
Abstract
Objective: The aim of this study was to determine whether the CNDP1 (carnosinase gene) D18S880 microsatellite polymorphism confers susceptibility to diabetic nephropathy (DN). Methods: The authors conducted meta-analysis on association between the CNDP1 D18S880 microsatellite polymorphism and DN susceptibility, using fixed and random effects models. Results: A total of nine comparative studies were included in this meta-analysis, which included 4546 DN, 7994 diabetes mellitus (DM), and 1826 healthy (Heal) subjects. Overall, the analysis revealed that the D18S880 microsatellite polymorphism was significantly associated with DN for the five trinucleotide repeat (5L) allele and five leucines repeat (5L-5L) homozygous in the comparisons of DN versus DM (5L: odds ratio [OR] 0.90, 95% confidence interval [CI] 0.84-0.97, p=0.008; 5L-5L: OR 0.88, 95% CI 0.81-0.97, p=0.006) and DN versus non-DN (DM+Heal) (5L: OR 0.92, 95% CI 0.86-0.98, p=0.009; 5L-5L: OR 0.89, 95% CI 0.82-0.96, p=0.004). The protective effects of the D18S880 polymorphism were similar to those observed in the subgroups of the type 2 DM and the Caucasian population. However, significant association was not found in the type 1 DM population. Conclusions: This meta-analysis confirms that the carnosinase D18S880 microsatellite polymorphism is associated with DN susceptibility, especially in the type 2 DM and the Caucasian population.
Introduction
A family study conducted in 18 Turkish extended families exhibiting type 2 DM showed evidence for linkage between microalbuminuria and proteinuria and the genomic region on chromosome 18q22.3-q23 (Vardarli et al., 2002). The locus was supported by a highly significant logarithm of odds score of 6.1. Linkage of DN to 18q was confirmed by an affected sib-pair analysis performed on Pima Indians and by a large sib-pair analysis of African Americans (Vardarli et al., 2002; Bowden et al., 2004). Following these findings, an association was found between DN and the D18S880 microsatellite, located in the carnosinase-1 gene (CNDP1) on chromosome 18q (Janssen et al., 2005). Alleles of this microsatellite encode for a variable number of leucine residues (from 4 to 8) in the leader peptide of the carnosinase precursor, whereas the 4L and 8L repeats are rare (<0.005%) (Ahluwalia et al., 2011). And subjects with diabetes, but without DN were more frequently homozygous for the five leucines repeat (5L-5L) genotype than those who had ESRD (Freedman et al., 2007). Both studies concluded that the five trinucleotide repeat (5L) allele was protecting against DN (Freedman et al., 2007; Ahluwalia et al., 2011). Although the D18S880 microsatellite was not associated with ESRD in an African American population under both the allelic and genotypic models, the results of stratified analysis showed that protection from DN afforded by 5L-5L homozygosity in the D18S880 microsatellite may be masked by the effects of additional risk haplotypes in CNDP1 and CNDP2 (McDonough et al., 2009). Likely, protection for DN of 5L-5L homozygosity was sex specific, the genotype risk for the population was estimated to be 0.5 (0.30-0.68) in women and 1.2 (0.77-1.69) in men (Mooyaart et al., 2010). However, several studies have not found any association between the D18S880 microsatellite and DN in DM (Wanic et al., 2008; Craig et al., 2009; Alkhalaf et al., 2010; Ahluwalia et al., 2011).
This inconsistency may be due to inadequate statistical power, racial and ethnic difference, type of DM, and publication bias. Meta-analysis is a powerful tool for summarizing the results from different studies by producing a single estimate of the major effect with enhanced precision. The aim of this meta-analysis was to assess the pooled effect between the CNDP1 D18S880 microsatellite polymorphism and DN.
Materials and Methods
Identification of eligible studies
We performed an exhaustive search for studies that examined the association of the CNDP1 D18S880 microsatellite polymorphism with DN. Available articles were identified through a literature search using the keywords “carnosinase” or “CNDP1” and “diabetic nephropathy” in the PubMed, MedLine and CNKI (Chinese National Knowledge Infrastructure) database. For these two concepts, all relevant keyword variations were used. The process was performed three times to ensure that no references were omitted. Meanwhile, additional literature was collected from cross references within both original and review articles. We only recruited data from fully published articles, not any meeting or conference abstracts. No language restrictions were applied.
