
Abstract
Currently, concerns of clopidogrel and proton pump inhibitors (especially omeprazole) interaction are raised, because they are both metabolized by CYP2C19. What is more, omeprazole can also inhibit the activity of CYP2C19. The study was to compare the influence of omeprazole on platelet inhibition of clopidogrel in various CYP2C19 mutant alleles. One hundred forty-two consecutive patients undergoing elective coronary stenting received aspirin and clopidogrel, and were randomized to omeprazole or the placebo. Enrolled patients were analyzed for adenosine diphosphate-induced platelet aggregation (ADP-Ag), and CYP2C19*2 and CYP2C19*3 were identified by polymerase chain reaction-restriction fragment length polymorphism. Of the patients included, 47 (33.1%) belonged to homozygous extensive metabolizers (homEMs) (CYP2C19*1/*1), 70 (49.3%) belonged to heterozygous extensive metabolizers (hetEMs) (*1/*2 or *1/*3), and 25 (17.6%) belonged to poor metabolizers (PMs) (*2/*3 or *2/*2). ADP-Ag had a significant difference among the three genotypic groups (p<0.01). Moreover, the present study revealed that the degree of the interaction between clopidogrel and omeprazole was not homogeneous within the various genotypes of CYP2C19. The difference of ADP-Ag between the patients with and without omeprazole was significantly largest in homEMs (45.7%±14.2% vs. 35.5%±16.0%, p<0.05). However, any significant difference of ADP-Ag between the patients with and without omeprazole was not observed in other two genotypic groups (hetEMs and PMs, p>0.05). In conclusion, concomitant therapy with omeprazole appears to reduce the antiplatelet effect of clopidogrel most significantly in homEMs of CYP2C19.
Introduction
Methods
Patients
Patients >18-years old who underwent successful percutaneous coronary intervention with drug-eluting stents were prospectively eligible for inclusion. Inclusion criteria were symptomatic coronary artery disease or documented by revascularization or myocardial infarction. Exclusion criteria were history of thrombocytopenia (platelet count <100×109/L) or bleeding disorder, serious liver disease, gastrointestinal ulcer, use of glycoprotein (GP) IIb/IIIa inhibitors before the procedure, and previous allergy to or prior use of clopidogrel or PPIs. Patients received a 300-mg loading dose of clopidogrel and a 300-mg loading dose of aspirin at least 12 h before stenting. Stents were deployed according to standard techniques. Anticoagulation was obtained with low-weight-molecular heparin when possible, or unfractionated heparin in patients older than 75 years of age or with renal failure. Use of a GP IIb/IIIa antagonist was allowed at the operator's discretion during the procedure. Maintenance doses were clopidogrel 75 mg and aspirin 100 mg daily. At the start of clopidogrel treatment, patients were randomized to omeprazole 20 mg/day or placebo with randomization by sealed envelopes. Enrolled patients were analyzed for post-treatment platelet reactivity with adenosine diphosphate-induced platelet aggregation (ADP-Ag), and given genetic analysis.
Patients were documented for atherosclerosis risk factors, such as diabetes mellitus, arterial hypertension, hypercholesterolemia, and smoking status. Concomitant cardiovascular medications (β-blockers, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, calcium channel blockers, and statins) at inclusion were also recorded. The ethics committee of our institution approved the study protocol.
Platelet reactivity
Blood samples for testing platelet reactivity were drawn at least 12 h after clopidogrel and omeprazole co-therapy, and before administration of GP IIb/IIIa antagonist if needed. The blood-citrate mixture was centrifuged at 800 rpm for 10 min. The resulting platelet-rich plasma was kept at room temperature for use within 1 h. Platelet-rich plasma obtained by further centrifugation of samples at 4000 rpm for 10 min was used to adjust the platelet count to 2.5×108/mL. Platelets were stimulated with ADP (5 μM), and aggregation was assessed with a PACKS-4 Aggregometer. Aggregation was expressed as the percentage change in light transmittance from baseline with platelet poor plasma as a reference. Here we analyzed data on the maximal intensity of ADP-Ag. An ADP-Ag >50% was defined as high post-treatment platelet reactivity (HTPR) as previously described (Barragan et al., 2003; Cuisset et al., 2008).
DNA extraction
Genomic DNA was isolated from whole blood by BioSpin Whole-Blood Genomic DNA Extraction Kit.
