
Abstract
Hereditary Inclusion Body Myopathy (HIBM, IBM2, MIM:600737) is an autosomal recessive adult onset progressive muscle wasting disorder. It is associated with the degeneration of distal and proximal muscles, while often sparing the quadriceps. The bifunctional enzyme UDP-GlcNAc 2-epimerase/ManNAc kinase (GNE/MNK), encoded by the GNE gene, catalyzes the first two committed, rate-limiting steps in the biosynthesis of N-acetylneunaminic acid (sialic acid). Affected individuals have been identified with mutations in the GNE gene. In the present study, the GNE coding region of 136 symptomatic patients were sequenced. A total of 41 patients were found to have GNE mutations. Eight novel mutations were discovered among seven patients. Of the eight novel mutations, seven were missense (p.I150V, p.Y186C, p.M265T, p.V315T, p.N317D, p.G669R, and p.S699L) and one was nonsense (p.W495X), all of which span the epimerase, kinase, and allosteric domains of GNE. In one patient, one novel mutation was found in the allosteric region and kinase domain of the GNE gene. Mutations in the allosteric region lead to a different disease, sialuria; however, this particular mutation has not been described in patients with sialuria. The pathological significance of this variation with GNE function remains unknown and further studies are needed to identify its connection with HIBM. These findings further expand the clinical and genetic spectrum of HIBM.
Background/Introduction
H
The GNE gene encodes for the bifunctional enzyme UDP-N-acetylglucosamine 2-epimerase/N-acetylmannosamine kinase (GNE/MNK) enzyme that catalyzes the first two rate-limiting steps in sialic acid biosynthesis (Hinderlich et al., 1997; Darvish, 2003). The enzyme consists of two domains: the GNE domain carries out epimerase function, while the MNK domain conducts the kinase activity. Mutations in the GNE gene can result in two different human disorders, HIBM or sialuria (Huizing et al., 2005).
Strong evidence suggests that the etiology of HIBM is related to mutations in the GNE gene (MIM:603824). GNE mutations associated with HIBM are predominantly missense mutations found in the GNE or MNK coding domain in either a compound heterozygous or homozygous fashion. HIBM mutations result in the reduced GNE/MNK enzyme, and ultimately, the hyposialylation of skeletal muscle glycoproteins and cell-surface glycoconjugates (Sparks et al., 2005). To date, more than 75 HIBM-associated GNE allelic variations have been described, the most prevalent being the Jewish Middle Eastern founder mutation, GNE:p.M712T in exon 12. (Eisenberg et al., 2001; Nishino et al., 2002; Eisenberg et al., 2003) Although HIBM has primarily been found in the Middle Eastern population, recent findings have described affected individuals of non-Middle Eastern descent with novel mutations that span other regions of the GNE gene, usually in a compound fashion.
In contrast, sialuria is an autosomal dominant disorder that reduces the allosteric feedback-inhibition mechanism, which results in overproduction of sialic acid (Leroy et al., 2001). The reduced feedback-inhibition results in cytoplasmic build-up and urinary excretion of large quantities of free sialic acid. Although the features of sialuria vary widely among affected people, muscle weakness is not related to sialuria. In fact, many affected adults may only experience very mild symptoms or have no health problems related to the condition. All reported sialuria patients are heterozygous for a mutation at amino acid 263 or 266 (Enns et al., 2001). The collection of these mutations suggests that the allosteric site spans between codons 263-266.
In the present study, 136 symptomatic patients referred for molecular diagnostic confirmation were sequenced for variations in the coding region of the GNE gene. 42 patients were discovered to have variations in the GNE gene. A total of 29 different mutations were identified, eight of which were novel. Seven of the novel mutations span either the kinase or epimerase domain. One novel mutation lies within the allosteric site.
