
Abstract
Aim: To evaluate the levels of soluble CTLA-4 (sCTLA-4) in sera of celiac disease (CD) patients with overlapping autoimmune diseases (OAD; diabetes mellitus, autoimmune thyroid diseases, inflammatory bowel diseases, and autoimmune polyendocrine syndromes). Methods: Sera from Italian patients with CD were obtained and enzyme-linked immunosorbent assay was used to measure sCTLA-4. Results: Consistently high serum sCTLA-4 levels were observed in CD (13.20 ng/mL, p<0.0001) and OAD (19.48 ng/mL, p<0.0001) compared to normal controls. A significant increase in the level of serum sCTLA-4 was observed in OAD (p=0.0273) compared to CD alone. At variance, no significant difference in the sCTLA-4 levels was observed when single OAD were compared. Conclusion: The present study shows for the first time a statistically significant increase of serum sCTLA-4 levels in CD patients with associated autoimmune disease (namely, CD and OAD) versus patients with CD alone. Previously, the potential genetic associations of several CTLA-4 polymorphisms to susceptibility to autoimmune diseases have been described, although the relationship between CTLA-4 polymorphisms and the ability to produce the soluble form is not fully clarified. CTLA-4 is a strong actor in the adaptive response: our data give supportive evidence of the common background of autoimmune diseases.
Introduction
C
The CTLA-4 gene, located on chromosome 2q33, is a likely candidate gene for autoimmune diseases because of its role in controlling the T-cell proliferative response. It encodes a T-lymphocyte surface molecule, whose binding to B7 molecules delivers a negative signal to the T cell and can mediate its apoptosis (Harper et al., 1991; Walunas et al., 1994). B7 molecules are expressed on professional antigen presenting cells, such as mature dendritic cells (including Langerhans cells), monocytes, and also B lymphocytes (Sharpe and Freeman, 2002). A native soluble form of CTLA-4 (sCTLA-4), deriving from a lack of transmembrane sequence, has been described (Oaks and Hallett, 2000). The presence of high concentrations of sCTLA-4 was observed in sera of patients with different autoimmune diseases (Saverino et al., 2010).
Several recent studies evaluated the genetic association and contribution of two individual markers from the CTLA-4 gene: +49A/G SNP, rs231775, resulting in a threonine to alanine substitution in the signal peptide of the molecule and the CTLA-4 3′-untranslated region (UTR) (AT)n repeat known to be involved in susceptibility to various autoimmune disease (Schiavo and Saverino, 2013). The relationship between the presence of SNP conferring susceptibility/protection to autoimmune disease and the genetic regulation/modification of CTLA-4 is not yet fully clarified, and in some aspects conflicting (Saverino et al., 2010; Schiavo and Saverino, 2013).
Very recently, AlFadhli (2013) demonstrated increased levels of serum sCTLA-4 in patients with a single autoimmune disease, such as systemic lupus erythematosus and rheumatoid arthritis, as well as in a group of overlap autoimmune disease patients. These results prompt us to explore the levels of this soluble receptor in CD patients with associated autoimmune diseases.
Materials and Methods
Patients
In previous studies, we have evaluated 160 patients with CD (age range 0.8-71), who showed elevated sCTLA-4 levels as measured by the enzyme-linked immunosorbent assay (ELISA) (see below) (Simone et al., 2009). For the present study, we have selected 94 sera for the presence of overlap autoimmune diseases (18 diabetes mellitus [DM], 43 autoimmune thyroid diseases [AIT], 17 inflammatory bowel diseases [IBD], and 18 autoimmune polyendocrine syndromes [APS]). For controls, we collected sera from 45 healthy donors (age range 19-45), as previously described (Simone et al., 2009). The research was approved by the Ethics Committee of the School of Medicine, University of Naples “Federico II,” Italy, and was in accordance with the principles of the Helsinki II declaration. Blood samples were collected after obtaining written informed consent. The diagnosis was based on ESPGHAN criteria (Walker-Smith et al., 1990). All were diagnosed from 2002 to 2005. Serum samples were obtained at diagnosis, before starting a gluten-free dietary regimen. Sera were stored frozen at −20°C in aliquots until use and freezing and thawing were avoided.
