
Abstract
Purpose: Physicians will play a large role in the delivery of genomic medicine, given the limited number of trained genetics professionals. The objective of this study was to assess physician preparedness for incorporating genomic testing (GT) and pharmacogenetic testing (PT) into practice by determining knowledge, experience, comfort level, and barriers, as well as their expectations for practice and educational needs. Methods: A 30-question survey was distributed to physicians spanning all disciplines within our healthcare system. Results: Perceived knowledge was poor; 40%-72% reported “no to minimal knowledge” for all genomics topics. Recent graduates or those with no patients who had undergone GT or PT had lower comfort levels. Participating physicians anticipate usage to increase; however, most were uncertain when and how to incorporate genomics into practice. Physicians perceived lack of knowledge and time to keep updated as their greatest barriers to incorporating GT and PT into practice. Conclusion: Overall, physicians appear underprepared, perceiving they lack sufficient knowledge and confidence to incorporate GT and PT into practice. The majority of physicians expect their role in GT and PT to increase. The results underscore the importance of enhancing policies and initiatives to increase physician knowledge and comfort level.
Introduction
Despite the increase in number of genetic tests, no parallel increase of genetics professionals has occurred. Sixty percent of physician and PhD members of the American Board of Medical Genetics perceive there to be too few geneticists (Cooksey et al., 2005). Currently, there are 1216 ABMG-certified Clinical Geneticists in the United States as of the 2011 exam cycle (ABMG, 2011). Genetic services for complex disease and pharmacogenetics will likely fall to primary care physicians (PCPs) or other nongenetic specialists.
Given the exponential rate of advancement, keeping healthcare professionals up-to-date on the benefits, risks, and limitations of new genetic technology will be difficult (Ginsburg, 2008). Studies have consistently found that physicians lack adequate knowledge when tested on basic genetic concepts (Metcalfe et al., 2002; Baars et al., 2005; Houwink et al., 2011). Little research has investigated physician knowledge regarding the genomics of complex disease and pharmacogenetics (Ginsburg, 2008; Avard and Knoppers, 2009). Twenty-nine percent of physicians surveyed by Medco Health Solutions, Inc., along with the American Medical Association, reported receiving prior education about pharmacogenomics. However, only 10% sampled felt adequately informed about pharmacogenomic testing (Stanek et al., 2009, 2012).
Few studies examined physicians' experiences with and preparedness for direct-to-consumer (DTC) genetic testing. A national survey of 1880 healthcare providers found that 7% had a patient with questions in the past year regarding DTC tests and 3% had a patient bring results for discussion (Kolor et al., 2009). Recently, in a survey of PCPs in North Carolina, 38.7% (148/382) heard about DTC genetic testing, but only 15% (57/380) felt prepared to answer a question about DTC genetic testing (Powell et al., 2011). Only 28 (18.9%) and 5 (3.3%) physicians had a patient(s) ask about DTC tests or bring tests results, respectively.
There appears to be a consensus that educational resources surrounding genomics and pharmacogenetics are necessary and would benefit physicians by increasing their knowledge base and improving genetic services (Frueh and Gurwitz, 2004; Ginsburg, 2008; Scheuner et al., 2008; Avard and Knoppers, 2009; Houwink et al., 2011; Powell et al., 2011). However, questions arise about the best educational methods to use to overcome these deficiencies (Valle and Manolio, 2008).
The purpose of this study is to (1) determine what experience physicians have had with genomics and pharmacogenetics in a community-based health system; (2) assess physician perceived knowledge of genomics and pharmacogenetics; (3) explore physician comfort level with genomic testing (GT); (4) assess physicians' expectations for the future of genomic medicine; (5) determine barriers preventing physicians from applying genomics to clinical management of patients; and (6) investigate physicians' educational resources and beliefs about future educational needs in genomic medicine.
Materials and Methods
A 30-item electronic anonymous survey was developed in consultation with a multidisciplinary group of physicians (geneticists, internists, vascular surgeons, and oncologists) and with InsightOut Chicago, a local market research company. E-mail invitations and reminders, including a weblink to the survey, were distributed to 2071 physicians spanning all medical disciplines within NorthShore University HealthSystem, a community-based health system. The survey was open from November 19, 2010, to December 7, 2010. Respondents who indicated involvement in direct patient care were directed to answer all questions; otherwise, they were solely asked questions regarding their knowledge of genomics, the resources they use surrounding genomics, and their anticipated educational needs. Participants were provided definitions for genomic medicine, pharmacogenetic testing (PT), and DTC genetic testing (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/gtmb).
