
Abstract
Objective: The aim of this study was to determine whether the tumor necrosis factor-alpha-inducible protein 3 (TNFAIP3) polymorphisms confer susceptibility to systemic lupus erythematosus (SLE) in ethnically different populations. Methods: The authors conducted meta-analyses on associations between the TNFAIP3 polymorphisms and SLE susceptibility, using fixed and random effects models. Results: A total of eight comparative studies were included in this meta-analysis, which included four Asian, three European, and one African American population. Meta-analysis revealed that an association was found between the minor allele of rs2230926 and SLE in all subjects (odds ratio [OR] 1.848, 95% confidence interval [CI] 1.547-2.208, p<1.0×10−9). After stratification by ethnicity, the minor allele of rs2230926 was found to be significantly associated with SLE in Asians and Europeans (OR 1.821, 95% CI 1.495-2.219, p<1.0×10−9; OR 2.251, 95% CI 1.830-2.768, p<1.0×10−9). In addition, a significant association was found between the minor allele of the rs5029939 polymorphism and the risk of developing SLE in all study subjects and Europeans (OR 1.804, 95% CI 1.255-2.592, p=0.001; OR 2.145, 95% CI 1.731-2.658, p<1.0×10−9). Furthermore, an association was found between the minor allele of rs3757173 and SLE in all study subjects (OR 1.540, 95% CI 1.017-2.331, p=0.041). However, no association was found between SLE susceptibility and rs6922466 (OR 0.953, 95% CI 0.812-1.120, p=0.561). Conclusions: This meta-analysis confirms that the TNFAIP3 polymorphisms are associated with SLE susceptibility in different ethnic groups, namely in Asians and Europeans.
Introduction
S
The tumor necrosis factor alpha inducible protein 3 (TNFAIP3) encodes ubiquitin-editing protein A20, which is an inhibitor of nuclear factor-κB (NF-κB) activity in several signaling pathways, including those of TNF and Toll-like receptors (Boone et al., 2004). Furthermore, A20-deficient mice show systematic inflammation, a damage involving kidneys and joints, and develop lupus-like autoimmunity (Lee et al., 2000). TNFAIP3 participates in the negative regulation of inflammatory responses, and alterations in the activity or expression of TNFAIP3-encoded A20 may influence the pathogenesis of SLE (Tavares et al., 2010). The TNFAIP3 gene is located at 6q23, and is known to be associated with susceptibility to multiple autoimmune diseases (Dieude et al., 2010). In particular, rs2230926 is located in the coding region of TNFAIP3, and an amino acid substitution of Phe to Cys at position 127 in the ovarian tumor domain has been suggested to play a role in the inhibitory function of A20 (Coornaert et al., 2009). The Cys127 allele product is modestly less effective at inhibiting NF-κB activation by TNF than the Phe127 allele product (Musone et al., 2008). In a recent study, it was shown that a strong association exists between rs5029939 and SLE (Graham et al., 2008). In addition, it was found that a tight linkage disequilibrium (LD) exists between rs5029939 and rs2230926 (Lodolce et al., 2010).
Associations between the TNFAIP3 polymorphisms and SLE have been reported in different ethnic groups (Graham et al., 2008; Musone et al., 2008; Bates et al., 2009; Cai et al., 2010; Kawasaki et al., 2010a; Lodolce et al., 2010; Shimane et al., 2010; Yang et al., 2010). Typically, the allelic frequencies of genes often differ substantially in different ethnic groups, and thus ethnically specific association studies are required to determine genetic associations in different populations (Nath et al., 2005; Lee et al., 2006a, 2006b). In the present study, we investigated whether the TNFAIP3 polymorphisms contribute to SLE susceptibility in different populations using a meta-analysis approach.
Materials and Methods
Identification of eligible studies and extraction of data
A literature search was conducted for studies that examined associations between the TNFAIP3 polymorphisms and SLE. The MEDLINE citation index was utilized to identify articles in which the TNFAIP3 polymorphism was determined in SLE patients and controls (until February 2012). In addition, all references mentioned in identified articles were reviewed to identify additional studies not indexed by MEDLINE. The following key words and subject terms were searched: “tumor necrosis factor alpha inducible protein 3,” “TNFAIP3,” “systemic lupus erythematosus,” and “SLE.” The following information was extracted for each study: author, year of publication, ethnicity of the study population, demographics, numbers of cases and controls, and the allele frequencies of the TNFAIP3 polymorphisms.
