
Abstract
SF3B1, located on chromosome 2q33.1, encodes a core component of RNA-splicing machinery, and its mutation has been described in myelodysplastic syndromes (MDS) characterized with ring sideroblasts (RS). To explore the reliability and sensitivity of the high-resolution melting analysis (HRMA) technique for the identification of the SF3B1 mutations, mutations in 92 patients with MDS were detected in this study. The sensitivity could reach 5%, obviously higher than the 25% of direct DNA sequencing. A low frequency (5.4%) of SF3B1 mutations were identified in patients with MDS, including three cases of K700E, one case of H662Q, and one case of K666M. Further, SF3B1 mutations were more frequently recurrent in the 33% of patients with MDS characterized with RS, whereas in other subtypes of MDS, only 2.3% of patients were detected with SF3B1 mutations (p=0.006). In conclusion, a rapid, reproducible, sensitive, and high-throughput HRMA assay has been established for the scanning of SF3B1 mutations.
Introduction
The RNA-splicing system plays an important role in the maintenance of the protein diversity through alternative splicing in the face of a limited number of genes (Pajares et al., 2007; David and Manley, 2010). Aberrant RNA splicing has been identified in a wide variety of cancers (Pajares et al., 2007; David and Manley, 2010). The disruption of interactions of several factors involved in the splicing process can cause various types of mutations in an ever-increasing number of genes (Baralle and Baralle, 2005). SF3B1, one subunit of the splicing factor 3b protein complex, can anchor the U2 small nuclear ribonucleoproteins complex (U2 snRNP) to the pre-mRNA in the process of RNA splicing (Gozani et al., 1998). Recently, SF3B1 mutations have been identified in MDS with an intriguingly high frequency in the subtypes with ring sideroblasts (RS) (Malcovati et al., 2011; Papaemmanuil et al., 2011; Yoshida et al., 2011; Damm et al., 2012b; Patnaik et al., 2012; Visconte et al., 2012). Although the pathological role of SF3B1 mutations in MDS remains unknown, the detection of the SF3B1 mutation is helpful to the molecular diagnosis of MDS. In the present study, we established a sensitive, reliable, and rapid scanning method for detecting SF3B1 mutations using a high-resolution melting analysis (HRMA) technique.
Materials and Methods
Patient samples and DNA extraction
This study was approved by the Ethics Committee Board of the Affiliated People's Hospital of Jiangsu University. Bone marrow samples were collected from 92 patients with primary MDS after informed written consent. These patients underwent diagnosis according to the 2008 World Health Organization classification (Vardiman et al., 2009). The mononuclear cells were separated by density-gradient centrifugation using Ficoll. Genomic DNA was extracted using a Genomic DNA Purification Kit (Gentra). The peripheral mononuclear cells from 100 healthy individuals were used as controls.
Primer design and PCR conditions
Three pairs of primers were designed to amplify the five common mutations (K700, K666, H662, R625, and E622) in the SF3B1 gene with LightScanner primer design software v1.0 (Idaho Technology). The sequences of these primers are shown as follows: 5′-GTCTGGCTACTATGATCTCTACC-3′ (forward, E622/R625), 5′-AAAAGCTCTAGCTGTTGTGT-3′ (reverse, E622/R625); 5′-GAAGTCCTGGCAAGCGA-3′ (forward, H662/K666), 5′-ACTTACCATGTTC AATGATTTCAACTA-3′ (reverse, H662/K666); 5′-TGTAGGTCTTGTGGATGA GC-3′ (forward, K700), 5′-GCCAAAGCACTGATGGT-3′ (reverse, K700). The sizes of PCR products were 83, 119, and 51 bp, respectively. PCR was carried out in a volume of 25 μL containing 50 ng genomic DNA, 1× PCR buffer (Invitrogen), 0.25 mM of each dNTP, 2.5 mM of MgCl2, 0.8 μM of both forward and reverse primers, 0.8 μM of internal oligonucleotide calibrators (Qian et al., 2010), 1× LCgreen Plus (Idaho Technology), and 1 U Taq polymerase (MBI Fermentas). A 7300 Thermo cycler (Applied Biosystems), consisting of 95°C for 5 min, followed by 40 cycles, including 94°C for 30 s, 60°C for 30 s, and 72°C for 30 s, was used for PCRs.