Genotyping
The CYP2C19 wild-type gene and two mutated alleles, CYP2C19*2 in exon 5 and CYP2C19*3 in exon 4, were identified by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). For the analysis of the CYP2C19*2 allele, the forward and reverse primers were 5′-AATTACAACCAGAGCTTGGC-3′ and 5′-TATCACTTTCCATAAAAGCAAG-3′. The final 50 μL of PCR mixture contained 34 μL of PCR-grade water, 5.0 μL of 10×PCR buffer with 15 mM MgCl2, 4.0 μL of deoxyribonucleoside triphosphates (2.5 mM each), 1.0 μL of primers (10 mM each), 1.0 μL of Taq DNA polymerase (5 U/μL; BioFlus), and 4.0 μL of genomic DNA sample. Temperature cycling proceeded as follows: initial denaturation for 5 min at 94°C, followed by 35 cycles of 30 s at 94°C, 30 s at 55°C, 40 s at 72°C, and a terminal extension for 7 min at 72°C. The forward and reverse primers used for detection of the CYP2C19*3 allele were 5′-AAATTGTTTCCAATCATTTAGCT-3′ and 5′-ACTTCAGGGCTTGGTCAATA-3′. The reaction system and amplification conditions were similar to those of the CYP2C19*2, except that the annealing temperature was 53°C. The 169- and 271-bp gene fragments were amplified by PCR, respectively, and their products were digested with the restriction endonucleases (SmaI [Fermentas] for CYP2C19*2 and BamHI [Fermentas] for CYP2C19*3). The digested products were analyzed on 3% agarose gels and stained with ethidium bromide.
Statistics
The SPSS statistical package Version 14.0. was used for statistical analysis. Continuous variables were expressed as mean±standard deviation. Categorical variables were expressed as frequencies and percentages. Groups were compared with the chi-square or Fisher exact test for categorical variables. Continuous variables among groups were tested via Student's t-tests and one-way analysis of variance or nonparametric statistical testing (Mann-Whitney) when there was no variance homogeneity.
Results
A total of 142 consecutive patients were prospectively included in the study, and given a genetic analysis. Baseline characteristics of the patients are summarized in Table 1. Demographic indicators and concomitant medications were well balanced among the treatment groups at baseline.
homEMs, homozygous extensive metabolizers; hetEMs, heterozygous extensive metabolizers; PMs, poor metabolizers; PPI, proton pump inhibitors; ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin II receptor blockers.
Of the patients, 47 (33.1%) belonged to homozygous extensive metabolizers (homEMs; *1/*1), 70 (49.3%) belonged to heterozygous extensive metabolizers (hetEMs; *1/*2 or *1/*3), and 25 (17.6%) belonged to poor metabolizers (PMs; *2/*3 or *2/*2). However, homozygotes for CYP2C19*3 were not found in the study. The allele frequencies of the CYP2C19*2 and CYP2C19*3 mutations in the subjects were 0.38 and 0.05 (data not shown), respectively. ADP-Ag was significantly different among the three genotypic groups: 42.0%±15.5% in homEMs, 44.2%±13.9% in hetEMs, and 53.3%±14.1% in PMs (p<0.01). What is more, the prevalence of HTPR in EM genotypic groups was 35.0% (31.9% in homEMs and 37.1% in hetEMs), significantly lower than PM genotypic groups (p<0.01, Table 2). The prevalence of HTPR in PMs was 68.0%.
HTPR, high post-treatment platelet reactivity.
The patients were randomized to receive omeprazole (n=83, 59.2%). Patients without PPIs had a better platelet response to clopidogrel significantly assessed by ADP-Ag: 41.4%±15.5% versus 47.8%±14.0% (p<0.05). The difference of ADP-Ag between the patients with and without omeprazole was significantly largest in homEMs (45.7%±14.2% vs. 35.5%±16.0%, p<0.05, Fig. 1), indicating the effect of omeprazole on attenuated platelet inhibition of clopidogrel in homEMs. We identified more clopidogrel nonresponders in the omeprazole group than in the placebo group: 38.7% versus 18.8% (p<0.05, Fig. 2). However, any significant difference of ADP-Ag between the patients with and without omeprazole was not observed in other two genotypic groups (hetEMs and PMs, p>0.05, Fig. 1).
