
Abstract
Objective:
Quantitative-fluorescence polymerase chain reaction (QF-PCR) was used to detect common fetal aneuploidies in pregnancies with increased (maternal age) or high risk (increased nuchal translucency, abnormal fetal ultrasonography, positive biochemical hormone test, or positive family history) for fetal aneuploidy.
Methods:
The QF-PCR testing was performed on 642 prenatal samples (73.3% amniotic fluids, 26.7% chorionic villus). DNA from prenatal samples were analyzed using an in-house-developed QF-PCR method with 20 micro-satellite markers located on the chromosomes 13, 18, 21, X and Y. Karyotyping of the 392 samples was done and both results were compared.
Results:
634/642 samples were successfully analyzed. In 7.1% of 634 cases numerical chromosome abnormalities were detected. Results of QF-PCR and karyotyping were compared in 392 cases. In the group, with increased risk of fetal trisomy the specificity and sensitivity of QF-PCR method was 100%. Among cases with high risk for fetal aneuploidy, sensitivity was 100% (86.6%-100%); however, the specificity was lower, 91.1% to 100%, depending on the referral reason.
Conclusions:
In women, at advanced age QF-PCR can be used alone without karyotyping. In cases with higher risk, especially those with abnormal ultrasound findings, analysis performed only with QF-PCR is not a sufficient diagnostic method.
Introduction
In recent years, more rapid aneuploidy tests for the most common prenatal chromosome aneuploidies were developed: Fluorescence in situ hybridisation (Klinger et al., 1992) Quantitative Fluorescence Polymerase Chain Reaction (QF-PCR) (Adinolfi et al., 1997) and multiplex ligation probe amplification (Slater et al., 2003) are the commonly used for diagnostic purposes because of the best performance and usability.
Introduction of the QF-PCR of short tandem repeats (STR) markers allowed a rapid and an affordable prenatal diagnosis of common aneuploidies (Mansfield, 1993; Adinolfi et al., 1997). The QF-PCR method is based on a quantitative analysis of the allele signals on a capillary electrophoresis machine to determine the chromosome copy number. The main advantages of the QF-PCR are speed (24-48 h), accuracy and automation.
Different QF-PCR kits are commercially available for the in vitro diagnosis of common chromosome aneuploidies (Devyser Complete, ChromoQuant, Aneufast; Applied ByoSystems) (Association for Clinical Cytogenetics and Clinical Molecular Genetics Society, 2007; Mann et al., 2011). While commercial assays are basically designed for the Caucasian population and are often expensive, there is a need to investigate the informative markers also in other populations (Jain et al., 2012) or to develop their own informative markers. We developed an in-house QF-PCR assay in the Laboratory of Medical Genetics, University Medical Centre Maribor, Slovenia (UMC Maribor), which incorporates 17 STR-markers on chromosomes 13, 18, 21, and 3 markers specific for sex chromosomes.
Furthermore, the successful application of rapid aneuploidy detection tests raised the question about necessity of full karyotyping for all pregnancies (Ogilvie et al., 2005; Kagan et al., 2007) undergoing invasive testing, especially if indicated by maternal advanced age only (Caine et al., 2005). QF-PCR might be used as a stand-alone test for some referral indications (Hills et al., 2010) or as an adjunct test to full karyotype analysis, which subsequently confirms the rapid result and scans for other chromosome abnormalities not detected by QF-PCR assay. According to the Professional European guidelines for QF-PCR, the results of rapid testing may be followed by full karyotype analysis of cultured cells (Association for Clinical Cytogenetics, 2009).
Interestingly, some authors in European laboratories reported promising results only by using QF-PCR approach in a number of pilot studies (Leung et al., 2004; Cirigliano et al., 2009; Badenas et al., 2010), but still, the question remains if this approach is safe enough to be routinely introduced in clinical practice. In some rare cases, normal QF-PCR results and consequent abnormal karyotype in locations not covered by QF-PCR were reported (Caine et al., 2005). Clinical practice shows that all pregnant women having invasive tests also require a rapid test, as well. Recent reviews (Mujezinović et al., 2010) of studies analyzing the effect of rapid prenatal test on maternal anxiety found no conclusive evidence that knowing the results from a rapid analysis reduces maternal anxiety, when waiting for the full karyotype after amniocentesis.