High-resolution melting analysis
After PCR, SF3B1 mutations were detected by the HRMA using the LightScanner™ platform (Idaho Technology). Plates were heated from 55°C up to 95°C with a ramp rate of 0.10°C/s. The fluorescence was collected, and the melting curve analysis was performed using the LightScanner software package with CALL-IT® software (Idaho Technology). Melting profiles were calibrated by internal oligonucleotide controls, and then normalized, grouped, and displayed as fluorescence-versus-temperature plots or subtractive difference plots (−df/dt vs. T).
DNA sequencing
To confirm the results of the HRMA, a separate PCR was carried out to generate a larger product (867 bp) using the primers 5′-TTTAGGCTGCTGGTCT-3′ (forward) and 5′-AAGGTAATTGGTGGATT-3′ (reverse). PCR conditions were similar with that for the HRMA. PCR products were directly sequenced on both strands using an ABI 3730 automatic sequencer.
Statistical analyses
The SPSS 17.0 software package was used for the analysis of clinical data. The difference of continuous variables between groups was compared using Mann-Whitney's U-test. The difference of categorical variables between patient groups was compared using the chi-square analysis or Fisher's exact test. A statistical significance was indicated by two-tailed p-values<0.05.
Results
Purified plasmid DNA cloned with an SF3B1 K700E mutant and wild type was generated from one patient with MDS identified with a heterozygous K700E mutation by sequencing. The sensitivity of the HRMA was evaluated by analyzing plasmid DNA with different concentrations of the K700E mutant diluted by wild type (0%, 1%, 2%, 5%, 10%, 25%, 50%, and 100% mutant). The sensitivity test was carried out in quadruplicate to ensure the reproducibility of the HRMA. The K700E mutation could be easily distinguished with the maximal sensitivity of 5% in a background of wild-type DNA (Fig. 1), higher than that of the direct DNA sequencing (25%) (Fig. 2).
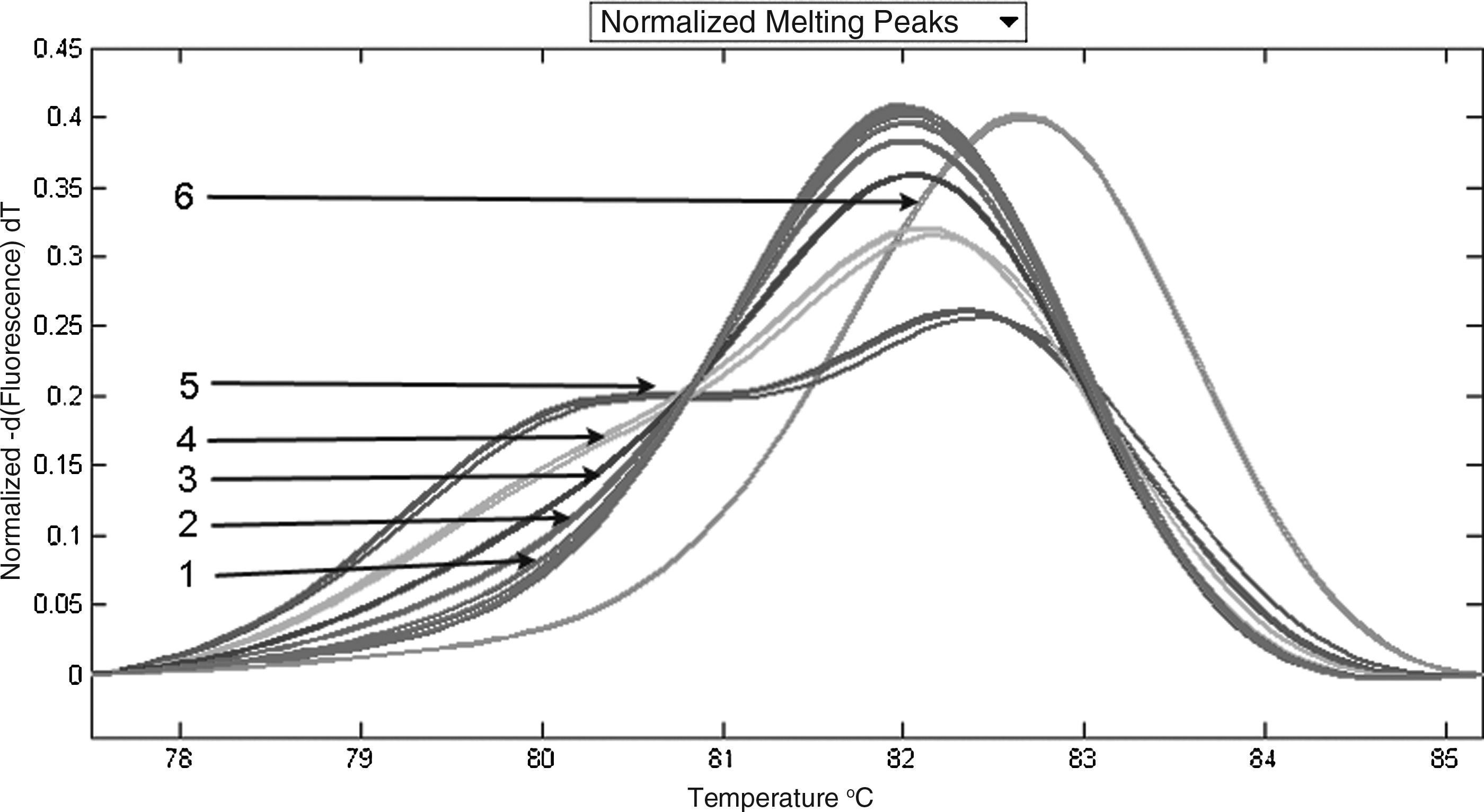