Enzyme-linked immunosorbent assay
A specific ELISA was used for measuring serum sCTLA-4 levels (Bender), according to the manufacturer's protocol. Each sample was diluted 1:10 and tested in triplicate. Deviation between triplicates was <10% for any reported value. The lowest sensitivity threshold is 0.1 ng/mL.
The analytical response was linear approximately between 0.162 and 1.200 of absorbance values (corresponding to 0.1-50 ng/mL) as assessed by a serial dilution test using a strongly positive serum (Simone et al., 2009).
Statistical analysis
Statistical analysis was performed using GraphPad Prism software 4·0 (GraphPad Software, Inc.). Because of the skewed nature of some of the data, nonparametric tests were used throughout. The Welch test was used to account for heterogeneity of variances in study groups. The p-values <0.05 were considered significant.
Results
Serum sCTLA-4 levels
To verify the presence of a circulating form of CTLA-4 in human serum, we utilized a sensitive ELISA, as previously published (Simone et al., 2009). Figure 1 shows combined data from the ELISA on patients with CD and normal healthy volunteers, summarizing our previous studies, where the presence of sCTLA-4 was evaluated in 160 patients with CD and 45 healthy donors (Simone et al., 2009), and a group of CD patients with overlapping autoimmune diseases (OAD). Only 7/45 healthy subjects (15.6%, range 0.1-8.4 ng/mL) had detectable serum sCTLA-4 with a detection limit of 0.1 ng/mL. Instead, 145/160 CD patients (90.6%, range 0.1-94.66 ng/mL), and all OAD patients (n=94, range 0.7-98.36) had detectable serum sCTLA-4. Thus, the serum sCTLA-4 concentration was found to be significantly higher in CD (p<0.0001) and OAD (p<0.0001) compared to healthy control.