Inclusion and exclusion criteria
A study was included in the present meta-analysis if (1) it was published up to July 2012; (2) it was a case-control study; (3) it made the allele frequency or genotype distribution data available; (4) DN patients had to have DM with microalbuminuria or macroalbuminuria or ESRD. A study would be excluded if family members had been studied, because the analysis is based on linkage considerations. When a study reported results on different subpopulations, we treated each subpopulation as a separate comparison in the meta-analysis.
Data extraction
Two investigators independently extracted the data with a standard protocol and the result was reviewed by a third investigator. Discrepancies were resolved by discussion with our research team. From each study, we extracted the first author's name, the year of publication, the source of publication, racial ancestry, the number of cases (DN defined as microalbuminuria/macroalbuminuria/proteinuria or ESRD) and controls (DM and/or nondiabetic participants) and the available genotype and allele frequency information from the D18S880 microsatellite polymorphism.
Statistical analysis
Allele frequencies at the CNDP1 D18S880 microsatellite polymorphism from the respective study were determined by the allele counting method. We examined the relationships between the 5L allele/5L-5L genotype and susceptibility to DN (DN vs. DM and DN vs. non-DN [(DM plus healthy subjects]). The point estimates of the risk, the odds ratio (OR), and its 95% confidence interval (95% CI) were estimated for each study. The between-study heterogeneity was assessed by the Chi-square test-based Q-statistic (Cochran, 1954). A significant Q-statistic (p<0.10) indicated heterogeneity across studies, and then the result of the random effect model was selected. Otherwise, the result of the fixed effect model was selected. We also measured the effect of heterogeneity by another measure, I2=100%×(Q−df)/Q (Higgins and Thompson, 2002). Finally, the pooled OR was obtained by the Mantel-Haenszel method in the fixed effect model and by the DerSimonian-Laird method in the random effect model (Mantel and Haenszel, 1959; DerSimonian and Laird, 1986). The pooled OR was performed weighting individual OR by the inverse of their variance, and the significance of the pooled OR was determined by the Z-test.
Publication bias is well known to compromise the validity of the meta-analysis, because negative or uninteresting results are less likely to be published. To assess the publication bias, we evaluated the study quality using a funnel plot. The funnel plot should be asymmetric when there is a publication bias and symmetric in the case of no publication bias. Since the funnel plot approach is limited by the requirement for a range of studies with varying size, we employed the Egger's linear regression test (Egger et al., 1997). The Egger's test measures the funnel plot asymmetry on the natural logarithm scale of OR.
Statistical analyses were performed using the software STATA version 7 (Stata Corp LP, College Station, TX). All the p-values were two sided. p<0.05 was considered statistically significant.
Results
Characteristics of studies
Characteristics of studies included in the current meta-analysis are presented in Table 1 (Janssen et al., 2005; Freedman et al., 2007; Wanic et al., 2008; Craig et al., 2009; McDonough et al., 2009; Alkhalaf et al., 2010; Mooyaart et al., 2010; Ahluwalia et al., 2011). There were 91 articles relevant to the searching words (Fig. 1). Through the step of screening the abstract, 59 of these articles were excluded (6 were review; 1 was a family-based study; 15 were not conducted in humans; 36 were not performed in diabetic nephropathies; 1 was not a case-control study), leaving 32 studies for full publication review. Of these, 24 were excluded (22 did not explore the D18S880 microsatellite polymorphism and DN susceptibility; 2 did not make the allele frequency or genotype distribution data available). However, one of the eligible studies contained data in two different types of DM (Janssen et al., 2005). Therefore, nine studies were analyzed independently in this meta-analysis. A total of 4546 DN, 7994 DM, and 1826 healthy subjects were investigated, including 8 Caucasian and 1 African American, 4 type 1 and 5 type 2 DM. Two studies had only genotype frequency data for the D18S880 microsatellite but no allele data were available (Alkhalaf et al., 2010; Mooyaart et al., 2010). The frequencies for the allele as well as the genotype of the D18S880 microsatellite polymorphism were extracted from 7 and 9 of the eligible studies, respectively.