Prospectively, physicians were subdivided (Supplementary Table S2) into primary care physicians, surgical specialists, internal medicine/pediatric specialists, and other specialists—from here forward referred to as PCPs, surgeons, specialists, and other specialists, respectively. Pediatric specialists were combined with internal medicine specialists due to low overall numbers within our hospital system; however, it was important to include these specialists as they potentially would have expertise in genomics.
All questions were formatted using a 5-point Likert-type rating scale except when addressing barriers to incorporating genomic medicine into practice, which used a 4-point scale.
This study was approved by the NorthShore University HealthSystem Institutional Review Board (EH11-016) before distributing the survey.
Statistics
InsightOut conducted statistical analyses using SurveyWriter (surveywriter.com) to compute standard two-tailed z-tests for proportions and paired independent Student's t-tests for means. Significance was considered at the 95% confidence interval (<0.05 p-value) when analyzing responses from subgroups.
Results
Response rate and demographics
Two hundred sixty surveys were completed for a response rate of 13% (260/2071). Graduation from medical school was reported up through 1990 by 163 (63%) and after 1990 by 97 (37%). Of the 260 respondents, 249 (96%) indicated involvement in direct patient care and 92 consider themselves to be PCPs (37%). When asked what they consider their primary affiliation, 33% indicated “primary care” (PCP), 18% “surgery” (surgeons), 18% “internal medicine/pediatric specialties” (specialists), and 31% “other specialties” (other).
Physician experience with GT
In the past year, 47% and 24% indicated that at least one patient had inquired about GT for complex disease and PT, respectively. More specialists and surgeons than PCPs saw “more than 10” patients in the past year who inquired about GT (13% and 14% vs. 2% respectively, p<0.05). More PCPs and specialists than surgeons had “1-5 patients” in the past year who inquired about PT (20% and 27% vs. 7% respectively, p<0.05). Forty-one percent (101/249) and 21% (52/249) of physicians had at least one patient in the last year who had GT and PT, respectively. Surgeons were more likely than PCPs to have seen “more than 10 patients” in the past year who had GT (11% vs. 1%, p<0.05), although there was no difference between specialties for PT. Twenty-one (8.4%) reported “currently using” GT and 28 (11.2%) specified “currently using” PT (Supplementary Table S3).
Twenty-six physicians (10%) had 1 to 5 patients who sought advice or interpretation of results from a DTC genomics test. Of these 26 physicians, 7 spent 5 min or less discussing or interpreting the results, 11 respondents spent 6-15 min, 7 individuals spent 16-30 min, and 1 physician spent more than 30 min in discussion. When asked if they had referred these patients to a genetics healthcare provider, 17 of 26 (66%) reported referring at least one patient.
Physician knowledge of genomics and GT
Given a 5-point Likert scale (from no to expert understanding), participants were asked to rate their knowledge surrounding “pharmacogenetics,” “genetics of complex diseases,” “Genome Wide Association Studies (GWAS),” “basic genetics principles,” and “when and how to incorporate genomic medicine into practice.” Overall, physicians were least confident in their knowledge surrounding “GWAS” (72% had no to minimal understanding) and reported themselves most knowledgeable about “basic genetics principles” (42% had above average to expert knowledge) (Fig. 1). When analyzing differences between physicians' specialties, PCPs were more uncertain regarding “when and how to incorporate genomic medicine into practice” than nonprimary care physicians (nPCPs) (61% vs. 50%; p<0.05). Specialists reported statistically higher mean understanding for all topics related to GT, GWAS, and PT (Table 1). Physicians with at least one patient who had undergone GT, PT, or both had a higher mean level of understanding for all knowledge areas surveyed (Table 1). One exception existed: there was no difference in the mean knowledge level of “basic genetic principles” for physicians who had at least one patient who had undergone PT versus physicians who had none. There was no difference in mean perceived knowledge of respondents based on graduation date.