For this reason, we wanted to present 5 years of experience with the in-house-developed QF-PCR assay in the Laboratory of Medical Genetics, University Medical Centre Maribor, Slovenia and evaluate the role of QF-PCR results compared to karyotyping for different indications of invasive prenatal testing.
Materials and Methods
Patients
In a 5-year period, we analyzed 642 samples: 73.3% amniotic fluids (AF) (16-24 weeks of gestation) and 26.7% chorionic villi (CV) (11-16 weeks of gestation). Samples were collected from mothers undergoing invasive testing at the Clinical Department of Perinatology at the University Medical Centre Maribor, Slovenia from January 2008 to December 2012 (5 years). The reasons for prenatal diagnosis included advanced maternal age (MA) (>37 years), increased nuchal translucency (NT) measurement, abnormal fetal ultrasonographic (US) examination, positive biochemical screening hormone test results (SHT), or positive family history (FH).
QF-PCR technology
Genomic DNA was extracted from a 1-3 mL of AF sample or 5 mg CV sample using the PureLink Genomic DNA Mini Kit (InVitrogen) according to the manufacturer's recommended protocols. All samples were prewashed and resuspended with 200 μL 1×phosphate-buffer saline (PBS, pH 7.4) before DNA extraction. QF-PCR analysis was performed within 72 h of sample collection and DNA extraction without previous knowledge of the fetal karyotypes.
PCR amplification was performed in a total reaction volume of 8 μL containing ∼10 ng of extracted genomic DNA, and 9.7-71.9 μM of each primer (Sigma Genosys) and 1×PCR Multiplex Master Mix (Qiagen). A total of 17 STR markers (Table 1) located on chromosomes 13 (n=5), 18 (n=5), 21 (n=7), X and Y (n=3) were amplified in six separate multiplex PCR reactions (labelled as primer mix: PM 1-6). After initial denaturation at 95°C for 15 min, 27 cycles of denaturation at 94°C for 30 s, annealing for 63 s at 64°C for PM1-4, at 56°C for PM5 or 60°C for PM6 and extension at 72°C for 60 s were performed in a PCR thermal cycler (Biometra or Eppendorf). Capillary electrophoresis was performed on Beckman-Coulter CEQ 8000 and data were analyzed with accompanying software.
QF-PCR, quantitative-fluorescence polymerase chain reaction.
Samples were identified as normal when >2 STRs for each chromosome showed peak ratios of 0.8-1.4. Chromosomal aneuploidies were identified when >2 STR showed peak ratios of <0.65 (1:2) or >1.80 (2:1) or 3 signals were present (Adinolfi et al., 1997).
Cytogenetics
For the cytogenetic analysis, samples of 15-20 mL AF or 5-10 mg CV were cultured for metaphase analysis. 20 metaphase spreads per sample were analyzed according to the Association for Clinical Cytogenetics Professional Guidelines (Association for Clinical Cytogenetics and Clinical Molecular Genetics Society, 2007).
QF-PCR versus karyotyping
Results of 392 QF-PCR samples were compared to their respective karyotypes according to the referral reasons for invasive genetic diagnostic (Table 2). Referral reasons for invasive prenatal testing were MA, positive NT measurement and/or serum SHT, other abnormal ultrasound findings (US), or FH of chromosomopathy.
Results are based on QF-PCR analysis for chromosomes 13, 18, 21 compared with cytogenetic analysis. Cases with mosaicism or balanced translocation with rate >10% were excluded.
The sensitivity and specificity with 95% confidence intervals of QF-PCR method for predicting karyotype results were calculated for different referral groups (VassarStats). Karyotypes with mosaicism or balanced translocations with the rate <10% were interpreted as normal.