Materials and Methods
The assays described were performed by the HIBM Research Group (HRG), a nonprofit molecular genetics laboratory specialized in performing high-complexity clinical molecular genetic testing, regulated under the Clinical Laboratory Improvement Amendments of 1988, California Laboratory Field Services, and accredited by the College of American Pathologists. Confirmation and validation of each assay was performed as part of standard procedures of the laboratory. All reagents were purchased from commercial sources and each batch validated in compliance with the clinical diagnostic quality standards. Reagents and containers were sterile and nuclease free unless otherwise noted.
Patients
All patients were referred to HRG for molecular diagnostic testing. A total of 136 symptomatic patients were included in this study. Buccal epithelial cells were obtained on standard sterile cotton tip swabs and whole blood was collected in EDTA or ACD tubes after consent for GNE testing.
Polymerase chain reaction
Exons 2-12 and their flanking intronic regions were amplified by polymerase chain reaction (PCR) using intronic primers close to the intron/exon boundary. Extracted nucleic acid samples underwent PCR amplification in a Techne TC-412 Thermal Cycler (Barloworld Scientific, Staffordshire, United Kingdom). Each 25 μL reaction comprised of 11.4 μL of triple distilled water, 5 μL of a 5×KAPATaq HotStart Buffer (KAPA Biosystems, Boston, MA), 0.5 μL of the 10 mM dNTP mix, 2 μL of 25 mM MgCl2, 2 μL of the 2.5 μM primer mix (1:1 forward to reverse ratio), 0.1 μL (5 U/μL) of KAPATaq HotStart DNA Polymerase (KAPA Biosystems, Boston, MA), and 4 μL of a 20 ng/μL template DNA. The amplification assay included a 3-min enzyme activation step at 95°C followed by 35 PCR cycles, each of which included three steps: denaturation of DNA template and primers for 30 s at 95°C, annealing of primers to single-stranded DNA template for 30 s at 60°C, and extension of the amplicon strand for 1 min at 72°C. The amplified products were then purified and concentrated using a ZR DNA Clean & Concentrator™ −25 kit (Zymo Research, Orange, CA) according to the manufacturer's instructions and eluted with triple-distilled water to a final volume of 30 μL. The purified amplicon was then electrophoresed and viewed in a 4% Nusieve® 3:1 ethidium bromide-stained precast agarose gel (Lonza, Rockland, ME) for size verification. DNA concentrations and optical densities were quantified using the NanoDrop ND-1000 Spectrophotometer.
Cycle sequencing
A 15 μL reaction mix was prepared for cycle sequencing, comprised of 2 μL of forward primer (1.0 μM), 1 μL of Sequencing Reagent Premix from the DYEnamic ET Terminator® Cycle Sequencing Kit (GE Healthcare Bio-Sciences, Piscataway, NJ), 5 μL of the Better Buffer (Gel Company, San Francisco, CA), and 7 μL of 5 ng/μL purified PCR product. Cycle sequencing was performed using 25 PCR cycles, each of which included denaturation for 20 s at 95°C, annealing for 15 s at 50°C, and extension for 1 min at 60°C. Final products were separated from the reaction mix using the ZR DNA Sequencing Clean Up Kit™ (Zymo Research) and eluted with 10 μL of Hi-Di™ Formamide (Applied Biosystems, Foster City, CA).
Sequencing and analysis
Eluted samples were diluted 1:10 with a total volume of 10 μL and loaded for sequencing on the ABI Prism® 310 Genetic Analyzer (Applied Biosystems). Electropherograms were visually inspected for peak shape and height to confirm the nucleotide identity using the Sequencher™ 4.10.1 software (Gene Codes, Ann Arbor, MI). A minimal 25% relative fluorescence units threshold was set for identification of heterozygous peaks. Results were aligned and compared to the NCBI reference sequence NM_005476.3. In addition, the novel mutations were further analyzed with two in silico bioinformatics tools, Polymorphism Phenotyping-2 (PolyPhen-2) and sorting intolerant from tolerant (SIFT) (Kumar et al., 2009; Adzhubei et al., 2010). Both are tools that predict the possible impact of an amino acid substitution on the structure and function of a human protein. The UniProtKB Protein ID Accession: Q9Y223.1 was used with both tools. Furthermore, the conservation of the affected amino acids were checked by multiple sequence alignment with sequences from Pan trogolodytes, Mus musculus, Rattus norvegicus, Bos taurus, Canis familiaris, and Danio rerio.