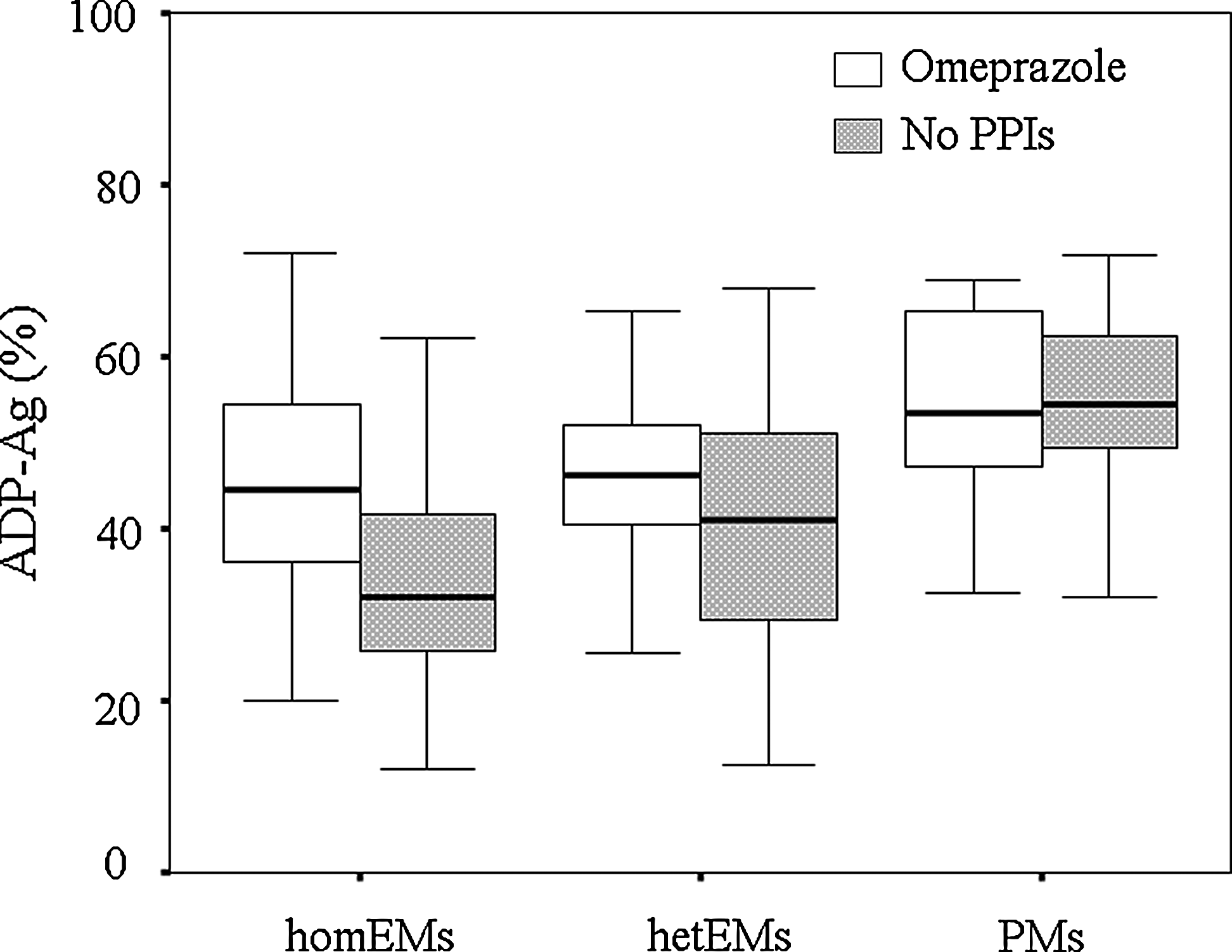
Mean values of ADP-Ag between the patients with and without omeprazole among the various CYP2C19 genotypic groups. The difference of ADP-Ag values between the patients with and without omeprazole was significantly largest in homEMs: 45.7%±14.2% versus 35.5%±16.0%, p=0.028. However, ADP-Ag between the patients with and without omeprazole was 47.2%±13.1% and 41.4%±14.4% in hetEMs, respectively (p=0.085), and patients with or without omeprazole had similar ADP-Ag values in PMs (53.9±13.0 vs. 52.9±15.0, p=0.864). ADP-Ag, adenosine diphosphate-induced platelet aggregation; homEMs, homozygous extensive metabolizers; hetEMs, heterozygous extensive metabolizers; PMs, poor metabolizers.