Results
Summary of the QF-PCR results at UMC Maribor
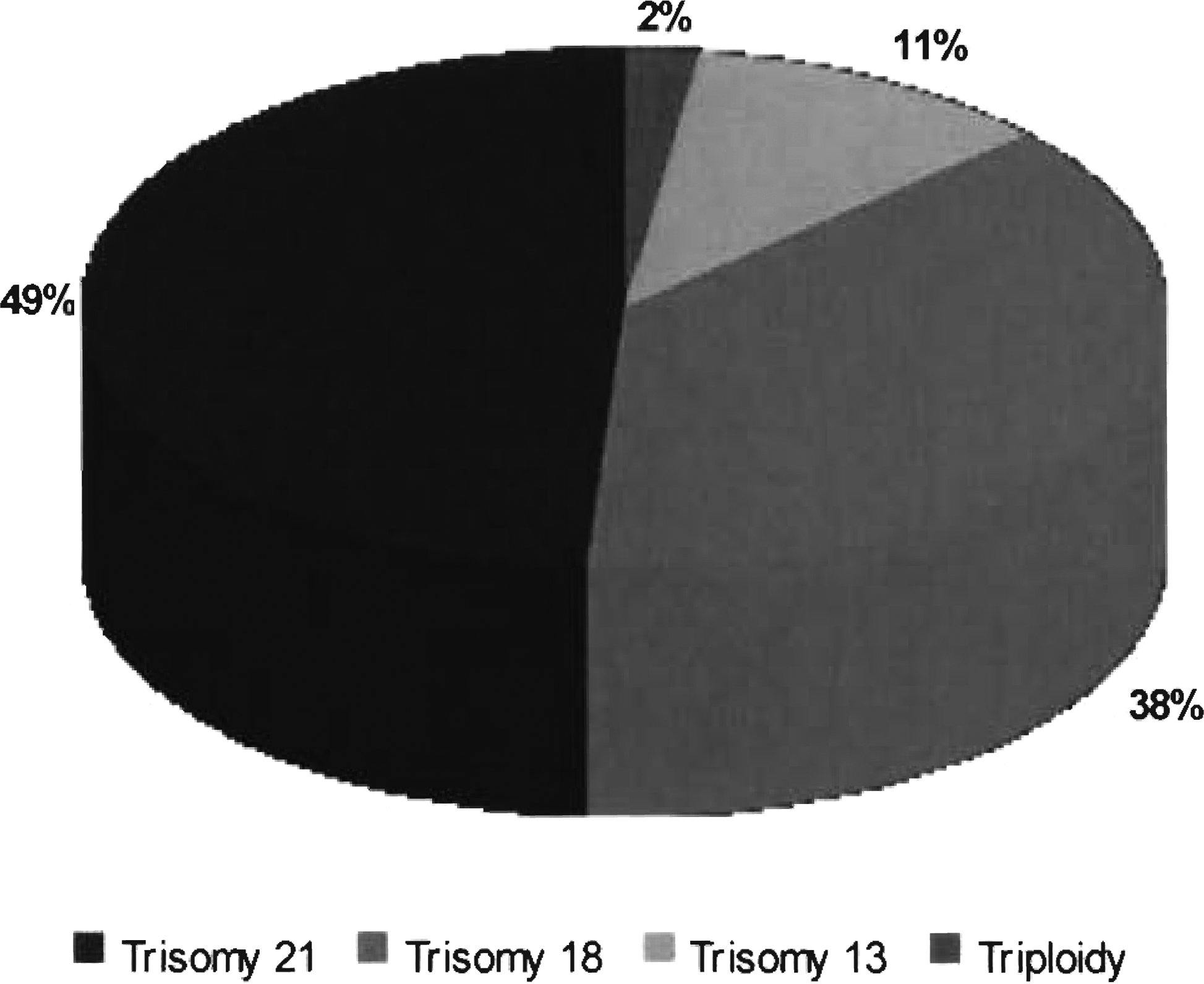
Over the 5-year period from January 2008 to December 2012, we received 642 prenatal samples for rapid QF-PCR testing and 634 (98.8%) were successfully analyzed. Analysis was not successful in eight samples due to maternal contamination. QF-PCR result was normal in 92.8% (589/634) of all successfully analyzed samples. In 45/634 (7.1%) samples chromosomal abnormalities were detected: 44 autosomal trisomies and 1 triploidy (Table 3). In the category of abnormal results, trisomy of the chromosome 21 presented the largest group with 48.9% (22/45) (Fig. 1).