Sensitivity of the high-resolution melting analysis (HRMA) for detecting the SF3B1 K700E mutation. 1: 0%, 1% and 2% mutant; 2: 5% mutant; 3: 10% mutant; 4: 25% mutant; 5: 50% mutant; 6: 100% mutant. The K700E mutation was identified at the maximal sensitivity of 5%.
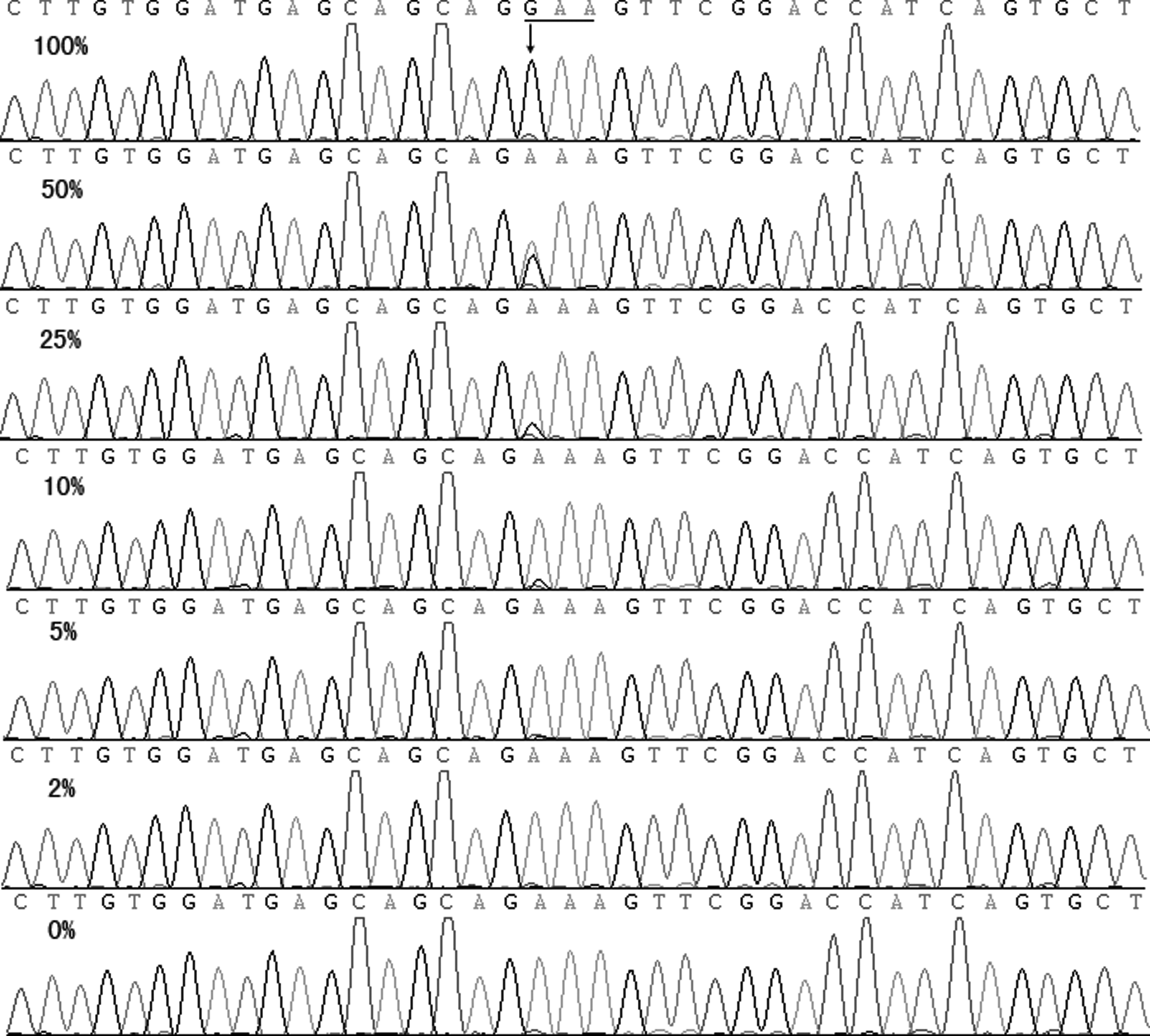
Sensitivity of DNA sequencing for detecting the SF3B1 K700E mutation. The maximal sensitivity of 25% was obtained. Straight line shows the mutated codon; arrow shows the mutation site.
Out of 92 patients with MDS, 5 (5.4%) cases were identified with heterozygous SF3B1 mutations using the HRMA, for the presence of obviously complex, gradual melting curve shapes. The identical judgment was interpreted by two blinded investigators. Subsequently, direct DNA sequencing confirmed the five mutations as three K700E (c.2098A>G, AAA→GAA), one H662Q (c.1986C>G, CAC→GAC), and one K666M (c.1997A>T, AAG→ATG), respectively. The representative melting curves and sequence chromatograms of SF3B1 mutations are shown in Figures 3 and 4. The SF3B1 mutation was not detected in all 100 controls (p=0.024).