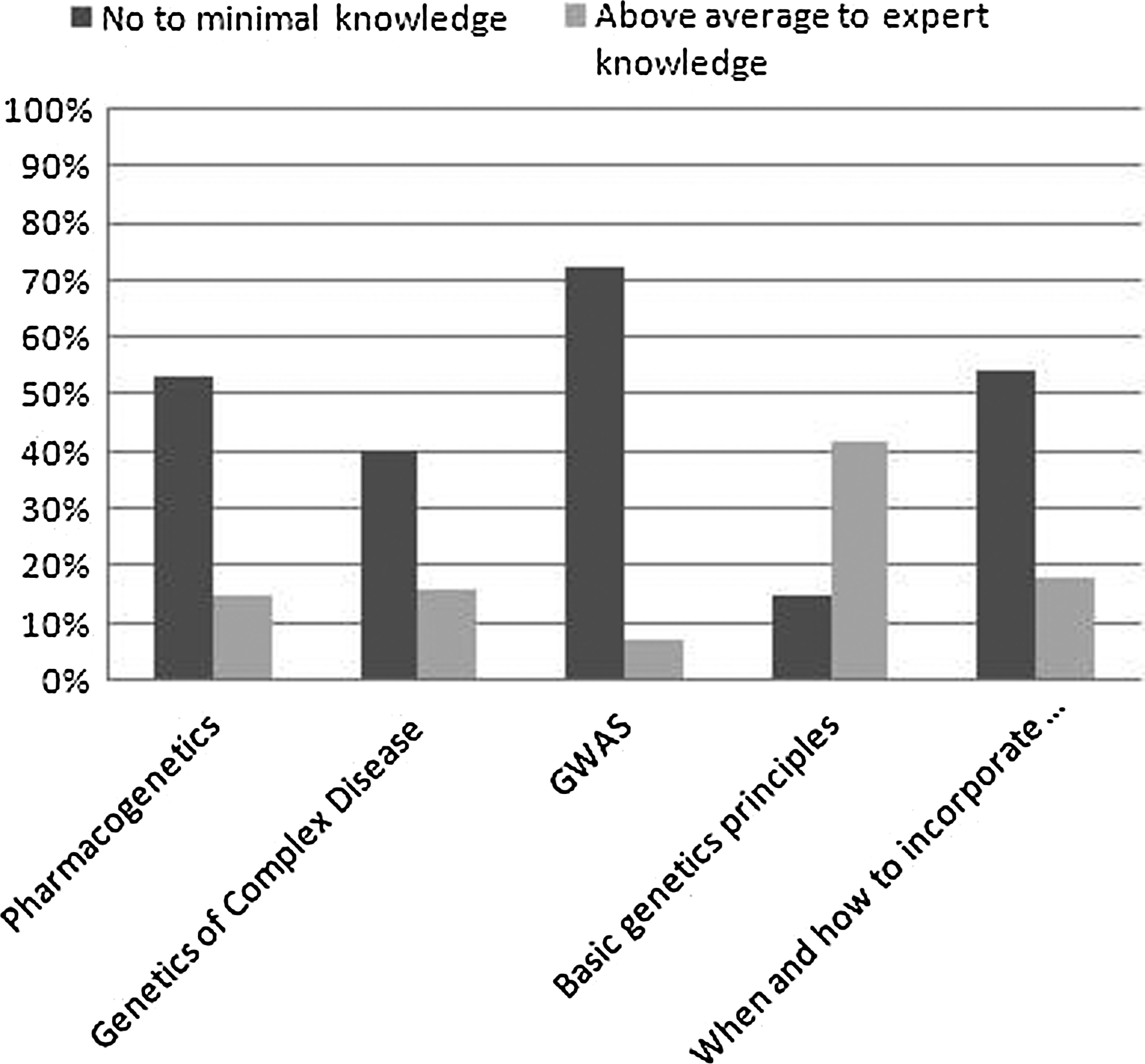
Physician-rated knowledge of genomic medicine. Physicians were asked to rate their understanding on a five-point scale, from no knowledge to expert knowledge, on the topics of pharmacogenetics; genetics of complex disease (coronary artery disease, diabetes, etc.); Genome Wide Association Studies (GWAS); basic genetic principles (Mendelian inheritance patterns, penetrance, anticipation, somatic vs. germline mutation); and when and how to incorporate genomic medicine into practice. Dark bars, no to minimal knowledge; light bars, above average to expert knowledge.
All bolded numbers are significantly different from the number on their left: 1+ patients versus no patients, p<0.05.
Letters a, b, and d represent significant differences between specialities, p<0.05.
GWAS, Genome Wide Association Studies; PCP, primary care physician.