Abnormal quantitative-fluorescence polymerase chain reaction results (n=45) detected in UMC Maribor between 2008 and 2012.
Results are based on QF-PCR analysis for chromosomes 13, 18, 21 compared with cytogenetic analysis. Cases with mosaicism or balanced translocation with rate >10% were excluded.
QF-PCR results versus karyotyping
QF-PCR results were compared to the karyotype in 392/634 (61.8%) cases (AF 65.6% and CV 34.4%). Thirty-two abnormal QF-PCR results (32/392, 8.1%) were detected, all confirmed by karyotyping (Table 4). Among 259 AF samples, 6.9% (18/259) had an abnormal QF-PCR result but cytogenetically, 10.4% (27/259) were abnormal (Table 4). QF-PCR correctly detected 66.7% of 27 samples (trisomies 13, 18 and 21); nine undetected cases were balanced or unbalanced structural rearrangements.
Results are based on QF-PCR analysis for chromosomes 13, 18, 21 compared with cytogenetic analysis. Cases with mosaicism or balanced translocation with rate >10% were excluded.
Among 133 CV samples, an abnormal karyotype was detected in 15.8% cases (21/133). 14 out of 19 cases (73.7%) were in the group of the most common prenatal chromosome aneuploidy rearrangements, correctly detected by QF-PCR. Five undetected cases had other chromosomal numerical aberrations (Table 4).
The total sensitivity of the QF-PCR method according to karyotype results was 100% and the specificity was 96.1% (ranging from 91.1% to 100%) (Table 5).
nc-not calculated, the calculation cannot be performed because the values entered include instance zero.
In a group with MA as a risk factor, the QF-PCR and karyotyping detected two cases (3.1%, 2/65) with abnormal results. In this group the specificity and the sensitivity of the QF-PCR method compared to karyotype results was 100% (Table 5).
Among cases with a high risk for fetal aneuploidy (increased NT, SHT, combination NT+SHT or abnormal US), the specificity was lower, depending upon a referral reason (Table 5). The highest pathology detection rate with QF-PCR method was in a group with the positive NT (15.1%) (8 out of 53); 80% of all abnormalities in this group were correctly detected with QF-PCR.
The highest specificity (100%) was achieved by both, positive NT measurement and SHT; the lowest specificity (91.1%) was in a group with pathological US as a referral reason.
Discussion
QF-PCR is a rapid, simple, and accurate prenatal diagnostic test, proved to be efficient and reliable in detecting numerical disorders of autosomes, as well as sex chromosomes. We use it for the detection of the most common clinically significant numerical abnormalities of chromosomes 21, 18, and 13 in prenatal samples. As a prenatal genetic test it may be useful as a preliminary tool to reduce parental anxiety and to accelerate therapeutic intervention when necessary. The technique is highly suitable for automation and enables high-throughput analysis of samples at a lower cost (Baig et al., 2010; Gekas et al., 2010). The rapid turnover of results, the targeted diagnosis of at-risk pregnancies with QF-PCR testing has been strongly recommended to minimize the waiting time for genetic counseling and for allaying parental anxiety (Leung et al., 2004; Ogilvie et al., 2005; Cirigliano et al., 2006). A common limitation of QF-PCR is that it cannot detect other numerical nor most structural chromosome abnormalities.
We present the blind study performed in Slovenia in which 642 AF and CV samples have been tested using STRs with the QF-PCR. The efficiency of the QF-PCR technique in this study was 98.8% (634/642). Because of maternal contamination 8 out of 642 samples were not successfully analyzed.