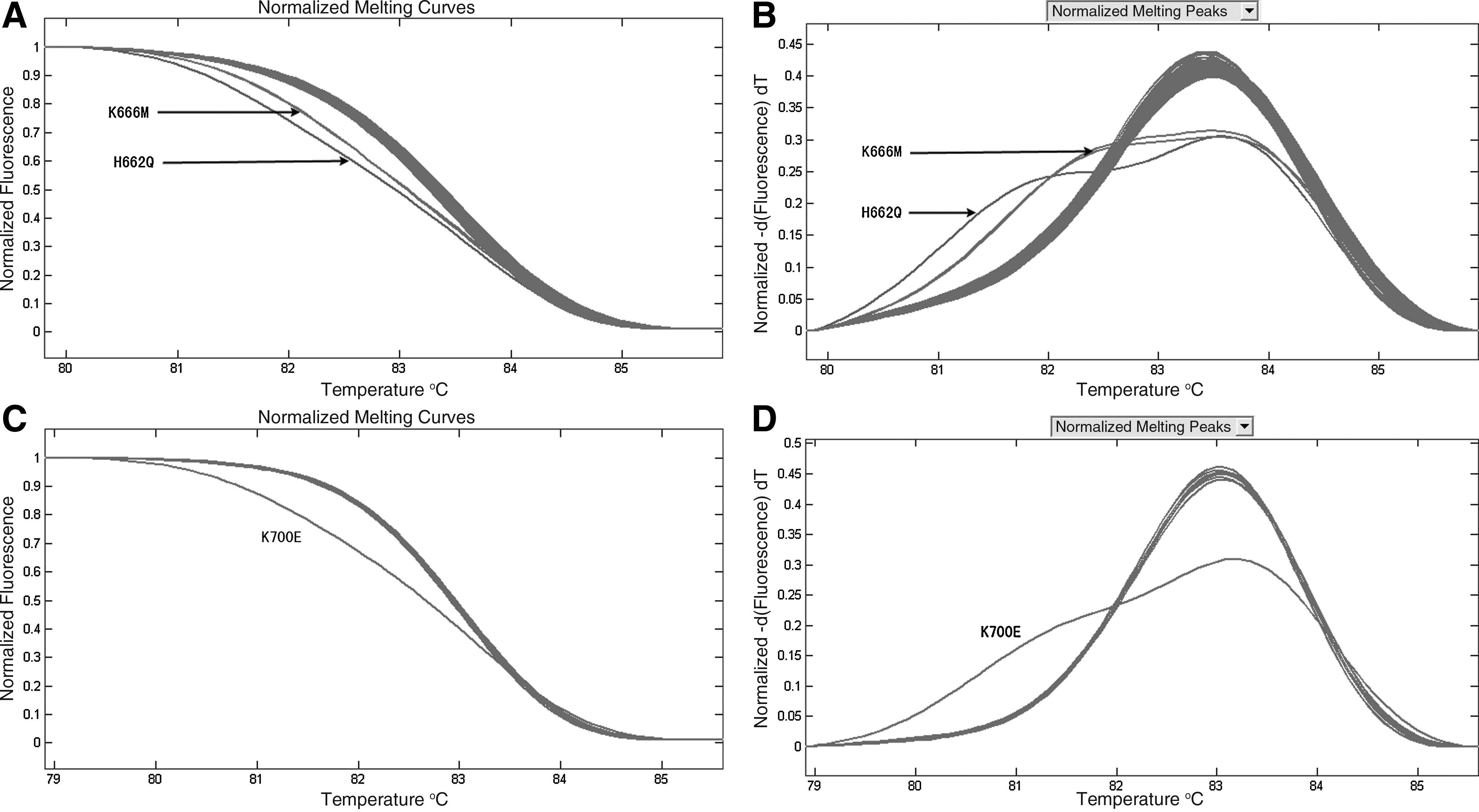
Representative results of the HRMA for detecting SF3B1 mutations in myelodysplastic syndromes.
