
Abstract
Genetic testing of myotonic dystrophy type 1 (DM1) is very important because it enables the diagnosis and indicates the severity of the disease. Mutation analysis is based on the detection of the number of CTG triplets in the 3′ untranslated region of the myotonic dystrophy protein kinase (DMPK) gene. Sometimes it could be complicated by the presence of different patterns of repeat interruptions in the 5′ and 3′ ends of the expanded alleles recently described in about 3% to 5% of patients. To make molecular diagnosis easier and faster, the use of triplet-primed PCR (TP-PCR) for the detection of expansions in DM1 and other dynamic mutation diseases was proposed. Here we present the results of a retrospective study performed by TP-PCR on 100 subjects previously analyzed by Southern blotting-long PCR.
Introduction
Materials and Methods
Study subjects
We retrospectively analyzed 100 DNA samples belonging to Sardinian subjects referred to our laboratory as clinically suspected DM patients and DM1 relatives. Signed informed consent was obtained from all the subjects.
Genotyping
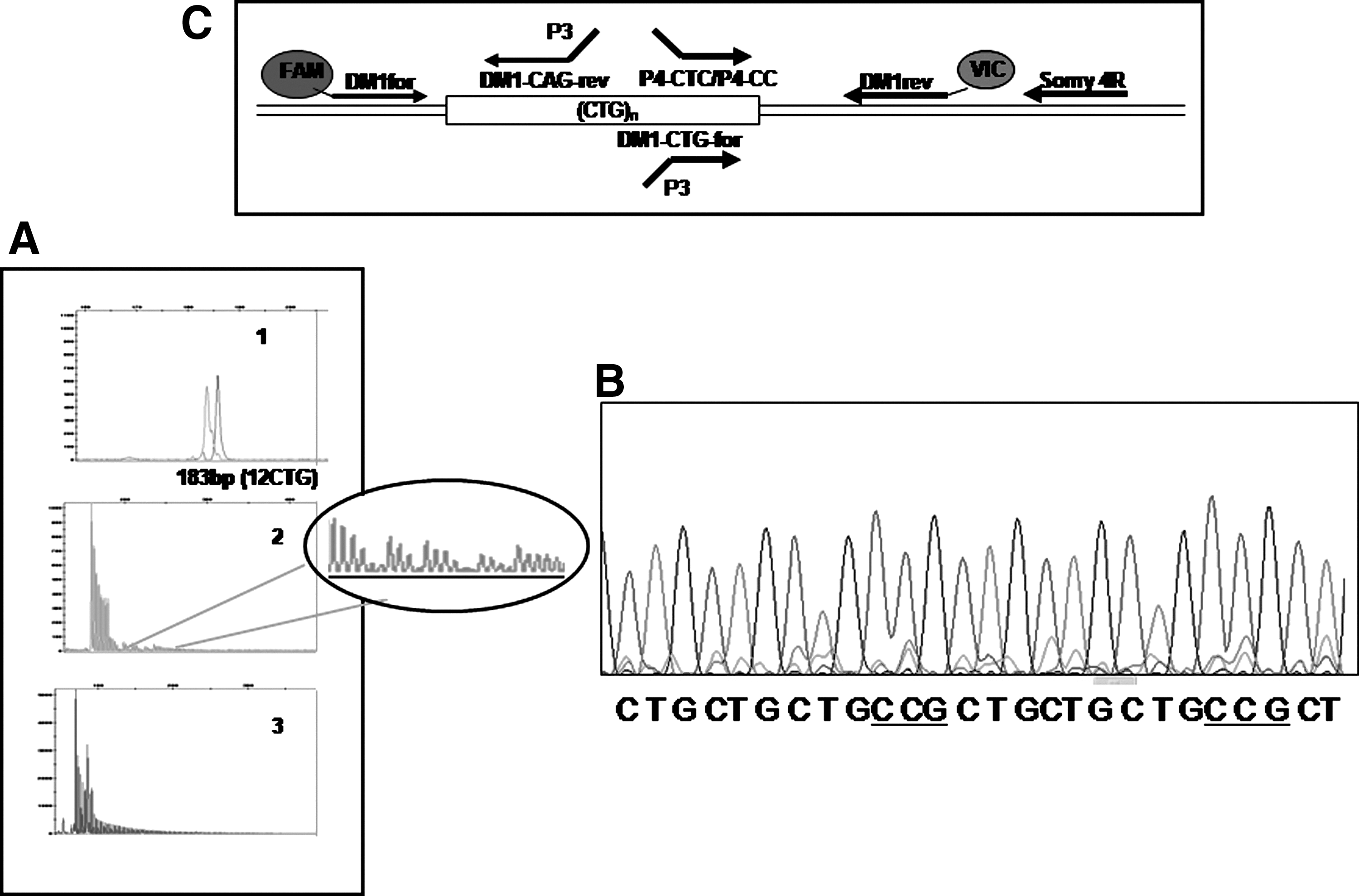
All DNA samples were previously analyzed with long PCR. The samples showing only one allele underwent to blotting followed by hybridization with (CTG)5 γATP labeled probe (Gennarelli et al., 1998). Successively, all 100 samples were analyzed using three different PCRs: conventional PCR using primers DM1for-FAM/DM1rev-VIC and two TP-PCRs performed in both directions according to Radvansky et al. (2011a, 2011b) using primers DM1-CTG-for/DM1-rev/P3, and DM1-for/DM1-CAG-rev/P3 (Fig. 1C) (Table 1). PCR products were separated on an ABI PRISM 3130 XL, and the data were analyzed using GeneMapper 3.7 software (Life Technologies). The same forward and reverse TP-PCR products in one patient (AB) were subjected to blotting followed by hybridization with (CTG)5γATP labeled probe (Southern blotting). The TP-PCRs were performed using P4-CC and P4-CTC as forward primers and Somy 4R as the reverse primer (Table 1).