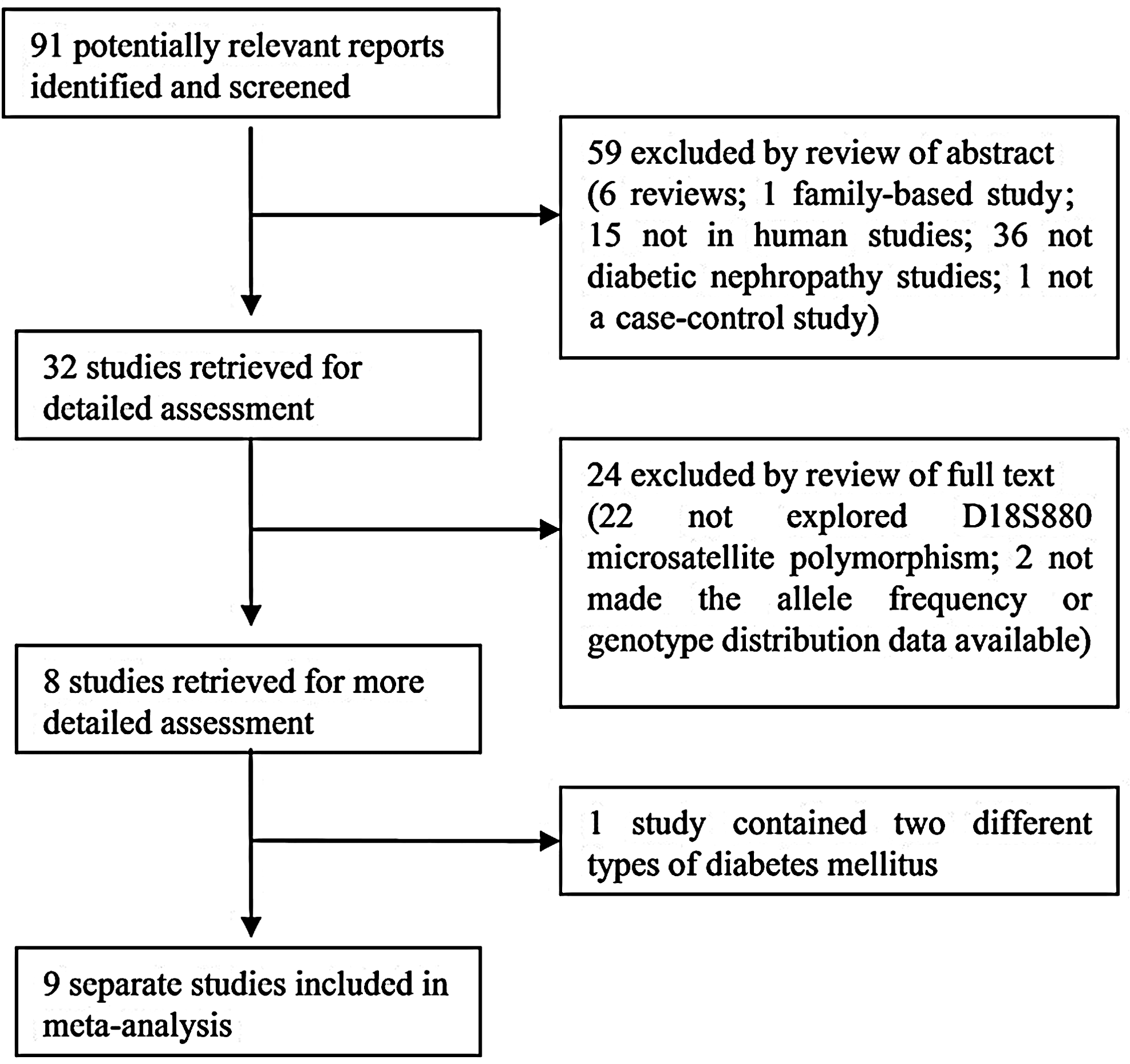
The flow diagram of the study selection process.
-, no data; NA, not available; DN, diabetic nephropathy; DM, diabetes mellitus; Heal, healthy subject; 5L, five trinucleotide repeat; 5L-5L, five leucines repeat.
Meta-analysis
Meta-analysis was performed on the overall population and stratified based on the different type of diabetic groups. A summary of the meta-analysis is in Table 2. The Q-test of heterogeneity was not significant and we conducted analyses using fixed effect models in the overall population. Overall, the 5L allele of the CNDP1 D18S880 microsatellite was significantly associated with diabetic nephropathy (DN vs. DM: OR 0.90, 95% CI 0.84-0.97, p=0.008; DN vs. non-DN: OR 0.92, 95% CI 0.86-0.98, p=0.009). The results of 5L-5L homozygosity were similar to 5L (DN vs. DM: OR 0.88, 95% CI 0.81-0.97, p=0.006; DN vs. non-DN: OR 0.89, 95% CI 0.82-0.96, p=0.004). The forest plots of positive results are shown in Figure 2.