Physician comfort level with GT
Participants were asked how comfortable they are with discussing the benefits and limitations of GT and with helping patients decide whether or not to pursue testing. Overall, more physicians reported being “not very to not at all comfortable” compared with those who reported being “extremely to very comfortable” (44% vs. 16%, p<0.05). More physicians who graduated medical school before 1990 were “very or extremely comfortable” compared to physicians who graduated after 1990 (21% vs. 9%, p<0.05) (Fig. 2). Physicians with one or more patients versus those with no patients who had GT were more comfortable with discussing benefits and limitations (23% vs. 11% indicated “extremely or very comfortable,” p<0.05; 23% vs. 59% indicated “not very to not at all comfortable,” p<0.05).
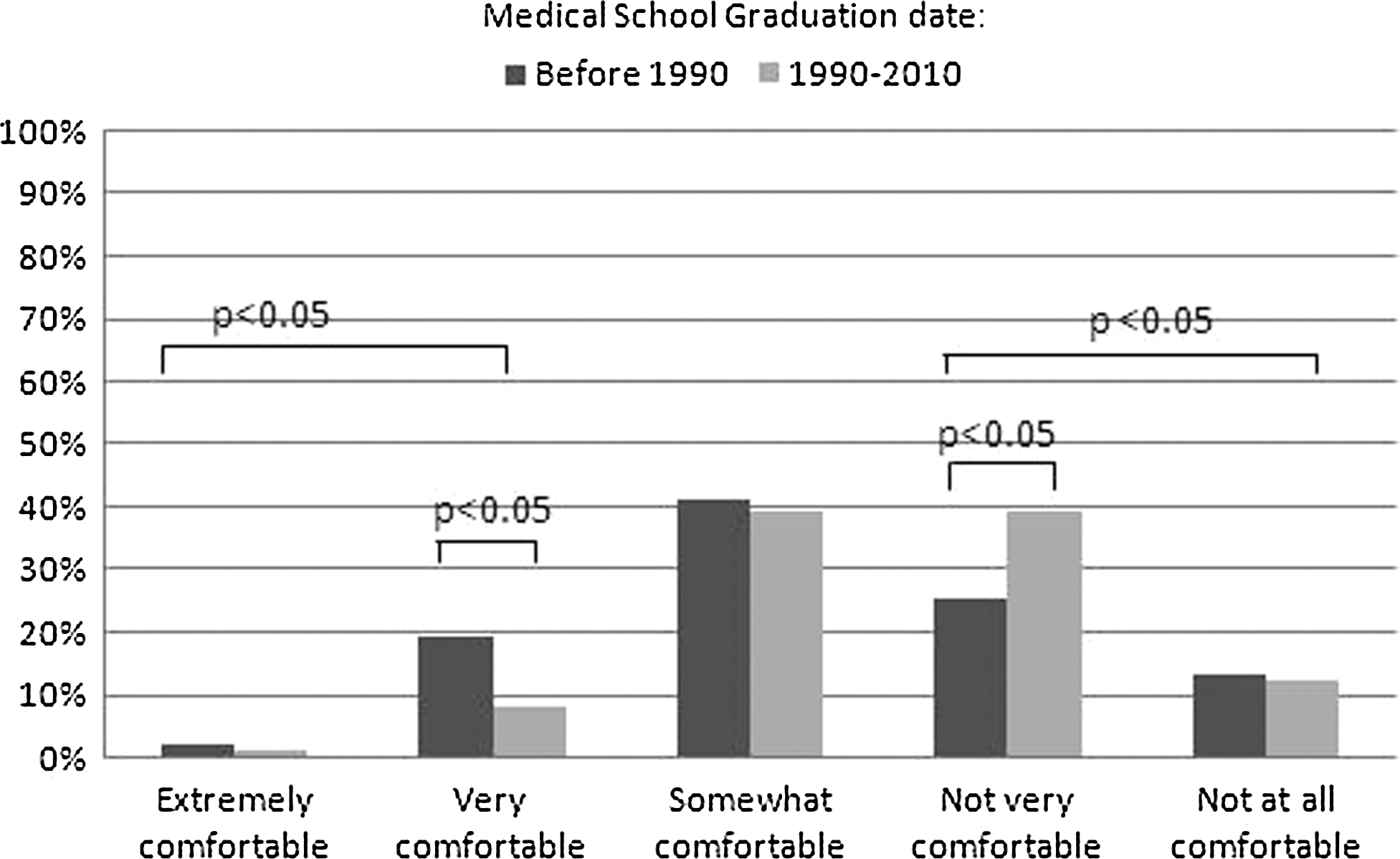
Physician comfort level with genomic testing. Participating physicians were asked how comfortable they are with discussing the benefits and limitations of genomic testing and with helping patients decide whether or not to pursue testing. Dark bars, respondents who graduated medical school before 1990; light bars, respondents who graduated medical school between 1990 and 2010.
