
Abstract
Spinal muscular atrophy (SMA) is an autosomal recessive neuromuscular disorder characterized by degeneration of alpha motor neurons in the spinal cord, resulting in progressive proximal muscle weakness and paralysis. SMA is the second most common neuromuscular disorder and a common cause of infant disability and mortality. About 95% of patients have a homozygous deletion of exon7 in the survival motor neuron 1 gene. About 50 fetuses from 47 Chinese couples at risk of having an affected child were recruited in this study. The homozygous absence of exon7 of the survival motor neuron 1 gene was detected by both polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) and the quantitative PCR method. Short tandem repeat microsatellite markers linked to the survival motor neuron 1 gene were used to do linkage analysis. In conclusion, the quantitative PCR method results were as reliable as the results using the PCR-RFLP method in prenatal diagnosis. The quantitative PCR method can give more information on SMA carrier status that coincides with the result of linkage analysis.
Introduction
S
SMA is characterized by degeneration of alpha motor neurons in the spinal cord, resulting in a progressive proximal muscle weakness and paralysis. Affected patients are classified into four types on the basis of age at onset and motor function achieved. Type I SMA (Werdnig-Hoffmann disease) patients have onset of clinical signs before 6 months of age, never acquire the ability to sit unsupported, and generally do not survive beyond the age of 2 years; type I is the most severe and common type, which accounts for about 50% of patients diagnosed with SMA. Type II SMA (intermediate) is characterized by onset between 7 and 18 months of age. Patients achieve the ability to sit unsupported, but never acquire the ability to walk independently with survival beyond 4 years of age. Type III SMA (mild, Kugelberg-Welander disease) have onset >18 months of age and during infancy, they develop proximal muscular weakness, they can walk independently, and survive into adulthood. These three types are childhood SMA. Type IV SMA has been added to classify those patients with adult onset at age >18 years and a mild course. This group includes patients who are able to walk in adulthood and are without respiratory and nutritional problems (D'Amico et al., 2011).
The gene locus for SMA has been mapped by linkage studies to chromosome 5q13 (Brzustowicz et al., 1990; Melki et al., 1990). Identification of the survival motor neuron (SMN) gene as the disease-causing gene was in 1995 (Lefebvre et al., 1995). Two almost identical SMN genes are present on chromosome 5q13: the telomeric or SMN1 gene, which is the SMA-determining gene, and the centromeric or SMN2 gene. The SMN1 and SMN2 genes only differ in 5 nucleotides, and the critical one is in exon7(c.840C>T), which leads to the alternative splicing of exon7, causing SMN2 to produce a reduced amount of full length transcripts and also a truncated and unstable protein (Vitte et al., 2007).
About 95% of patients have a homozygous absence of exon7 of the SMN1 gene (homozygous Δ7SMN1) due to deletion or gene conversion of SMN1 to SMN2 (Wirth, 2000). For this reason, the most frequently used clinical diagnosis is to test for homozygous deletion of the SMN1 gene, which can identify ∼95% of SMA patients. Although gene therapy and stem cell therapy to treat SMA patients have made some progress, but till now, SMA is an untreatable disease (Donnelly and Boulis, 2012). Prenatal diagnosis for an affected family is the only way to avoid another affected child.
In this study, we aimed to compare the implementation of SMA prenatal diagnosis using two technologies: one is polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) and the other is a quantitative PCR (Q-PCR) method. PCR-RFLP was developed in 1995 by Ven Der Steege, and through decades of practice, it is viewed as a gold standard in SMA prenatal diagnosis. On the other hand, Q-PCR has always been used in the SMA screening test (Sugarman et al., 2012), but it is a new method for SMA prenatal diagnosis and no investigation of the accuracy of this method usage in prenatal diagnosis has ever been made, especially in a Chinese population. Our main purpose is to compare the results of Q-PCR to PCR-RFLP to evaluate the accuracy of the Q-PCR method. We also expect to obtain accurate dosage information through Q-PCR in the prenatal diagnosis process to help genetic counseling of SMA for Chinese couples at risk of having an affected child.
Patients and Methods
Sample collection and DNA extraction
Fifty prenatal samples from 47 Chinese mothers with a previously affected SMA patient(s) seeking prenatal diagnosis at the outpatient clinic of the genetic counseling and the prenatal diagnosis center department of Shanghai Xinhua hospital (China) were enrolled into this study. Three mothers sought prenatal diagnosis of SMA twice. This study was approved by the Ethics Committee of Shanghai Xinhua Hospital. All the families received genetic counseling before amniocentesis for reviewing the medical and family history and assessing genetic risk. All families gave written informed consent.