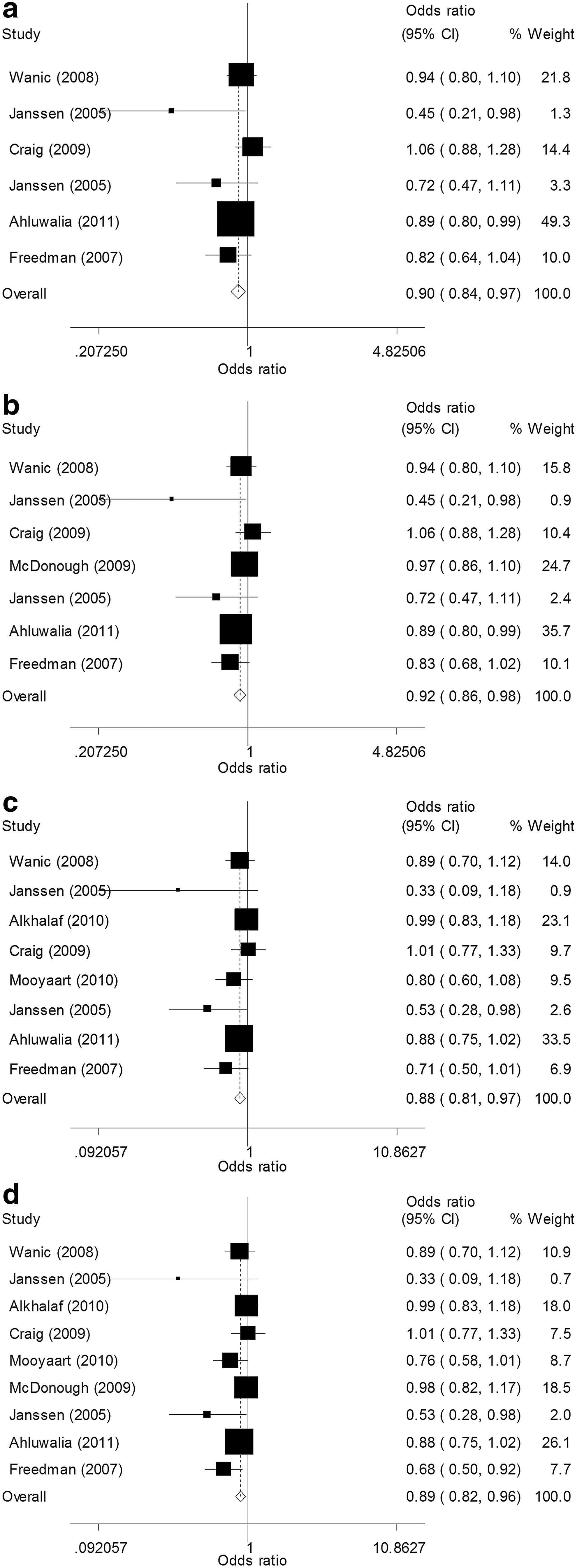
Forest plots for meta-analysis of positive results in the overall population.
non-DN, DM and healthy subjects; OR, odds ratio; CI, confidence interval; R, random effects model; F, fixed effects model.
We have performed group-specific meta-analysis in the type 1, type 2 DM, and the Caucasian population. The Q-test of heterogeneity was not significant except for type 1 DM, so we conducted analyses using the random effect models in the type 1 DM population, and fixed effect models in the type 2 DM and the Caucasian population. The D18S880 polymorphism was associated with DN in type 2 DM, for 5L (DN vs. DM: OR 0.87, 95% CI 0.79-0.95, p=0.003; DN vs. non-DN: OR 0.90, 95% CI 0.84-0.97, p=0.006), for 5L-5L (DN vs. DM: OR 0.82, 95% CI 0.73-0.93, p=0.002; DN vs. non-DN: OR 0.86, 95% CI 0.77-0.95, p=0.002) and in the Caucasian for 5L (DN vs. DM: same to overall; DN vs. non-DN: OR 0.90, 95% CI 0.84-0.97, p=0.006), for 5L-5L (DN vs. DM: same to overall; DN vs. non-DN: OR 0.87, 95% CI 0.80-0.95, p=0.002).
Funnel plot asymmetry was assessed by the method of the Egger's linear regression test. If there is asymmetry, then the regression line will not run through the origin. The results of the Egger's linear regression test are shown in Table 3. It was shown that there was no publication bias for the 5L allele except for the comparisons of DN versus DM in type 2 DM, and publication bias was found for the 5L-5L genotype except for DN versus DM in type 1 DM, DN versus non-DN in type 1 and type 2 DM.
non-DN, DM, and healthy subjects.