Evaluation of publication bias
Funnel plots are used to detect publication bias, but require studies with different sizes that involve subjective judgments. Thus, we evaluated publication bias using Egger's linear regression test (Egger et al., 1997a), which measures funnel plot asymmetry on a natural logarithm scale of odds ratios (ORs).
Evaluation of statistical associations
Allele frequencies of the TNFAIP3 polymorphisms in each of the studies were determined using the allele counting method. Allelic effect contrast for two (the minor allele) versus one (the common allele) was examined, and point estimates of risk, ORs, and 95% confidence intervals (CIs) were determined for each study. Cochran's Q-statistic was used to assess within and between study variations and heterogeneities (Davey Smith and Egger, 1997). Heterogeneity testing was performed to assess the probability of the null hypothesis, namely that all studies evaluated the same effect. When a significant Q-statistic (p<0.10) indicated heterogeneity across studies, the random effects model was used for meta-analysis, and when heterogeneity was not indicated across studies, the fixed effects model was used. Fixed effects assume that genetic factors have similar effects on SLE susceptibility across all studies, and that observed variations between studies are caused by chance alone (Egger et al., 1997b). The random effects model assumes that different studies show substantial diversity, and assess both within-study sampling errors and between-study variances (DerSimonian and Laird, 1986). The random effects model is used in the presence of significant between-study heterogeneity. We quantified the effect of heterogeneity by using a recently developed measure, namely I2=100%×(Q-df)/Q (Higgins and Thompson, 2002). I2 ranges between 0% and 100% and represents the proportion of interstudy variability attributable to heterogeneity rather than chance. I2 values of 25%, 50%, and 75% were defined as low, moderate, and high estimates, respectively. Statistical manipulations were undertaken using the Comprehensive Meta-Analysis computer program (Biosta; Englewood, NJ).
Results
Studies included in the meta-analysis
Electronic and manual searches resulted in the identification of 16 studies, and 11 were selected for a full-text review based on their titles and abstracts (Graham et al., 2008; Musone et al., 2008; Bates et al., 2009; Han et al., 2009; Cai et al., 2010; Kawasaki et al., 2010a, 2010b; Lodolce et al., 2010; Shimane et al., 2010; Yang et al., 2010; Adrianto et al., 2011). Two studies were excluded because they contained no extractable data (Han et al., 2009; Adrianto et al., 2011), and one was excluded because it contained duplicated data (Kawasaki et al., 2010b). Thus, eight studies were considered in this meta-analysis (Graham et al., 2008; Musone et al., 2008; Bates et al., 2009; Cai et al., 2010; Kawasaki et al., 2010a; Lodolce et al., 2010; Shimane et al., 2010; Yang et al., 2010), which included four Asian, three European, and one African American population (Table 1). Due to the limited number of studies, meta-analyses were conducted separately on the rs2230926, rs5029939, rs6922466, and rs3757173 polymorphisms. The selected characteristics of the eight studies included are summarized in Table 1.
SLE, systemic lupus erythematosus; TNFAIP3, tumor necrosis factor-alpha-inducible protein 3; E, European; A, Asian; AA, African American; USA, United States of America; NS, not significant.
Frequency of the minor allele of the TNFAIP3 rs2230926 polymorphism in the control groups
The mean frequency of the T allele was found to be 8.2% among all controls. The European controls had the lowest T-allele prevalence (2.5%). Frequencies ranged from 5.1% to 31.7% in these other ethnic groups, and African Americans had the highest T-allele frequency (31.7%) (Table 2).
Meta-analysis of the association between the TNFAIP3 polymorphisms and SLE
Meta-analysis was performed on all SLE patients and on SLE patients in each ethnic group. A summary of the meta-analysis findings of the relations between the TNFAIP3 polymorphisms and SLE is provided in Table 3. Meta-analysis showed an association between the minor allele of rs2230926 and SLE in all study subjects (OR 1.848, 95% CI 1.547-2.208, p<1.0×10−9) (Table 3, Fig. 1). Analysis after stratification by ethnicity indicated that the minor allele of rs2230926 was significantly associated with SLE in Asians and Europeans (OR 1.821, 95% CI 1.495-2.219, p<1.0×10−9; OR 2.251, 95% CI 1.830-2.768, p<1.0×10−9) (Table 3). The analysis performed in the single African American study showed a significant association between the minor allele and SLE (Table 3).