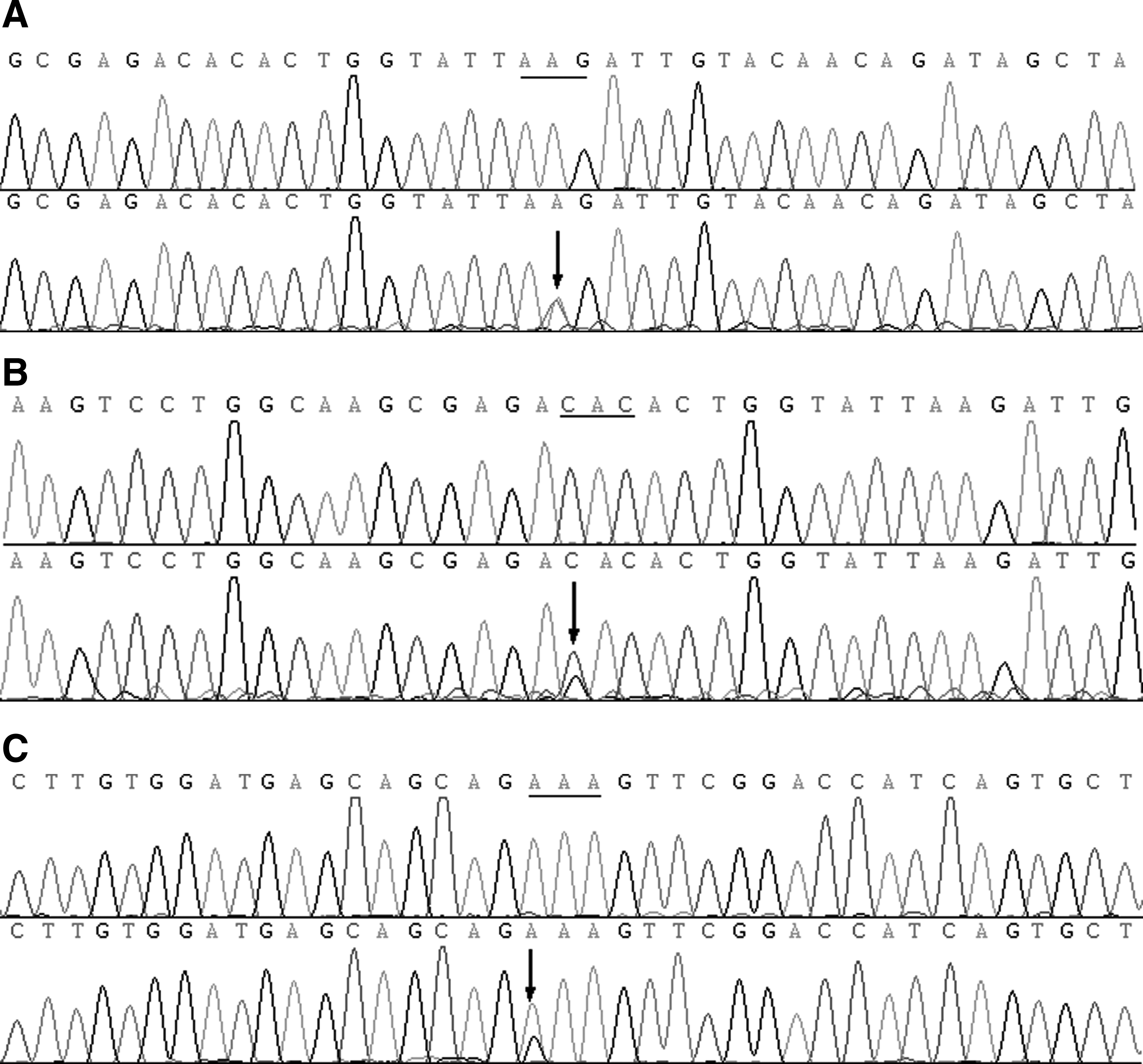
Results of DNA sequencing of SF3B1 mutations.
The clinical features of 92 patients with MDS are listed in Table 1. SF3B1 mutations were more frequently found in the subtypes of refractory anemia with ring sideroblasts (RARS) and refractory cytopenia with multilineage dysplasia and ring sideroblasts (RCMD-RS) than the other categories of MDS (33% vs. 2%, p=0.006). No significant differences in age, gender, blood parameters, and overall survival were observed between patients with and without mutations (p>0.05). According to the karyotype classification, all SF3B1 mutations were identified in patients with a favorable and intermediate-risk karyotype. Further, all SF3B1 mutations were classified into low- and intermediate-risk groups according to the IPSS classification. The clinical and hematopoietic parameters of five SF3B1 mutated cases are shown in Table 2.