Sequencing
The TP-PCR products obtained by the use of P4-CC as forward primer and Somy 4R as reverse primer and TP-PCR product obtained with DM1for and DM1-CAG rev primers were sequenced using primer Somy4R and DM1-CAG-rev, respectively (Table 1) (Life Technologies) (Musova et al., 2009).
Results
Using the long PCR method followed by hybridization with (CTG)5 γATP-labeled probe, 54 samples out of 100 showed two fragments corresponding to normal alleles; the remaining 46 showed one fragment corresponding to the normal allele and one expanded fragment corresponding to the mutated allele. Utilizing the approach based on one conventional PCR and two bidirectional TP-PCRs in the same samples, we found that the results were concordant for 99 samples. A pattern of interruption was present in one DM1 sample (AA) (Fig. 1A). TP-PCR using primers DM1-CTG for and Somy4R, followed by sequencing with primer Somy4R, revealed a CCG interruption in the stretch of CTG in an AA patient (Fig. 1B).
One DNA sample (AB) belonging to an asymptomatic patient gave discordant results when reverse TP-PCR was performed. As shown in Figure 2A, with long PCR a single fragment in the normal range was detected (lane 1). Again, using conventional PCR, only one 160-bp fragment corresponding to a 4CTG allele was detected. The expanded fragment was not revealed by the forward TP-PCR, but only by reverse TP-PCR (Fig. 2B) even after Southern blotting as shown in Figure 2C. Sequencing analysis of TP-PCR products obtained with primers DM1-for and DM1-CAG-rev revealed a stretch of >70 CTG in patient AB. No TP-PCR products were obtained when P4-CTC and P4-CC were used as forward primers and Somy 4R as the reverse primer (Table 1).
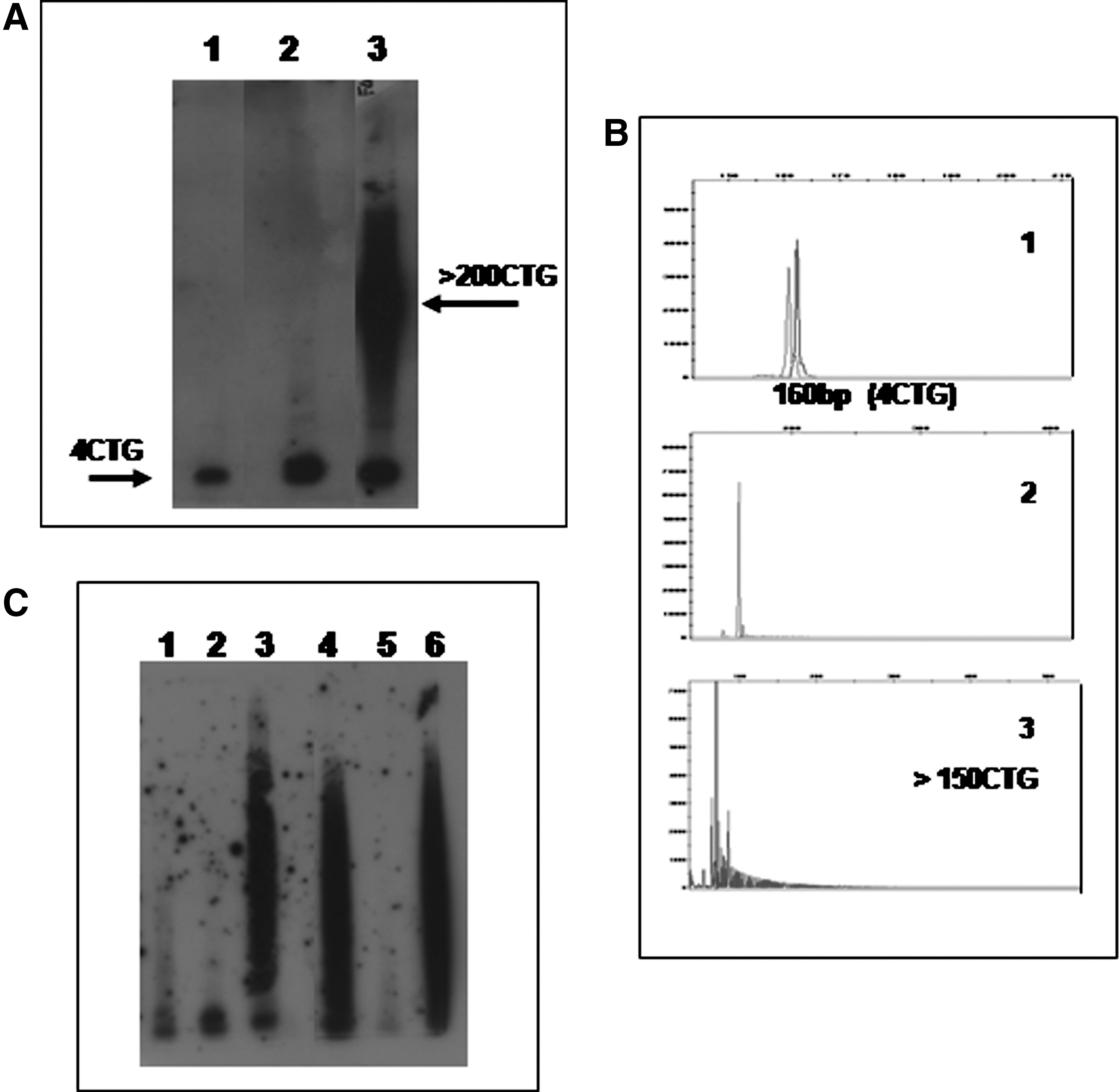
Analysis of DMPK repeat in patient AB.
Discussion
Diagnostic testing of molecular pathologies due to dynamic mutations with possible large expansions, such as DM1, has been always troublesome. The reference method for DM1 has been long-range PCR followed by blotting and hybridization with radiolabeled probe to identify expansions up to 2500-3000 repeats (Gennarelli et al., 1998). This method is time-consuming and requires radioactive material, and sometimes amplification of large expansions could fail. The use of