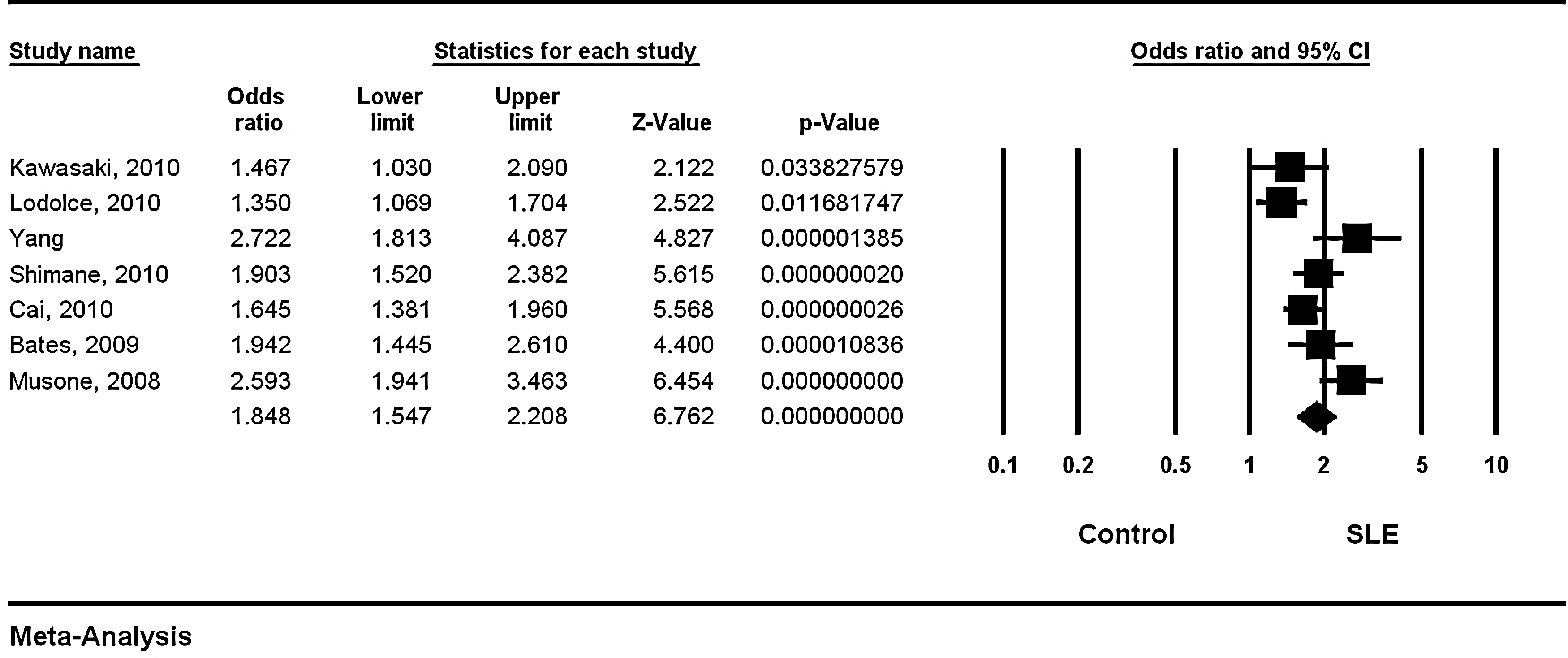
Odds ratios (ORs) and 95% confidence intervals (CIs) of individual studies and pooled data for the minor versus major allele of the tumor necrosis factor-alpha-inducible protein 3 (TNFAIP3) rs2230926 polymorphism with respect to susceptibility to systemic lupus erythematosus (SLE) in all study subjects.
OR, odds ratio; CI, confidence interval; F, fixed effects model; R, random effects model; NA, not available.
Meta-analysis revealed a significant association between the minor allele of the rs5029939 polymorphism and the risk of developing SLE in all study subjects and in Europeans (OR 1.804, 95% CI 1.255-2.592, p=0.001; OR 2.145, 95% CI 1.731-2.658, p<1.0×10−9) (Table 3, Fig. 2). The original analysis performed in the African American study showed a significant association between the minor allele of rs5029939 and SLE (Table 3). Meta-analysis revealed an association between the minor allele of rs3757173 and SLE in all study subjects (OR 1.540, 95% CI 1.017-2.331, p=0.041) (Table 3, Fig. 2). The original analysis performed in the single Asian study showed a significant association between the minor allele of rs3757173 and SLE (OR 1.947, 95% CI 1.352-2.804, p=3.4×10−4), and the original analysis in the African American study revealed a marginal association between the minor allele of rs3757173 and SLE (Table 3). No association was found between SLE susceptibility and rs6922466 by meta-analysis (OR 0.953, 95% CI 0.812-1.120, p=0.561) (Table 2). Furthermore, stratification by ethnicity failed to identify any association between this rs6922466 polymorphism and SLE in Europeans or Asians (Table 2).