Ultrasound guided amniocentesis was performed in the second trimester of the pregnancies between 16 to 20 weeks. Fetal DNA was extracted from 10 mL amniotic fluid samples; parents' genomic DNA was extracted from leukocytes of a 2 mL peripheral blood sample, both using the QIAamp® blood DNA Mini Kit (QIAGEN).
Detection of homozygous Δ7SMN1
The PCR-RFLP analysis method was performed as described by Van der Steege et al. (1995) with modification. Exon7 of SMN was amplified using SMN1-exon7-F: 5′-CTTCCTTTTA TTTTCCTTACAGGGATT-3′; SMN1-exon7-R: 5′-CACTTTC ATAATGCTGGCAGACTT-3′. The annealing temperature was 52°C. To distinguish SMN1 and SMN2 in exon7, 5 μL from the PCR product was incubated at 37°C with 10 U of the HinfI restriction enzyme, which has a specific identifiable site GANTC (Newengland Biolabs®). The enzyme cleaves only the SMN1 exon. Digested products were run on a 2% agarose gel stained with Gelred™ (Biotium) and an 8% PAGE gel with silver stain (Fig. 1). During each test, parents' samples were used as a negative control of SMA, and the proband sample was used as a positive control.

Sample polymerase chain reaction (PCR)-restriction fragment length polymorphism results of families with/without affected homozygous Δ7SMN1. Lanes 1, 2 are the paternal sample (nonhomozygous mutation sample); 3, 4 are the maternal sample (nonhomozygous mutation sample); 5, 6 are the proband sample (homozygous mutation sample); 7, 8 are the fetus sample. Lanes 1, 3, 5, 7 are the PCR product of the survival motor neuron (SMN) gene; 2, 4, 6, 8 are the result of the HinfI cleaved PCR product.
The Q-PCR assay was based on primers that specifically amplify SMN1 using a Syber Green® PCR mix (TakaRa). To distinguish SMN1 from SMN2 in the amplification reaction, 3′- ends of the primers were designed to end on SMN1-specific sequence. The primers used were as follows: SMN1-exon7-Q-F: 5′-CCTTTTATTTTCCTTACAGGGTTTC-3′; SMN1-exon7-Q-R: 5′-GATTGTTTTACATTAACCTTTCAACTTTT -3′ (Lee et al., 2004). As a reference gene, exon 12 of the human serum albumin gene was used. Triplicates of each sample were run in separate tubes on ABI 7500 (PE Applied Biosystems) with SD<0.5.