Discussion
Genetic factors play an important role in the development of DN, which is one of the most severe complications of DM (Quinn et al., 1996; Pei et al., 2010; Yu et al., 2012). Carnosine, β-alanyl-L-histidine, the substrate of the enzyme encoded by the CNDP1 gene, has been reported to have a natural ACE-inhibitor activity (Hipkiss, 1998; Hou et al., 2003), serve as an oxygen free radical scavenger (Boldyrev et al., 2004), cleave advanced glycation end products (Hipkiss et al., 2002), protect renal cells against the deleterious effects of high glucose levels, and reduce the development of DN (Masson et al., 2005).
The CNDP1 D18S880 microsatellite polymorphism lies in the 5′ coding part of the transcript, the number of trinucleotide repeats is directly related to the number of leucine residues in the leader peptide of the carnosinase precursor: five, six, or seven leucines (Wanic et al., 2008). Individuals homozygous for the five leucine repeat allele have reduced serum carnosinase concentrations (Janssen et al., 2005; Riedl et al., 2007). This is expected to result in higher renal concentrations of the protective dipeptide carnosine. Many studies have been conducted to test the association of the CNDP1 D18S880 microsatellite polymorphism with DN, but the studies reported conflicting results (Janssen et al., 2005; Freedman et al., 2007; Wanic et al., 2008; Craig et al., 2009; McDonough et al., 2009; Alkhalaf et al., 2010; Mooyaart et al., 2010; Ahluwalia et al., 2011). It is necessary to perform a comprehensive meta-analysis to assess the importance of the D18S880 microsatellite polymorphism for DN susceptibility.
In this study, we retrieved nine studies that included 4546 DN, 7994 DM, and 1826 healthy subjects to evaluate the association of the D18S880 microsatellite polymorphism with DN. Our meta-analysis detected a significant genetic association of the D18S880 microsatellite polymorphism with DN, and 5L-5L was a protective genotype for susceptibility of DN, especially in the type 2 DM and the Caucasian population. Our meta-analysis results also showed that 5L was a protective allele for susceptibility of DN in the type 2 DM and the Caucasian population.
In our study, we found that the CNDP1 D18S880 microsatellite 5L-5L genotype reduced the risk of DN, especially in the type 2 DM and the Caucasian population, a lower 5L allele frequency of the D18S880 microsatellite may increase the susceptibility of DN in the type 2 DM and the Caucasian population. However, no significant genetic association of the D18S880 microsatellite polymorphism with DN was found in the type 1 DM population. This difference might be due to genetic heterogeneity or ethnic influences. In addition, studies with a small sample size may have insufficient statistical power to explore a slight effect or may have generated a fluctuated risk estimate. Considering the limited studies included in the meta-analysis, our results should be interpreted with caution.
Some limitations of this study should be discussed. First, cases (DN) and controls (DM only or DM plus healthy subjects) in these studies contributing to this meta-analysis were not age- and sex-matched. Second, significant between-study heterogeneity was detected in two comparisons (5L: DN vs. DM/DN vs. non-DN). But it was not a major problem, because DN itself is heterogeneous. Third, publication bias was detected for the 5L allele in the contrast of DN versus DM in type 2 DM, and for the 5L-5L genotype except for DN versus DM in type 1 DM, DN versus non-DN in type 1 and type 2 DM. Thus, some publication bias may distort the meta-analysis. Finally, meta-analysis remains a retrospective research that is subject to the methodological deficiencies of the included studies. We minimized the likelihood of bias by developing a detailed protocol before initiating the study, by performing a meticulous search for published studies, and by using explicit methods for study selection, data extraction, and data analysis.
In conclusion, we provide evidence of an association between the CNDP1 D18S880 microsatellite polymorphism and DN, especially in the type 2 DM and the Caucasian population. The identification of the DN susceptibility variant can lead to novel biological insights and improved measures of individual aetiological processes. The genetic association between CNDP1 Mannheim with protection from DN shed light on a novel and potentially important pathway in the development of DN. To reach a definitive conclusion, further gene-gene and gene-environment interaction studies based on a larger sample size, a case-control design, and stratification by ethnicity are still needed.
Footnotes
Acknowledgments
Financial support: This work was partly supported by grants from the National Natural Science Foundation of China (81102192, 30901255) and the Anhui Provincial Postdoctoral Science Foundation (2009-9).
Author Disclosure Statement
No competing financial interests exist.