Results
A total of 136 patients were tested for GNE gene mutations, all of which were symptomatic for muscular disease. 35 patients had previously described mutations. Seven patients had eight different novel mutations that were unreported. (Table 1; Fig. 1) The eight novel variations are nonsynonymous mutations, including one nonsense (p.Trp495X) and seven missense (p.Asn317Asp, p.Met265Thr, p.Val315Met, p.Tyr186Cys, p.Gly669Arg, p.Ser699Leu, and p.Ile150Val). All seven patients with novel mutations are compound heterozygous. Of the seven, one patient is compound heterozygous with two novel variations, p. Met265Thr and p.Val315Met, which lie within the allosteric site and epimerase domain, respectively.

Electropherogram of eight novel mutations. Eight mutations were found in seven patients experiencing symptoms of muscle weakness.
Seven patients carry novel GNE mutations. Reported mutations have been previously published. Of the eight novel mutations, five of these mutations were found in patients of Caucasian descent, one mutation found in a patient of Pakistani descent, one mutation found in a patient of Indian descent, and one mutation found in a patient of Middle-Eastern descent. All seven patients are compound heterozygous.
SIFT, sorting intolerant from tolerant.
All of these mutations result in nonconservative amino acid changes. One of these results in early termination of the protein: p.Trp495X. Three result in a nonpolar to polar amino acid change: p.Met265Thr, p.Val315Thr, and p.Tyr186Cys. One results in a polar to negatively charged amino acid change: p.Asn317Asp. One results in a nonpolar to positively charged amino acid change: p.Gly669Arg. One results in a polar to a nonpolar amino acid change: p.Ser699Leu. One results in a nonpolar to nonpolar amino acid change: p.Ile150Val. Multiple sequence alignment revealed (Fig. 2), SIFT predicted p.Asn317Asp, p.Met265Thr, p.Tyr186Cys, and