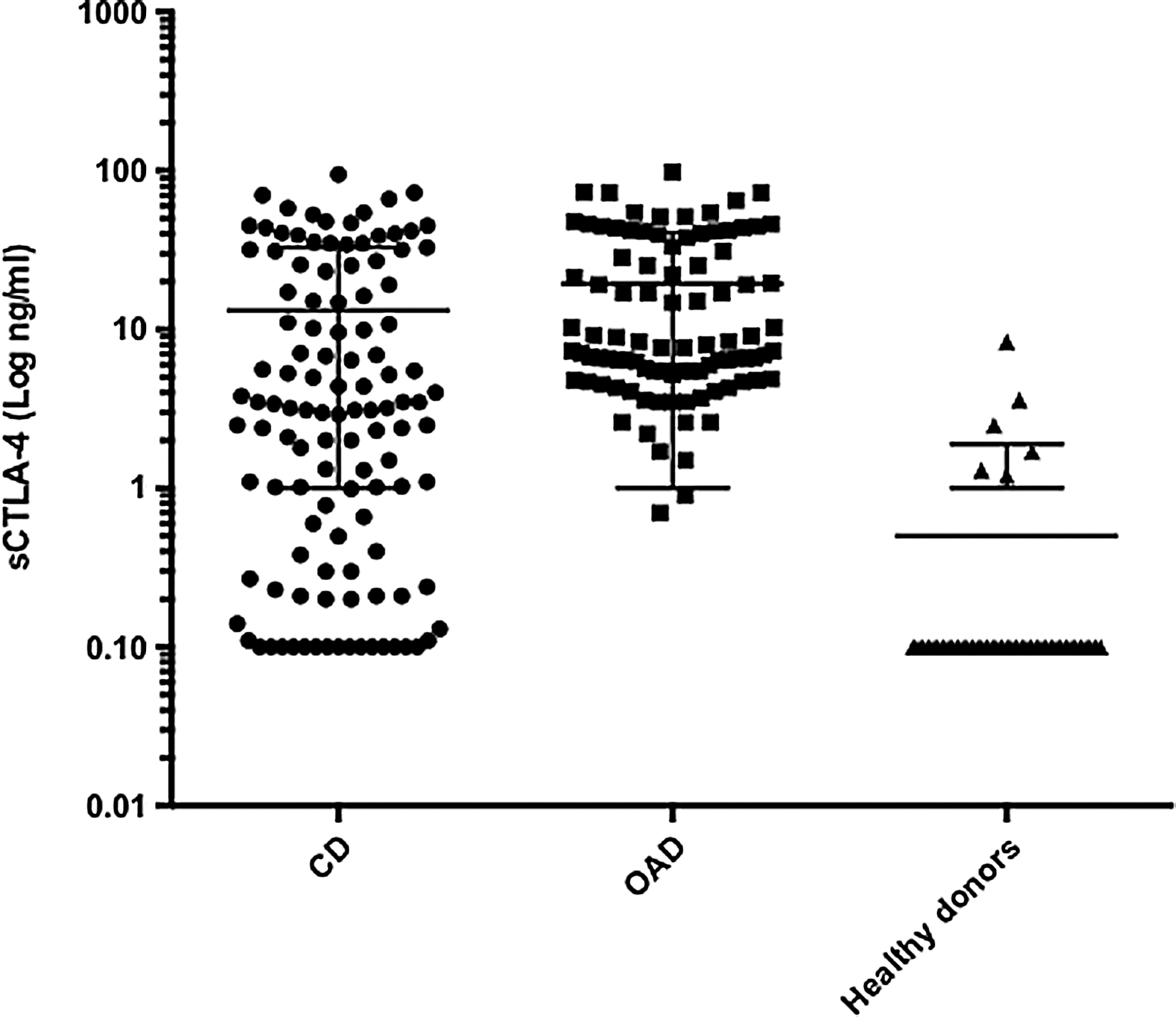
A soluble form of CTLA-4 (sCTLA-4) is differently found in serum of patients with celiac disease (CD), OAD, and normal donors. A sum of previous results on autoimmune patients is presented. The concentration of sCTLA-4 was evaluated by enzyme-linked immunosorbent assay (ELISA) on sera collected from different patients (n=160; CD), and a healthy donor group as a control (n=45). Results are expressed as Log of ng/mL. Each sample was diluted 1:10 and tested in triplicate. Deviation between triplicates was <10% for any reported value (Simone et al., 2009). In addition, concentration of sCTLA-4 was evaluated on sera collected from a group of CD patients with overlapped autoimmune diseases (OAD) (n=94).
Interestingly, serum concentrations of sCTLA-4 were found to be significantly higher in OAD patients (median 7.70, mean 19.48 ng/mL, range 0.7-98.36) compared to CD (median 3.10, mean 13.20 ng/mL, range 0.1-94.66 ng/mL) (p=0.0273, unpaired t-test with Welch's correction).
As depicted in Figure 1, sCTLA-4 concentrations in sera from CD seem to be cluster distributed from the limit of test detection to 94.66 ng/mL. Subsequently, sCTLA-4 concentration values were transformed in folds of increasing the detection limit. Thus, we arbitrary divided these values in subgroups low (1-10-fold, i.e., 0.1-1 ng/mL), medium (10.1-100-fold, i.e., 1.1-5 ng/mL), and high (>100-fold, i.e., >10.1 ng/mL) sCTLA-4 concentration (Fig. 2). Of note, only two sera from OAD patients are in the low subgroup, the others being in the subgroups with higher concentrations. On the other hand, the patients having isolated CD cluster are in the low group, as the few healthy donors having detectable sCLTA4.