A minimum of four specific markers should be tested for each chromosome and two informative marker results consistent with a bi-allelic pattern are required for an unambiguous interpretation (Association for Clinical Cytogenetics and Clinical Molecular Genetics Society, 2007). Our in-house test offers improved diagnostic efficiency because of more STRs markers (17+3 sex chromosome specific) compared to those used in previously reported studies (12-15 on chromosomes 13, 18, 21) (Mann et al., 2011) or in commercially available kits (Devyser Complete: 15+7, ChromoQuant: 17+7, Applied ByoSystems: 19-plex system; Aneufast: 14+3). The efficiency of our self-developed technique was therefore higher: all 634 samples have at least two informative markers and no false positive results were presented in our analysis. Most commercially assays performed similarity in the detection of aneuploidies, frequently observed difference between them is requiring for less frequent reflex testing, which translates into shorter turnaround time and cost saving (Scott et al., 2012).
Out of 634 successfully analyzed samples a normal QF-PCR result was detected in 92.8% (589/634). Forty-four autosomal trisomies of chromosomes 13, 18 and 21 and one triploidy were detected (45/634, 7.1%). Trisomy of the chromosome 21 was the largest category. Our results are comparable with other studies, based on a similar but larger set of samples. In Hills et al. (2010) paper, 9737 patients were analyzed (60% AF sample, 40% CV sample), 10.3% of pathological QF-PCR results with comparable detection rate by each abnormal category results were detected.
In the group of 392 samples, where both analysis, QF-PCR and karyotyping were available, a total 100% (CI 86.6%-100%) sensitivity and 96.1% (CI 93.4%-97.8%) specificity ranging from 91.1%-100% depending on the referral reason was obtained. In this comparative group, thirty-two (32/392, 8.2%) autosomal aneuploidies of chromosomes 21, 18, 13 were detected with both, QF-PCR and by karyotyping, while in total, cytogenetically 46 all chromosomal aberrations were detected (46/392; 11.7%). The highest specificity (100%) was achieved in the group with increased MA and positive NT and SHT; the lowest specificity (91.1%) was evaluated in a group with pathological ultrasound as a referral reason. Relative small numbers of detected chromosome abnormalities by different referral groups are the reasons for the wide ranges of the 95% CI calculated by the specificity and the sensitivity. While false negative results may be incorrectly reassuring before the release of the karyotype, false positive results could have irreversible consequences and potentially leading to the termination of a pregnancy of a healthy fetus with QFPCR analysis we didn't find any false positive case in a 5 year period.
Pathological US markers are often associated with other uncommon chromosomal aberrations (Ogilvie et al., 2005), this is confirmed by our results. The lowest specificity in our analysis was in the group with pathological US (91.1%): 5 out of 10 cases have a normal QF-PCR result and abnormal karyotype. We confirmed that pathological US demands a full karyotype analysis, which enables to find all chromosomal aberrations. Papoulidis et al. (2012) reports that by selectively applying dual testing (karyotype and QFPCR) only at cases with abnormal US and/or positive FH, 0.1% cases of high/unknown risk would have been missed. A similar report Speevak et al. (2011): when QFPCR is performed in all cases and G-banding techniques performed only in higher risk cases, the residual risk for a clinically significant chromosome abnormality will be as low as 0.083%.
Conclusions
Our results demonstrate that QF-PCR is a reliable and rapid method for detection of common numerical chromosome disorders. With its high sensitivity and specificity, as shown in our study, QF-PCR is a reliable and rapid prenatal diagnostic test especially in a group of patients with referral diagnoses advanced MA, and positive NT and SHT. In cases with pathological ultrasound findings, the analysis performed with QF-PCR method only is not enough. An Australian group (Scott et al., 2013) concluded combination qf PCR and array comparative genomic hybridization results is an effective first tier prenatal testing regime, without requiring conventional karyotyping.
Currently in Slovenia, QF-PCR analysis is performed in pregnancies with high risk for fetal chromosome aneuploidy after biochemical SHT, positive US, and increased NT or because of parental anxiety, following always by karyotyping.
Footnotes
Author Disclosure Statement
No competing financial interests exist.