Expectations for GT
When asked how soon they anticipated using GT/personal genome scans, most answered “1-2 years from now” for determining the risk of developing complex disease (31%) or prescribing medications (27%). The majority anticipated a “modest increase” over 5 years for number of patients seeking advice or incorporating GT (51%) and PT (42%) into medical care. No respondents thought frequency of use would decrease. Thirty-five percent (35/101) of physicians with at least one patient versus 16% (23/148) with no patients who had undergone GT expect a “significant increase” for incorporating GT into practice, p<0.05. Forty-six percent (24/52) versus 18% (36/197) of physicians with patients versus no patients who had undergone PT expect a “significant increase” for incorporating pharmacogenetic information into practice (p<0.05). More PCPs than nPCPs felt their patients would be “extremely likely” or “very likely” to share their GT results from a DTC company (62% versus 50%, respectively; p<0.05).
Barriers to incorporating genomic medicine into practice and educational resources
Overall, physicians (n=249) reported “lack of knowledge about genomic medicine”(73%) and “time required to keep up-to-date on the latest advances”(70%) as most significant barriers “greatly” or “somewhat” impacting their willingness and ability to incorporate genomic medicine into practice (Table 2). “Lack of knowledge about genomic medicine” was reported less as a barrier for physicians who had graduated before 1990 compared to those who graduated after 1990 (mean values 2.1 vs. 1.9, p<0.05).
Of all respondents (n=260), most utilized resources to stay informed about genomic medicine were “journal articles/reviews” (77%) and “continuing medical educational (CME) activities/meetings” (59%) (Supplementary Fig. S1). Sixty-four percent reported that CMEs keep them informed about advances “not very well” or “not well at all.” More PCPs thought their CMEs did “not very well” keeping them informed about genomics advances compared to nPCPs (60% vs. 36%, p<0.05). The most commonly reported resources used to answer a “genomic medicine” question were “genetics consult (formal or ‘curbside’)” (50%) and “online medical reference site” (48%). The majority was only “somewhat satisfied” with any resource used to answer a “genomic medicine” question, with the exception of “genetics consult,” which the majority of users were “very satisfied” (Supplementary Table S4). When asked what resources would be “extremely” or “very useful” in addressing educational needs related to advances in genomic medicine, most expressed interest in “customized electronic updates (email/web notices) related to their specialty” (64%); an institutional “website devoted to educational items (e.g., society guidelines, institutional guidelines, patient materials, etc.)” (54%); and “increased incorporation of genomic advances into grand rounds topics” (51%).
Discussion
The majority of physicians responding to the survey had no experience with GT or PT. Although GT use among physicians has not been reported, our sample reported a similar level of PT use and DTC testing compared to previous studies (Scheuner et al., 2008; Kolor et al., 2009; Stanek et al., 2009, 2012). We found surgeons and specialists more likely than PCPs to have patients with questions about and/or had undergone GT.
Our sample perceives that they lack sufficient knowledge for all genomics concepts presented. Studies have repeatedly found that PCPs are unprepared to incorporate basic genetic principles in clinical practice, citing lack of knowledge and confidence (Metcalfe et al., 2002; Carroll et al., 2003; Guttmacher et al., 2007); here we show that this deficiency extends to genomics. More PCPs in our sample versus specialists reported lower understanding of “when and how to incorporate genomic medicine.” Specialists reported significantly higher perceived knowledge than PCPs for most topics, consistent with previous reports (Hunter et al., 1998; Emery et al., 1999).
Our sample showed no difference in perceived knowledge based on graduation date although our survey did not include a test of actual knowledge or physician age. Surveys including tested knowledge of basic genetics show that more recent graduates have higher tested knowledge scores (Hofman et al., 1993; Wilkins-Haug et al., 2000b; Baars et al., 2005; Finn et al., 2005). We are unaware of a study that conducted a knowledge test of physicians for PT and GT; therefore, further research is needed to determine whether physicians' perceived knowledge is an accurate representation of actual knowledge of genomic medicine.
