheless, the Brazilian Society of Genetics produced a document titled “Guide to good laboratory practices in human cytogenetics and molecular genetics,” for genetic testing laboratories, although it does not fill all the gaps, with regard to the certification and quality control of the laboratories (Borovik et al., 2004). The lack of regulation of genetic testing in Brazil encourages the creation of private laboratories, sometimes of dubious quality; stimulates the provision of genetic testing with no proven clinical utility; facilitates DTC testing, without a medical prescription and adequate genetic counseling; often wastes scarce resources; and further increases inequities and injustice in the access to health care. Although there are no Brazilian companies offering DTC genetics testing, some foreign companies offer this service over the Internet. There is no way of knowing what the real impact of their business is in Brazil (there are no studies published or surveys made, to the best of our knowledge), but we believe that, as in other countries, this is not very significant.
The biggest challenges in this area, in Brazil, are as follows: (1) to counter the indiscriminate supply and resource dispersal with tests of doubtful clinical validity and utility; (2) to set the proper standards and assessment procedures for genetic tests already being offered or to be newly introduced; (3) to establish adequate prioritization among the various types and contexts of genetic tests; (4) to promote education and training and a regionally fair distribution of skilled professionals (laboratory and clinical geneticists, as well as genetic counselors and nurses); thereby (5) expanding the access for users of the UNHS to appropriate and useful genetic testing, by adding effective health technology assessment, ethical meaning, and social responsibility to the provision of medical genetics services in Brazil.
Footnotes
Acknowledgments
The authors are grateful to the São Paulo Research Foundation (Fundação de Amparo à Pesquisa do Estado de São Paulo, FAPESP) for financial support in the form of a postdoctoral fellowship to D.G.Melo (process No 2010/16613-9).
Authors' Contributions
D.G. Melo created a draft of the manuscript that was critically revised by J.Sequeiros. Both the authors read and approved the final submitted version of this article.
Author Disclosure Statement
The authors declare that they have no competing interests.