WBC, white blood cell count; WHO, World Health Organization; RA, refractory anemia; RARS, refractory anemia with ringed sideroblasts; RCMD, refractory cytopenia with multilineage dysplasia; RCMD-RS, refractory cytopenia with multilineage dysplasia with ringed sideroblasts; RAEB, refractory anemia with excess of blasts; del(5q), MDS with isolated del(5q); MDS-U, myelodysplastic syndrome unclassifiable; IPSS, International Prognostic Scoring System; Int-1: Intermediate-1; Int-2: Intermediate-2.
M, male; F, female; N, normal.
Discussion
RNA splicing is a multistep process by a spliceosomal complex assembly that requires one critical component called U2 small nuclear ribonucleoprotein (snRNP), formed by SF3A, SF3B, and the 12S RNA unit (Gozani et al., 1998). SF3B1 is involved in the early stages of spliceosomal assembly, recruiting U2 small nuclear RNA to the branch-point sequence of introns, directly interacting with U2AF, and helping to specify the site of splicing (Maciejewski and Padgett, 2012). Recently, somatic SF3B1 mutations have been found in 20% patients with MDS, particularly in those characterized by RS (57%-68%) (Papaemmanuil et al., 2011; Yoshida et al., 2011), but at a very low frequency in other myeloid hematopoietic malignancies (Papaemmanuil et al., 2011), which was confirmed by several studies subsequently (Malcovati et al., 2011; Damm et al., 2012a; Makishima et al., 2012; Patnaik et al., 2012). Moreover, SF3B1 mutations were related to better overall survival and a lower risk of evolution into AML (Malcovati et al., 2011; Papaemmanuil et al., 2011; Damm et al., 2012a; Makishima et al., 2012). Thus, the detection of SF3B1 mutations may contribute to molecular diagnosis and prognostic prediction.
Currently, direct DNA sequencing is used to detect SF3B1 mutations (Malcovati et al., 2011; Papaemmanuil et al., 2011; Yoshida et al., 2011; Damm et al., 2012a; Makishima et al., 2012). In this study, we established a rapid high-throughput HRMA protocol to detect SF3B1 mutations, which relied on the saturating doubling-stranded DNA-binding dye, LCGreen, included before PCR amplification, and enabled identification of the PCR products based on their different dissociation behaviors. Heterozygotes were identified by a change of the melting curve shape, and different homozygotes were distinguished by a change of the melting temperature. The performance and interpretation time for the HRMA starting from extracted genomic DNA were 2.5 h, significantly shorter than that for the sequencing method (4 days). Further, the cost could be significantly reduced, as only positive amplicons identified by the HRMA need DNA sequencing. Moreover, the sensitivity of the HRMA in scanning the SF3B1 mutation was 5%, significantly higher than that of DNA sequencing (25%). Additionally, quadruplicate analyses showed a good reproducibility. We further scanned SF3B1 mutations in 92 patients with MDS using the HRMA and identified SF3B1 mutations in 5 (5.4%) cases, which were confirmed by DNA sequencing. Although the frequency of SF3B1 mutations in our cohort was lower than those reported previously (Malcovati et al., 2011; Papaemmanuil et al., 2011; Yoshida et al., 2011; Damm et al., 2012a; Makishima et al., 2012), the discrepancy may caused by the small size of MDS with RS, but not by the methodology. It is also possible that the mutations in other sites were not be detected in this study. A consistent finding was that SF3B1 mutations were more prevalent in RARS and RCMD-RS.
In summary, we established a rapid, reproducible, sensitive, and a high-throughput HRMA assay for the scanning of SF3B1 mutations. This HRMA assay should be more useful in the identification of SF3B1 mutations in clinical diagnostic laboratories.
Footnotes
Acknowledgments
This study was supported by the Science and Technology Special Project in Clinical Medicine of Jiangsu Province (BL2012056), the National Natural Science foundation of China (81270630), the 333 Project of Jiangsu Province (BRA2011085), the Natural Science foundation of Jiangsu Province (BK2009206), and the Social Development Foundation of Zhenjiang (SH2010015 and SH2011056).
Author Disclosure Statement
No competing financial interests exist.