Previous studies have found that knowledge is based on experience (Hofman et al., 1993; Wilkins-Haug et al., 2000b; Metcalfe et al., 2002). Our sample showed higher perceived knowledge if physicians had at least one patient who had undergone GT or PT. The one exception was for understanding of “basic genetic principles,” alluding to the notion that knowledge of basic genetics is not sufficient to interpret and incorporate GT and/or PT into clinical care. General practitioners gain knowledge by contextual experiences (Metcalfe et al., 2002). PCPs in our sample have less experience seeing patients who had questions or had GT than specialists and/or surgeons. Our PCPs reported significantly lower levels of knowledge than specialists for most topics.
Physicians who graduated before 1990 or had seen at least one patient who had GT were more comfortable with discussing benefits and limitations, similar to past studies (Wilkins-Haug et al., 2000a, 2000b; Powell et al., 2011). Confidence in our sample appears to be related to experience or, perhaps, a refined ability to discuss areas of uncertainty given more experience with patients. However, overall, confidence in our sample is lacking. It has been suggested previously that perceived lack of knowledge about genetics leads to lack of self-confidence among physicians (Fry et al., 1999; Suther and Goodson, 2003; Guttmacher et al., 2007). Thus, the overall low confidence is likely related to the overall low knowledge that is evident regardless of graduation date.
Half our sample expects merely a “modest increase” of GT and PT in their practice over 5 years, while experts assume a more drastic increase for which PCPs and nongenetic specialists will extensively be involved in answering questions and/or doing testing (Emery and Hayflick, 2001; Guttmacher et al., 2007; Feero, 2008; Ginsburg, 2008; Avard and Knoppers, 2009; Drmanac, 2011; Houwink et al., 2011). Experience with GT or PT was associated with being more likely to expect a significant increase (47% and 24% respectively); however, those with experience represented a small percentage. Those without experience were less knowledgeable, less confident, and less likely to expect an increase in usage, leaving a large cohort that need to have focused education about the inevitable influx of genomics and pharmacogenetics, the benefits, and limitations.
Of 26 participants (10%) who had patients ask for advice or interpretation of DTC, most spent less than 15 min in discussion, although two-thirds of this group (17/26) indicated that they referred to a genetic professional. Our physician population, despite being provided a definition for DTC testing, may be considering tests with DTC marketing strategies (i.e., BRCA1 and BRCA2 testing in the United States) to be included in this category of DTC testing. Therefore, their reported referral practices may appear higher. Additionally, we did not provide a definition for “genetics healthcare provider”; therefore, each responder may have interpreted this differently when considering their referral practices.
More than half the physicians in our study thought it “very” or “extremely likely” that their patients would share DTC genomic results with them, when in actuality only 26.5% of patients report such results to their physicians (Bloss et al., 2011). This highlights a strong disconnect between physician perceptions regarding DTC testing and their patients' behaviors for sharing results. From the treating physician's vantage, this could be critical for the medical care of the patient and potential medical-liability (Frueh, 2011). Physicians need to ask their patients if they had GT and PT performed since they cannot assume patients will share this information without direct questioning. Naturally, this could be tailored to the specific scenario in which a clinician is seeing the patient. For example, a cardiologist may focus on PT for clopidogrel and GT related to cardiovascular risk. Additional research addressing communication of GT results between patients and their physicians is needed.
A large systematic review determined that many barriers exist preventing genomic medicine from entering into practice and guiding management of chronic adult diseases (Scheuner et al., 2008). The most common obstacles were “lack of sufficient knowledge and confidence relating to provision of genetic service.” Similarly, our population listed “lack of knowledge about genomic medicine” as most influential, more so for recent graduates. Recent graduates report their knowledge and comfort level as inadequate for using genomic medicine in practice. It is possible that recent graduates are more keenly aware of the extent of knowledge they do not know and therefore are less comfortable with providing genomic services, given that recent graduates show higher genetic knowledge levels when tested (Wilkins-Haug et al., 2000a; Metcalfe et al., 2002; Baars et al., 2005; Houwink et al., 2011).