For the result, we used 30 two-SMN1-copy-female mixed DNA as a reference sample, and then ABI 7500 provided the calculated fold change of the SMN1 gene based on the delta delta CT (ΔΔ CT) method automatically. Through testing 55 patients, 110 parents (known SMA carriers), and 2026 normal pregnancy women undergoing SMA carrier screening, we have standardized our laboratory's own fold change threshold: “0.000-0.001”defined as patient, “0.369-0.595” defined as “1+0” carrier (“X+Y” means X copy of SMN1 on one allele and Y copy of SMN1 on the other allele, so here it means one copy of SMN1 on one allele and zero copy on the other) and “0.801-1.279” has two copies of SMN1 (could be “1+1” normal, or “2+0” carrier). (Fig. 2). (data not show).
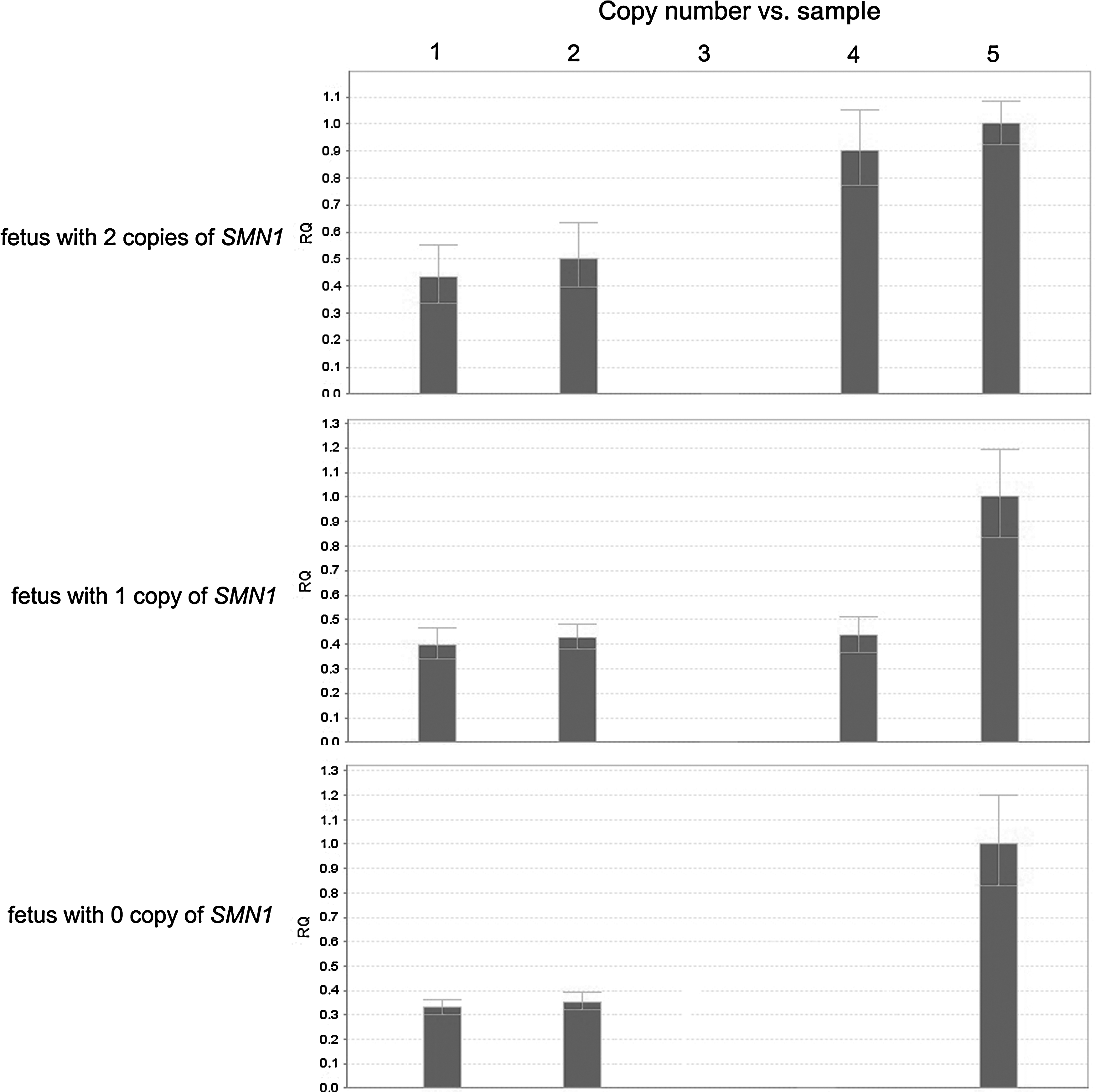
Sample quantitative PCR results of families as homozygous Δ7SMN1 deletion/carrier/noncarrier. X-axis is different sample lanes: lane 1 is the paternal sample; lane 2 is the maternal sample; lane 3 is the proband sample; lane 4 is the fetus sample; lane 5 is the reference sample. Y-axis shows the calculated fold change compared to the reference sample by ABI 7500. Different fold change scale defined each sample as deletion/carrier/noncarrier. RQ, relative quantity.
SMN gene linkage test
SMN gene linked short tandem repeat (STR) loci was chosen according to the polymorphic information among Chinese people. The four loci: D5S435, D5S351, D5S610, and D5S629 are regularly used in each of our SMA prenatal diagnosis cases, all with PIC>0.65. We also have two less polymorphic loci D5S1413 (PIC=0.463) and D5S557 (PIC=0.426) as alternative loci. Detailed information about how these loci were chosen can be found in the article our laboratory published in 2010 (Sun et al., 2010). STR information obtained from the processing family can rule out maternal material containment (MMC) during the test. With the proband's genetic information, we can picture the manner of SMN1 gene transmission in the family.
All the markers selected were labeled with fluorochromes 6-FAM, and the PCR products were analyzed by capillary electrophoresis on an ABI 3730, and the results were analyzed using Genemarker 4.0 software.
All prenatal samples were processed and reported within 24-48 h.
Results
Fifty prenatal tests from 47 families were performed in this study. The fifty tests were classified to two groups: (1) 41 families had at least one affected child with a homozygous Δ7SMN1 gene test and clinical diagnosis before a prenatal diagnosis procedure was done. (2) Six families had no availability of a genetic test for the affected child, but the clinical phenotype strongly supported the diagnosis of SMA. The number of aminocenteses performed for diagnosis was 50 samples, among them, 3 families of the 41 from the first group had amniocentesis two times.