conventional PCR DM1for/DM1rev and TP-PCR has allowed these problems to be overcome, to rapidly detect large CTG expansions, and to exactly size the normal and premutated alleles. Radvansky et al. (2011b) suggested the need to perform TP-PCR in both directions to avoid false-negative results due to the presence of interruptions located in the 3′ end of CTG stretch. The DM1 locus was considered a pure CTG repeats on the basis of the sequencing of small alleles and small expanded alleles with the exception of one interrupted DMPK allele in a sperm donor described by Leeflang and Arnheim (1995). Only recently, it has been shown that interruptions in the CTG-expanded allele are quite frequent having been found in 3%-4% of French DM1 (Braida et al., 2010) and in 5% of Czech DM1 (Musova et al., 2009) and to have important consequences for molecular diagnosis of DM1 because they can give false-negative results. In our population, 1 out of 46 DM1 patients (∼2%) showed a CCG interruption.
In this study TP-PCR in both directions confirmed the diagnosis in 46 DM1 subjects and in 53 out of 54 samples previously found to be normal. One subject did not show any CTG expansion by using both long PCR followed by blotting and hybridization and by TP-PCR using DM1-CTGfor (Kakourou et al., 2010). Only when TP-PCR using DM1-CAG-rev was performed, an expanded fragment was obtained. TP-PCR carried out with primers P4-CTC and P4-CC (Musova et al., 2009) failed to detect the most common CCG and CTC interruptions. By these data AB, previously diagnosed as normal, was shown to contain an expanded CTG allele. The false-negative result obtained by long PCR could be explained by interruptions other than CCG and CTC, a repeat-flanking deletion, and an insertion of non-CTG sequences as recently described by Axford et al. (2011) in UR-ADM9 patient's tissues. In conclusion, the bidirectional TP-PCR assay in combination with conventional PCR seems to be sufficient to correctly establish the presence or absence of DM1-expanded alleles and more effective than long PCR followed by blotting and hybridization.
Footnotes
Acknowledgments
This work was supported by a grant of Regione Autonoma della Sardegna LR11 1990.
Author Disclosure Statement
No competing financial interests exist.