For 81% of PCPs in our study, “time required to keep up-to-date on the latest advances” was the most significant barrier to incorporate genomic medicine into practice. Currently, 60% of PCPs report their CME activities to keep them up-to-date on genomic advances “not very well.” We do not know whether participants were referring to general primary care-related CME activities, which contain varying amounts of genomic information, versus genomic-specific CMEs as it relates to their clinical practice. It is important for CME activity providers to both assess participant satisfaction in the quality of CMEs targeted toward GT as it relates to clinical practice as well as to determine whether genomic-based topics should be incorporated into broader CME opportunities. Furthermore, given the greater lack of experience and perceived knowledge reported by PCPs in our sample and previous studies, PCPs may benefit more from focused educational resources (Emery et al., 1999). Finding ways to incorporate education into physicians' already busy schedules will need to be accounted for in any educational program developed.
Physician education requires innovative approaches (Emery and Hayflick, 2001; Guttmacher et al., 2007; Avard and Knoppers, 2009). Our sample suggests using technology such as “customized electronic updates (via email/web notices)” or an “institutional website devoted to educational items” to overcome knowledge deficiencies. Others suggest utilizing technology with electronic medical record delivery of genetic information, increasing accessibility to the Internet in clinic, and electronic decision support systems for PCPs; such systems are in development (Guttmacher et al., 2007). Medical schools need to continue to enhance curriculum in genetics and genomics to increase the physician comfort level (Guttmacher et al., 2007). Recently, Ormond et al. (2011) tested a strategy where medical students participated in genotyping services by a DTC company, concluding that the program was successful at educating students regarding limitations and utility of DTC testing. It is possible that such innovative educational strategies are needed for medical students and practicing physicians alike.
Although our response rate is comparative to other surveys of physician populations, the results may not be generalizable to physicians outside of a community-based health system (Stanek et al., 2009, 2012; Powell et al., 2011; Haga et al., 2012). We have elicited physicians' self-reported perceived knowledge, not actual tested knowledge, which has been shown to elicit different results in the area of basic genetic knowledge (Hofman et al., 1993; Wilkins-Haug et al., 2000b; Baars et al., 2005; Finn et al., 2005). However, no studies to date have provided this information for genomic medicine and PT. We do not know how responders differ from nonresponders of our survey. Possibly, those who did not respond have no knowledge or experience with genomics, and therefore ignored the invitations to our survey. If so, the knowledge and confidence levels for GT and PT in our population may be even more insufficient than are evidenced here.
To our knowledge, this is the first study to assess physician preparedness for incorporating genomic medicine and PT into clinical practice. While previous research has assessed physician knowledge of genetic medicine, which we would define as the use of knowledge regarding single-gene disorders (Metcalfe et al., 2002; Baars et al., 2005; Houwink et al., 2011), here we focus on genomic medicine—that is, the practice of medicine related to multigenic conditions as well as the incorporation of technology that enables the interrogation of large amounts of genomic data to provide important pharmacogenetic information and to improve risk assessment for complex disease. With the advent of whole genome and whole exome sequencing moving from the laboratory to the clinic and the shifting paradigm of single-gene testing to more complex assessment of the genome, it is important to begin assessing physician knowledge and readiness for this new wave of genomic technology. Overall, our sample appears underprepared, perceiving that they lack sufficient knowledge and self-confidence. Physicians who already had experience with patients asking questions or having testing for genomics of complex disease or PT were more confident and perceived their knowledge to be higher than physicians with no experience.
The majority of our sample expects their role in genomic medicine and pharmacogenetics to increase. For successful integration, educational programs and decision support tools will need to be developed to assist PCPs and nongenetic specialists to increase knowledge and confidence. Certain specialties may only need a subset of knowledge for PT in their practice, and it will be important to identify those tests that are relevant for their practice. PCPs, however, could potentially field questions across the spectrum of pharmacogenetics and genomics and thus will need to be prepared appropriately. Increasing access to educational programs and decision support tools, expanding the evidence base for use of genomics and pharmacogenetics, and working toward better reimbursement for these services will be imperative for implementation of genomic information in the clinic.
Footnotes
Acknowledgments
This study was funded by a NorthShore University HealthSystem Research Career Development Award awarded to Dr. Hulick, with additional support provided by the Department of Medicine. We would like to thank Dr. Janardan Khandekar for his assistance with our research.
Author Disclosure Statement
Mr. Weissman has received two honoraria from Myriad Genetics Laboratory. Dr. Hulick, Dr. Anderson, and Ms. Selkirk declare no potential conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.