For the first group, nine fetuses out of 44 (20.5%) showed homozygous Δ7SMN1. Both the PCR-RFLP (Fig. 1) and Q-PCR (Fig. 2) assays gave the same result, the STR result showed the same source of the polymorphism of the proband and the fetus within each family. Thirty-five fetuses out of 44 (79.5%) were diagnosed as nonhomozygous Δ7SMN1 using PCR-RFLP, among them, the STR result suggested that 28/44 are carriers, 7/44 are noncarriers. Q-PCR gave us the result that 27/44 is a 1+0 carrier and 1/44 is a 2+0 carrier, 6/44 is a 1+1 noncarrier, and 1/44 is a 2+1 noncarrier.
For the second group, because the genetic material of the affected children could not be obtained for genetic testing, the STR result could only be a tool to rule out MMC during the test. PCR-RFLP assay showed that one fetus out of 6 was homozygous Δ7SMN1, the other five were nonhomozygous Δ7SMN1. The Q-PCR result first suggested that all the parents of the families are 1+0 carriers and the results of the fetuses were 1/6 was homozygous Δ7SMN1, 4/6 were 1+0 carriers, 1/6 was 1+1 noncarrier.
Discussion
Realizing the fact that ∼95% of clinically typical SMA patients have the homozygous Δ7SMN1 mutation, a fast and reliable PCR method for testing SMA was developed in 1995 by Ven Der Steege. And following this idea, molecular genetic testing for the prenatal diagnosis of SMA has been developed and has been approved by many clinical laboratories (Scheffer et al., 2001; Essawi et al., 2012). However, this test cannot distinguish SMA carriers from noncarriers since both are expected to have negative results. And of course, the minority of SMA patients (∼5%) who have a small intragenic mutation in one SMN1 allele instead of the homozygous Δ7SMN1 mutation will also have negative results (Ogino et al., 2002), but this situation is not concerned in this study.
Q-PCR has been used as a SMA screening method, but it's accuracy in the prenatal diagnosis test has never been seriously studied. So in this study, we tried to prove that Q-PCR is as fast and reliable as the PCR-RFLP method Ven Der Steege developed in 1995 through the prenatal test for 50 fetuses. At the same time, Q-PCR can identify the difference between carriers and noncarriers and this character could verify itself as a more promising method in the SMA prenatal diagnosis test.
About 50 fetuses from 47 families with a history of having at least one affected SMA child had been given a reliable prenatal homozygous Δ7SMN1 mutation testing using two parallel methods: PCR-RFLP and Q-PCR. And STR linkage analysis was essential in each test. The result suggested that the Q-PCR method can identify all 10 affected fetuses as the PCR-RFLP method did. And more superior, the Q-PCR method had better coincidence with the STR-linkage study than the PCR-RFLP method. Q-PCR identified carrier and noncarrier status, in addition to giving results as affected or unaffected.
In this study, we have 6 families without index cases. Unlike in some other countries in the Chinese population, no molecular basis of this disease had ever been studied (Essawi et al., 2007); therefore, we had to identify the parents' carrier status before giving them prenatal testing (Cusco et al., 2001). Q-PCR is the only test that could achieve this purpose. In this study, we had identified all parents from these 6 families as carriers before processing the prenatal testing. Thus, Q-PCR for homozygous Δ7SMN1 mutation is particularly useful for prenatal diagnosis in cases where DNA of the index case is not available.
In conclusion, prenatal diagnosis and genetic counseling of SMA are important for SMA families due to the high incidence and fatal outcome of this disease. STR-linkage analysis is very important in prenatal diagnosis testing to rule out MMC and with proband's genetic information, it can detect fetus's carrier status. Analysis of the homozygous Δ7SMN1 mutation using PCR-RFLP has long been used as a standard method in prenatal diagnosis of SMA, but it has some limits on telling the carrier status. In this study, we used the Q-PCR method to identify the homozygous Δ7SMN1 mutation as well as carrier status at the same time; the results proved that the Q-PCR method is as fast and reliable as PCR-RFLP. It also has some advantages: (1) particularly useful in prenatal diagnosis cases, which index case is not available. (2) Q-PCR plus STR-linkage analysis can give more precise genetic image of the fetus status (patient/carrier/noncarrier). (3) Q-PCR plus STR-linkage analysis can identify some special carrier status as 2+0 and will help with future molecular testing.
We suggest that Q-PCR plus STR-linkage methods can substitute for traditional PCR-RFLP plus STR-linkage methods in SMA prenatal diagnosis testing. In the situation when the index case is not available, we recommend using Q-PCR and PCR-RFLP as a support method together, plus the STR-linkage test in the prenatal diagnosis process to double guarantee the accuracy of the result.
More precise and detailed molecular diagnosis information can help a genetic counselor to better explain the prenatal diagnosis result to families of SMA, which can help them to decide different opinions to continue pregnancy, and will help in future pregnancies of their family members.
Footnotes
Author Disclosure Statement
No competing financial interests exist.