p.Ile150Val to be tolerated variations and p.Val315Met, p.Gly669Arg, and p.Ser699Leu to have an effect on the protein functionality. However, Polyphen-2 predicted all six missense mutations likely to be damaging with the exception of p.Met265Thr. The p.Met265Thr mutation was predicted to be benign. Because PolyPhen-2 and SIFT do not have the capability to predict the effects of nonsense mutations, Trp495X was not analyzed. However, the premature termination of a protein will almost always be deleterious and result in the destruction of protein function. These novel mutations are expected to be pathogenic based on the patient clinical history, nature of the amino acid change that occurred, premature translation termination, degree of conservation, and two in silico prediction tools, PolyPhen-2 and SIFT.
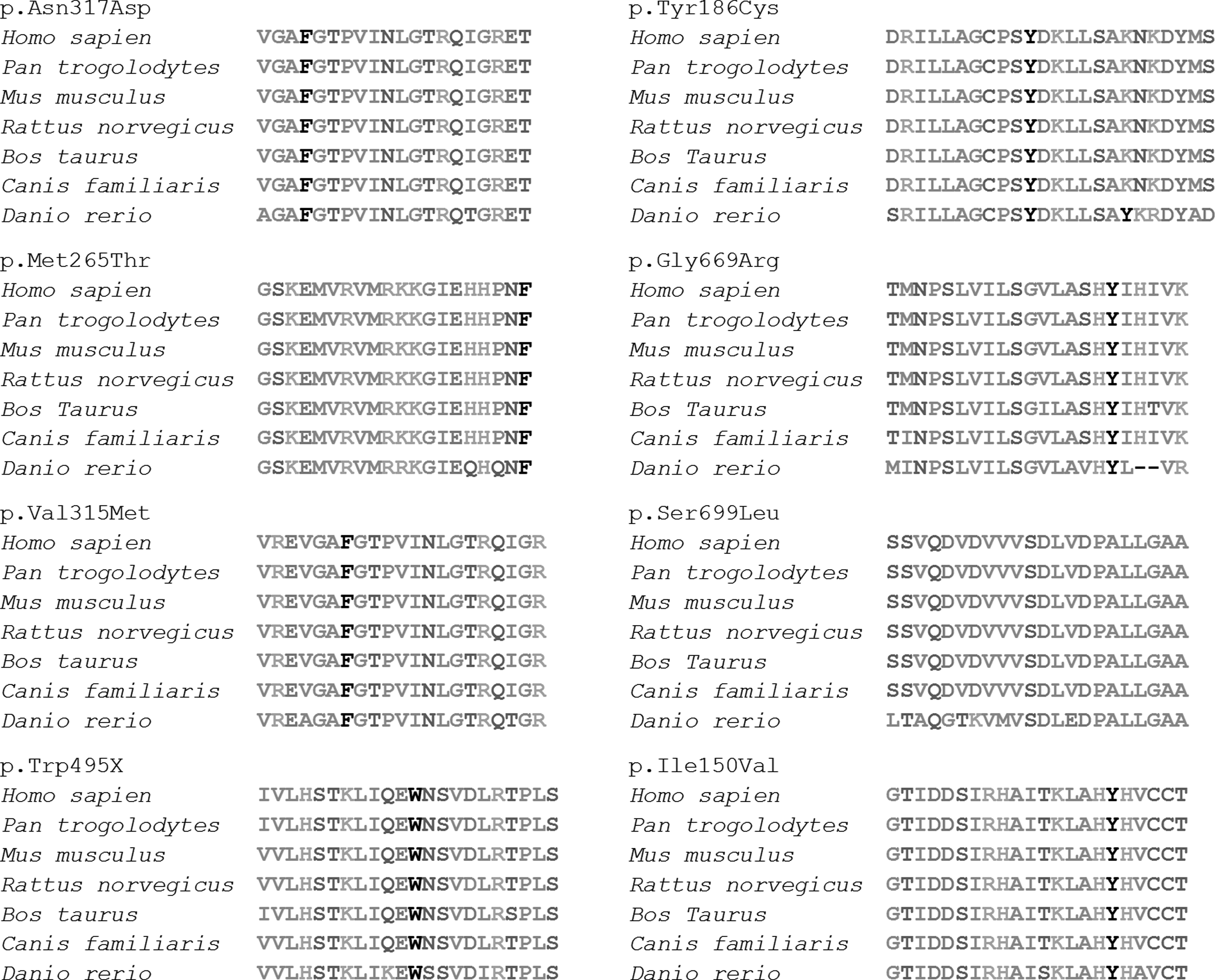
Multiple sequence alignment. Multiple sequence alignment of regions spanning novel mutations in the epimerase/kinase UDP-GlcNac. 2-epimerase/ManNac kinase (GNE/MNK) enzyme. All eight novel mutations occur in positions that are highly conserved in eight different species.
Seven of the novel mutations were found in patients of non-Middle Eastern descent. One novel mutation was found in a patient of Middle Eastern descent. All patients were reported to exhibit muscle weakness and muscle histopathological findings consistent with characteristic features of HIBM. When possible, chromosomal segregation of compound heterozygous patients was verified by sequencing genomic DNA obtained from their biological parents. Additional clinical data were available for six of the seven patients bearing novel mutations, (Table 2) revealing the potential consequences of the novel GNE mutations.
NMD, neuromuscular disease; EMG, electromyography; NCV, never conduction velocity; (normal reference ranges are as follows: men, 52-336 U/L; women, 38-176 U/L).