ORs and 95% CIs of individual studies and pooled data for the minor versus major allele of the rs5029939
Heterogeneity and publication bias
Both heterogeneity and publication bias tests were conducted in the meta-analyses of all of the TNFAIP3 polymorphisms. Between-study heterogeneity was found for the rs2230926 in the overall and Asian groups, and for rs5029939 and rs3757173 in all study subjects (Table 2). However, no evidence of heterogeneity was found for the rs2230926 and rs5029939 polymorphisms in Europeans or for the rs6922466 polymorphism in all study subjects (Table 2). It was found to be difficult to correlate funnel plots, which are usually used to detect publication bias, because of the small number of studies included. Egger's regression test showed no evidence of publication bias in this meta-analysis of the TNFAIP3 polymorphisms in any group analyzed (Egger's regression test p-values>0.1) (Fig. 3).
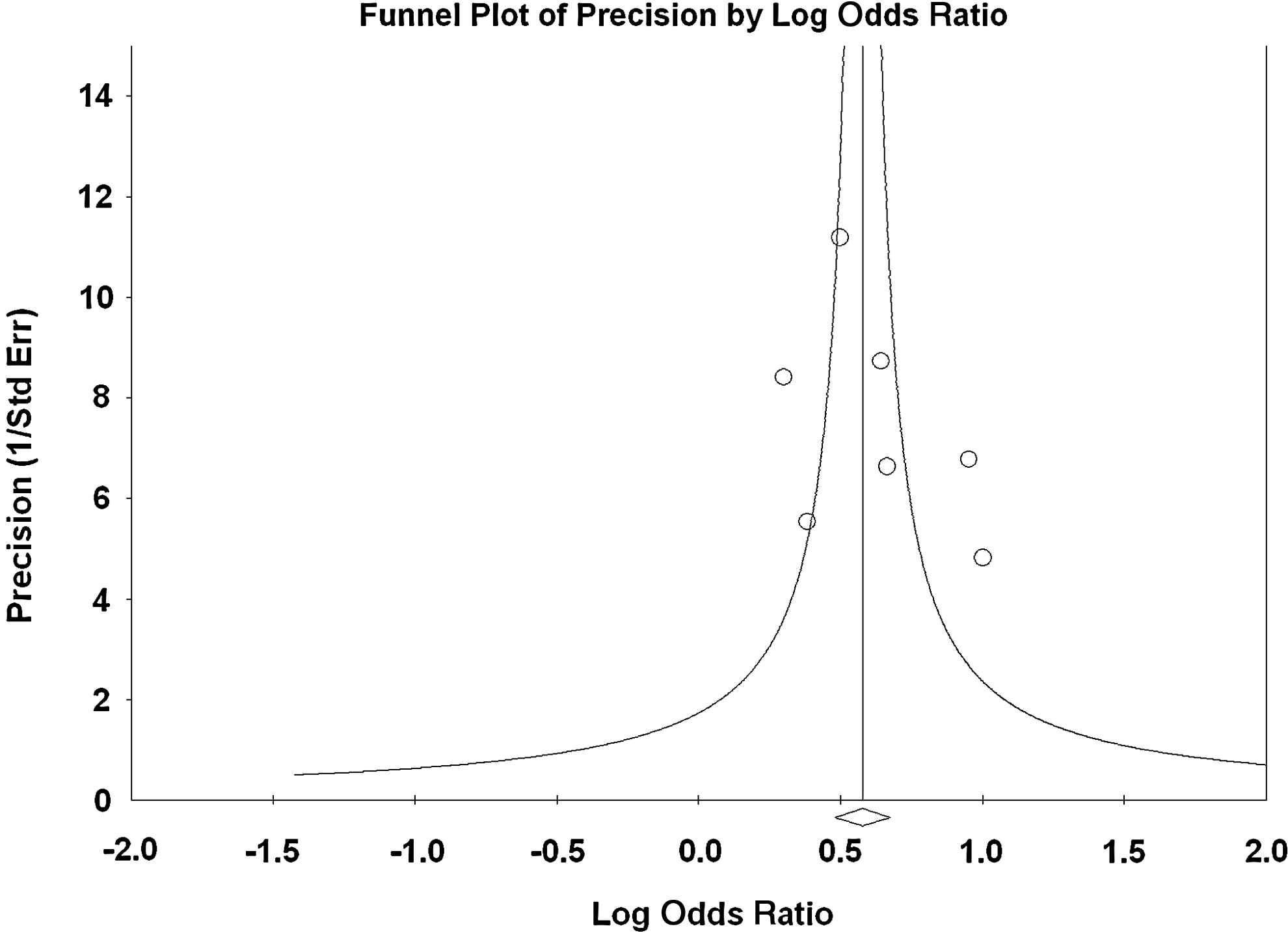
Funnel plot of studies regarding the association between the minor allele of the TNFAIP3 rs2230926 polymorphism and SLE in all patients (Egger's regression p-value=0.291).