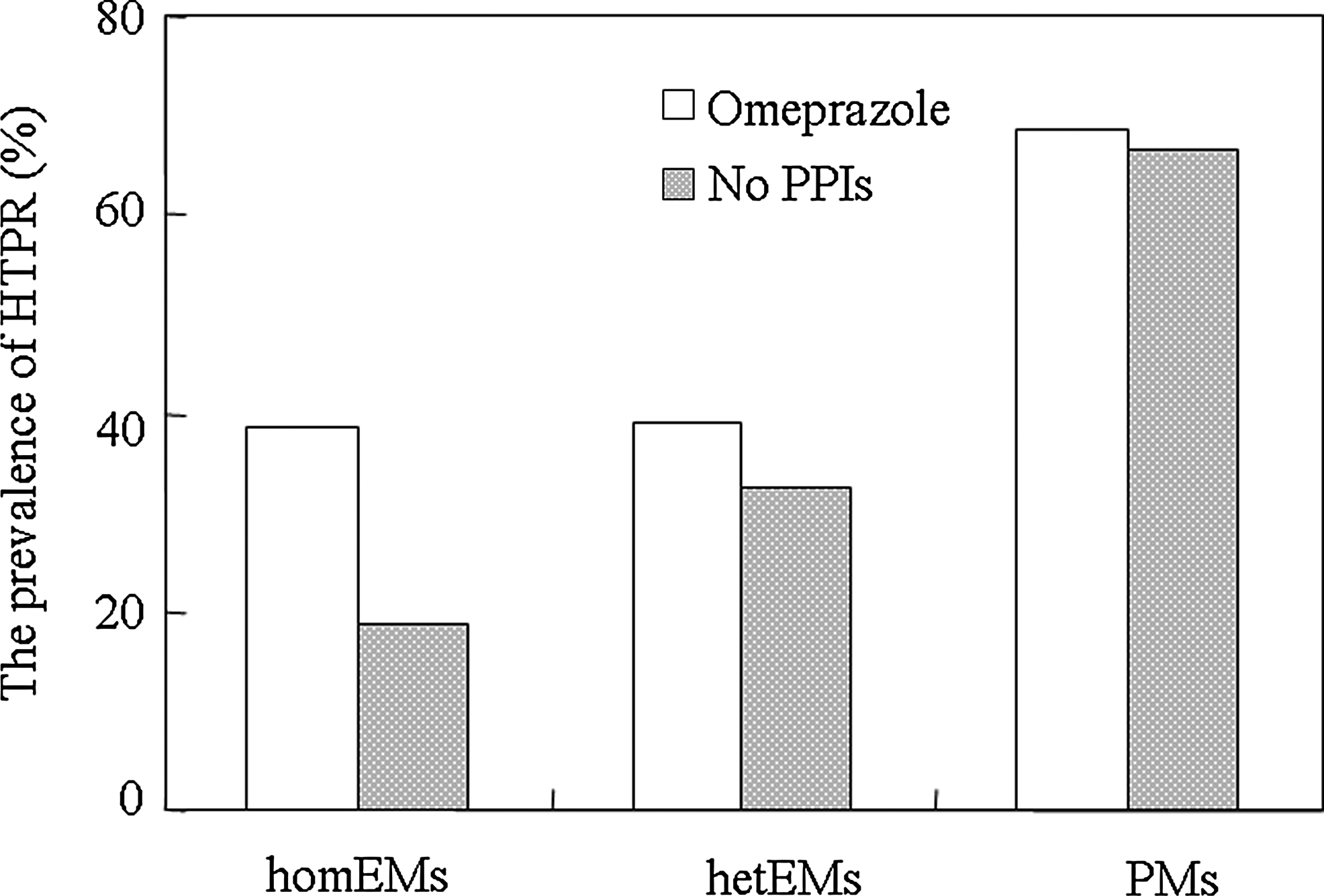
Differential prevalence of HTPR between the patients with and without omeprazole among the various CYP2C19 genotypic groups. They were not homogeneous within the various genotypic groups: 38.7% versus 18.8% in homEMs (p=0.049), 38.9% versus 32.4% in hetEMs (p=0.568), and 68.9% versus 66.7% in PMs (p=1.000). HTPR, high post-treatment platelet reactivity.