Patient 2
The patient is a 35-year-old man with a history of calf muscle cramps noted bilateral, predominantly proximal, leg weakness during physical therapy for an injured right knee. Inquiry elicited no family history of neuromuscular disease. The neurological examination showed predominant weakness of hip flexors and adductors; thighs and calves appeared hypertrophic. Laboratory results showed elevated creatine kinase (CK) (509 IU/L) and aldolase (10.2 U/L) with a normal metabolic profile and complete blood count. An MRI of the lumbosacral spine showed grade 1 anterolisthesis of L5 on S1 due to a pars interarticularis defect. Nerve conduction studies were normal; electromyography of arms and legs showed decreased amplitude and duration of voluntary unit action potentials with early recruitment, without myotonic discharges. A biopsy of the right M. quadriceps showed central pallor in scattered fibers on NADH stain; immunocytochemistry for dystrophin, adhalin, gamma-sarcoclycan, beta-dystroglycan, and merosin were negative. Repeat biopsies 7 months later of the right gastrocnemius and left biceps muscles revealed features of a chronic myopathy with rimmed cytoplasmic vacuoles compatible with HIBM. The patient has progressively weakened under our care despite weekly intravenous immunoglobulin (0.4 g/kg), the only commercially available external source of sialic acid.
Patient 3
The patient is a 41-year-old female who was evaluated at the age of 36 due to complaints of muscle weakness. A muscle biopsy of the right gluteus medius performed 1 year after onset revealed varying muscle fibers from ∼10 to 160 micrometers in diameter. Fibers smaller than 25 μm occurred frequently. Several fibers contained one or more small vacuoles sometimes rimmed by a membranous material. Occasional fibers are necrotic or regenerating with an absence of inflammatory changes. In Congo red-stained sections viewed under rhodamine optics, some vacuolated fibers contained congophilic deposits. Electromyography (EMG) studies revealed normal nerve conduction velocities, but with a reduction of muscle in paraspinal muscles and in other muscles that abnormalities appeared to be focal with areas of severe abnormality and other areas of less severe changes. Although there is no apparent defect of neuromuscular transmission, the findings continue to demonstrate abnormalities consistent with a myopathy. There was a mild elevation of CK, 375 U/L. There is no family history of neuromuscular disease.
Patient 4
The patient is a 35-year-old female who developed first symptoms around 21 years of age with tripping and gait difficulties. In addition, she had bilateral foot drop and mild hamstring weakness with quadriceps sparing. There was a clear progression of disease with progressive and severe weakness of the upper and lower extremities and now mild neck flexor and extensor weakness. A manual muscle testing and rating scale of 0-5 performed at 24 years of age revealed the following pattern: Deltoids 2, biceps 0, triceps 2, wrist extensors 0, finger extensors 2, finger flexors 2, interossei, 1, iliopsoas 0, quadriceps 4+, hamstrings 0, tibialis anterior 0, gastrocnemius 0, toe extensors 0, toe flexors 0, neck flexors 4+, and neck extensors 4+.
Absent deep tendon reflexes throughout except 1+ bilateral patellar reflexes. The sensory examination was normal. Laboratory testing revealed normal serum CK levels. EMG studies revealed irritable myopathy affecting the lower extremities. Histologic studies revealed intracellular-rimmed vacuoles without any inflammation. Histochemical studies were consistent with rimmed vacuoles. No other histochemical abnormalities were found. Although no immediate family members have a history of neuromuscular disease, reportedly two cousins in India are affected.
Patient 5
The patient is a 21-year-old female who initially presented muscle weakness in the hands and feet. The patient noticed weakness in both her hands and tripping feet at the age of 17. The progression of the disease was rapid and required a wheelchair after 3 years of onset. EMG studies revealed normal nerve conduction velocities, but with myopathic potentials based on small, brief, and early recruiting. Analysis of a muscle biopsy sample revealed severe variation in the fiber size, thickening of the endomysial with signs of necrosis and regeneration. Additionally, cytoplasmic-rimmed vacuoles were observed with no indication of inflammation.
Patient 6
The patient is a 36-year-old male who initially presented with dorsiflexion weakness in both lower extremities at the age of 31. One year after initial onset, the patient began to experience weakness and atrophy in his hands. Although the progression of the disease was slow and the patient can still walk, he now requires the use of AFO. EMG studies revealed normal nerve conduction velocities, but with myopathic potentials based on small, brief, and early recruiting. Histologic studies revealed variation in the fiber size, cytoplasmic-rimmed vacuoles with no indication of inflammation.