Discussion
In this meta-analysis, we examined evidence of associations between TNFAIP3 polymorphisms and SLE susceptibility. Our results provide evidence of a strong association between the TNFAIP3 polymorphisms and SLE. Although our findings do not support associations between the rs6922466 polymorphism and SLE susceptibility, our analysis revealed significant associations between the rs2230926 polymorphism and the risk of developing SLE in Asians, Europeans, and African Americans. Furthermore, our study shows an association between SLE and the rs5029939 polymorphism in Europeans and African Americans, and between rs3757173 and SLE in Asians. We could not include a recent large-scale study by Adrianto et al. (2011) on the TNFAIP3 polymorphisms in SLE, because the results of the TNFAIP3 polymorphisms were not available. The association results from the large-scale study by Adrianto et al. were consistent with our meta-analysis results, showing an association of rs2230926, rs5029939, and rs3757173 with SLE in Europeans and Asians. These findings suggest that the TNFAIP3 polymorphisms are associated with the development of SLE in Europeans and Asians.
The prevalence of the minor allele of the rs2230926 polymorphism was calculated in different populations, and was found to vary between 2.5% and 31.7%. Its mean frequency in all controls was 8.2%, and its frequency was lowest among the European controls and highest among the African American controls. Furthermore, our ethnic-specific meta-analysis showed that an association exists between the rs2230926 polymorphism and SLE in Europeans and Asians. Unfortunately, meta-analysis of the rs2230926 polymorphism was not possible in African Americans due to limited data.
The disease-associated variant of rs2230926 is a nonsynonymous variant that results in a phenylalanine-to-cysteine change at residue 127 of A20, a key player in anti-inflammatory reactions. The risk allele (Cys127) leads to reduced inhibition of NF-κB activation or reduced mRNA level of TNFAIP3 (Musone et al., 2008). These findings suggest that reduced negative regulatory activity of A20 protein leads to excessive immune activity, and thus enhanced autoreactivity. In addition, rs5029939, which is in strong LD with rs2230926, was found to be associated with lower TNFAIP3 mRNA expression (Lodolce et al., 2010). These findings suggest that both rs2230926 and rs5029939 play a functional role in the development of SLE.
Our analysis differs slightly from the previous meta-analysis performed on relations between the TNFAIP3 polymorphisms and SLE performed by Fan et al. (2011). In this previous study, one polymorphism (rs2230926) in the TNFAIP3 gene was analyzed, whereas we did meta-analyses on rs2230926, rs5029939, rs6922466, and rs3757173 polymorphisms. Furthermore, in this previous analysis, subgroup analysis was not performed by ethnicity, whereas in the present study, meta-analysis was undertaken to evaluate the genetic associations between the TNFAIP3 polymorphisms and SLE susceptibility in different populations, and revealed significant associations between the TNFAIP3 polymorphisms and SLE in Asians and Europeans.
Several limitations of the present study require consideration. First, publication bias, heterogeneity, and confounding factors may have distorted the meta-analysis. However, most of the studies enrolled demonstrated the same directionality with respect to associations between the TNFAIP3 polymorphisms and SLE. Second, only data from European and Asian patients were included in the ethnic-specific analysis, and thus our results are applicable to only these ethnic groups. Third, most of the studies included were performed in the populations of Asian and European descent—only one study was conducted in African Americans. The allelic frequencies of genes often differ substantially between populations, and thus further ethnicity-specific association studies are required to confirm genetic associations regarding SLE susceptibility in different populations. Fourth, the TNFAIP3 polymorphisms have also been reported to be associated with the severity of autoimmune diseases (Bates et al., 2009), but limited data prevented our examining the associations between the TNFAIP3 polymorphisms and the clinical manifestations of SLE.
In conclusion, this meta-analysis of published data confirms that the TNFAIP3 polymorphisms are associated with SLE susceptibility in Asians and Europeans. Furthermore, it shows that the prevalence of the minor allele of rs2230926 in the TNFAIP3 gene is ethnicity dependent. Further studies are required to determine whether the TNFAIP3 polymorphisms contribute to SLE susceptibility in different ethnic groups.
Footnotes
Author Disclosure Statement
No competing financial interests exist.