Discussion
CYP2C19 plays an important role in the bioactivation of clopidogrel. Once absorbed, only ∼15% of clopidogrel is bioactivated by two sequential steps dependent on several CYP450 isoenzymes (Kazui et al., 2010), with contributions from the isoenzymes CYP2C19, CYP3A4 or CYP3A5, CYP2C9, CYP1A2, and CYP2B6. Of these, CYP2C19 is responsible for ∼45% of the first step (the formation of 2-oxo-clopidogrel) and ∼20% of the final step to generate the pharmacologically active thiol metabolite. CYP2C19 is a polymorphically expressed enzyme (Goldstein, 2001), and the CYP2C19 gene is located on chromosome 10p, which has at least 25 variant mutations (Ingelman-Sundberg et al., 2009). CYP2C19*2 and *3, as the major mutant alleles of CYP2C19, are known to be associated with the genetically deficient metabolic activity, and have the highest occurrence among Asian populations (Desta et al., 2002). A number of studies have shown a considerable interethnic difference in the frequency of PMs of CYP2C19 19-23% among the Japanese population, 15% among the Chinese, and 13% among Koreans (Kubota et al., 1996; Shu and Zhou, 2000). This is much higher than that reported in Caucasian populations, which is 3-5% (Jacqz et al., 1988). The activity of CYP2C19 may influence the antiplatelet effect of clopidogrel in both healthy volunteers and patients (Chen et al., 2008; Simon et al., 2009), and our study also confirmed that the loss-of-function CYP2C19*2 and CYP2C19*3 alleles were associated with a poor response to clopidogrel. Other genetic polymorphisms (CYP2C19*3, *4, *5, and *8) associated with impaired CYP2C19 activity and possibly adverse clinical events are much less common in Asians, and thus were not investigated in the study.
This was the first time to investigate the influence of omeprazole on platelet inhibition of clopidogrel in various CYP2C19 mutant alleles. Concerns of PPIs and clopidogrel interaction were raised when omeprazole was found to inhibit the antiplatelet effect of clopidogrel in an in vivo study of 104 patients (Cuisset et al., 2009), because omeprazole is both a substrate and an inhibitor of CYP2C19. Ko et al. (1997) showed that omeprazole, but not other PPIs (esomeprazole, rabeprazole, and pantoprazole), appeared to inhibit CYP2C19 activity. What is more, the affinity of omeprazole for CYP2C19 may result in omeprazole being a more potent inhibitor of CYP2C19 isoenzyme. Therefore, metabolism of clopidogrel to its active form may be reduced in patients receiving omeprazole concomitantly (Siller-Matula et al., 2009). Indeed, Juurlink et al. (2009) suggested that among patients receiving clopidogrel after an acute myocardial infarction, a loss of the beneficial effects of clopidogrel was associated with concomitant therapy with omeprazole. However, the present study found that the degree of the interaction between clopidogrel and omeprazole was not homogeneous within the various genotypic groups. It confirmed that the use of omeprazole significantly reduced the antiplatelet activity of clopidogrel in homEMs, whereas omeprazole had no significant effect on platelet reactivity assessed by ADP-Ag in other genotypes (hetEMs and PMs), which has not been found in several other studies. The authors analyzed the potential causes: metabolic pathways of clopidogrel are dependent on several CYP450 isoenzymes, as previously mentioned. If the activity of the isoenzyme CYP2C19 is reduced, mainly caused by the loss-of-function alleles, its contribution to the metabolism of clopidogrel may be also minimized. Instead, other CYP450 isoenzymes may make more contribution to the metabolism of clopidogrel. However, omeprazole can just inhibit CYP2C19 activity, and thus it is less associated with a poor response to clopidogrel. It is suggested that among patients receiving clopidogrel after an acute myocardial infarction in homEMs, concomitant therapy with omeprazole appears to influence clopidogrel effect. However, the combination of clopidogrel and omeprazole can be continued to prevent patients in hetEMs and PMs from gastrointestinal bleeding. This is of great importance for daily practice, because omeprazole is now a standard medicine of care for patients receiving dual-antiplatelet therapy to prevent the risk of gastrointestinal bleeding (Bhatt et al., 2008).
Besides, studies examining the effect of various PPIs on the pharmacodynamics of clopidogrel have shown that omeprazole decreased the effect of clopidogrel, whereas lansoprazole, pantoprazole, and esomeprazole had no influence on the antiplatelet effect of clopidogrel (Gilard et al., 2008; Cuisset et al., 2009; Siller-Matula et al., 2009). A possible explanation is that metabolism of omeprazole mainly occurs through this pathway, while esomeprazole, pantoprazole, and lansoprazole are progressively less metabolized via this pathway. Additional large prospective clinical studies are required to confirm the interaction of clopidogrel and other PPIs for the patient with the loss-of-function alleles.
In conclusion, our study shows that the degree of the interaction between clopidogrel and omeprazole was not homogeneous within the various genotypes of CYP2C19. Concomitant therapy with omeprazole appears to reduce the clopidogrel effect significantly in homEMs, whereas omeprazole had no significant effect on the antiplatelet activity of clopidogrel in other genotypes (hetEMs and PMs).
Footnotes
Acknowledgments
The authors thanked their doctors, nurses, team, and technicians for assistance in executing this study.
Author Disclosure Statement
No competing financial interests exist.