Patient 7
The patient is a 30-year-old right-handed gentleman who initially had mild difficulty ambulating beginning at the age of 21. He initially described increasing stumbles and falls, as well as trouble lifting his toes. His toes and feet often got stuck on the risers when climbing stairs. His weakening progressed over the next few years and eventually developed bilateral foot drop requiring him to use microfiber AFOs. Getting up from a low seated position was difficult. In addition, climbing stairs became increasingly difficulty and now needs to use the side rails to help pull himself upstairs. However, he has not developed any hand or arm weakness. His weakness has stabilized since 2010, and he has not developed any further weakness of functional disability. He has no muscle cramping, trouble swallowing, or shortness of breath. The patient denies a complaint of numbness or tingling in his arms or legs. He denies trouble with bowel or bladder. He does describe mild occasional dizziness, but no vertigo, no loss of consciousness, and no cardiac symptoms. There is no known family history of nerve or muscle disease.
Left bicep muscle biopsy performed on 4/17/2007 revealed mild myopathy without inflammation. There was an increase in internally placed nuclei and a slight increase in atrophic fibers and endomysial fibrosis. EM revealed randomly distributed angulated atrophic myofibers and a small numbers of myofibers with sarcoplasmic zones that contain darkly staining granular material. NADH stain demonstrated a small number of atrophic fibers that stained intensly. Gomori trichrome did not reveal nemaline rods or ragged red fibers.
Immunohistochemistry for Dys 1,2, and 3, alpha, beta, delta sarcoglycan, gamma sarcoglycan, merosin, dysferlin, emerin, and laminin were normal. A stain for ubiquitin did not highlight any inclusions. EMG revealed myopathic appearing motor units in both proximal and distal tested leg muscles, in the setting of normal nerve conduction studies.
Discussion
Here we described eight novel mutations in patients with neuromuscular disease consistent with the HIBM phenotype. By genomic sequencing, we identified eight nucleotide changes that resulted in the mutations p.Asn317Asp, p.Met265Thr, p.Val315Met, p.Tyr186Cys, p.Gly669Arg, p.Ser699Leu, and p.Ile150Val and p.Trp495X in the GNE protein. Three of seven patients are of European descent, one patient is of Asian-Indian descent, one patient is of Pakistani descent, one patient is of Caucasian descent, and one patient is of Middle Eastern descent. In addition, the clinical data for six of the seven patients suggest that the novel GNE mutations are responsible for the HIBM phenotype.
Of the seven HIBM patients we described, patient 2 bears two novel GNE point mutations, p. Arg263Leu and p.Met265Thr, that lie within the epimerase and allosteric domains of the protein, respectively. The p.Met265Thr point mutation is unique because it resides within the allosteric domain of GNE, a site typically associated with sialuria, not HIBM. Sialuria patients have mutations that significantly compromise the feedback-inhibition mechanism, leading to the overproduction of sialic acids. Sialuria patients do not experience symptoms of muscle weakness. Similarly, individuals with a heterozygous mutation in the nonallosteric domain of GNE do not show symptoms of muscular disease. However, patients with homozygous or compound heterozygous mutations in the nonallosteric domain of GNE are symptomatic with a marked decrease in sialylation of glycoproteins. This bi-allelic mutation status suggests that reduced levels of protein and/or protein function result in muscular disease. This novel mutation should be further studied in vitro to confirm its affect on the GNE allosteric domain. Another finding is that the majority of patients with HIBM symptoms do not have a GNE coding mutation. This suggests that a more remote regulatory mutation might affect GNE expression or these are other distal myopathies that are not HIBM.
This work contributes to further understand the potential consequences of novel GNE mutations. A better understanding of the genetics of HIBM will contribute to early diagnosis and prevention of this severe muscular disorder.
Footnotes
Acknowledgments
The authors extend their gratitude to Advancement of Research [for Myopathies (ARM)] who supported this report.
Author Disclosure Statement
No competing financial interests exist.