sCTLA-4 sera concentration is not equally distributed among the CD population. The arbitrary partition of sCTLA-4 concentration in low, high, and very high values (respectively, ranging 0.1-1.0, 1.1-10.0, and >10 ng/mL) shows different properties of CD patients. In fact, CD alone seems to be almost equally distributed among the three groups, whereas OAD shows a paucity of subjects with low levels of this soluble receptor.
Finally, no significant differences in sCTLA4 levels were observed by comparing each single OAD (DM, AIT, IBD, or APS) (Fig. 3).

sCTLA-4 is increased in all autoimmune diseases, and does not show any cluster in specific diseases. sCTLA-4 serum levels were evaluated on 18 diabetes mellitus (DM), 43 autoimmune thyroid diseases (AIT), 17 inflammatory bowel diseases (IBD), and 18 autoimmune polyendocrine syndromes (APS) overlapping CD.
Discussion
CD is an autoimmune disorder triggered by dietary gluten in genetically susceptible persons. Gluten is a protein complex found in wheat, rye, and barley. CD is characterized by a broad range of clinical presentations, a specific serum autoantibody response, and variable damage to the small intestinal mucosa (Green and Cellier, 2007). CD affects 0.6%-1.0% of the population worldwide (Green, 2005; Green and Cellier, 2007; Telega et al., 2008), with wide regional differences for reasons that are still not fully clarified. Finally, the incidence of CD is increasing in many developing countries because of westernization of the diet, increased awareness of the disease, or a combination of these factors (Green and Cellier, 2007).
Serologic screening studies have shown that only a small proportion of cases of CD are clinically recognized (21% in a recent European study) (Fasano and Catassi, 2010; Mustalahti et al., 2010). The prevalence is 1.5 to 2 times as high among women as among men and is increased among persons who have an affected first-degree relative (10%-15%), type 1 diabetes (3%-16%), Hashimoto's thyroiditis (5%), or other autoimmune diseases (including autoimmune liver diseases, Sjögren's syndrome, and IgA nephropathy), Down's syndrome (5%), Turner's syndrome (3%), and IgA deficiency (9%) (Fasano and Catassi, 2010).
In addition, an association between CD and IBD, the two most common immune-mediated gastrointestinal diseases, has been described (Casella et al., 2010). An increased risk of the familial occurrence of Crohn's disease in patients with CD has been suggested (Casella et al., 2010). Similarly, the association between CD and primary biliary cirrhosis has been well established. In fact, CD and primary biliary cirrhosis share several features, including a higher prevalence in females, autoimmune comorbidities, and specific autoantibodies (Volta et al., 2013).
The importance of CTLA-4 in regulating autoimmune diseases in humans derived from the observation that expression of specific CTLA-4 polymorphisms correlates with a higher incidence of certain autoimmune diseases (Saverino et al., 2010; Schiavo and Saverino, 2013). Polymorphisms have been identified in the promoter region of the gene at position 318 from the ATG start codon; at position 49 in the first exon encoding for CTLA-4, and in an (AT)n repeat within the 3′-UTR of exon 3 (Saverino et al., 2010; Schiavo and Saverino, 2013). However, the mechanism by which CTLA-4 polymorphisms contribute to the pathogenesis of each disease remains unclear.
Several studies have previously reported the increased concentration of serum sCTLA-4 in autoimmune patients (Simone et al., 2009; Saverino et al., 2010; Schiavo and Saverino, 2013). The present experimental data extend these findings particularly in the analysis of overlapped autoimmune diseases. In a very recent study, AlFadhli (2013) demonstrated a significant increase in the serum sCTLA-4 concentration not only in systemic lupus erithematosus and rheumatoid arthritis, but also in a group of overlap autoimmune disease patients when compared to healthy controls. The present study extends this concept showing that a statistically significant increase of serum sCTLA-4 levels exists in overlap autoimmune patients with CD in comparison with patients with CD alone. Our previous studies demonstrated increased levels of sCTLA-4 in CD patients (Simone et al., 2009): the increase in the concentration of serum sCTLA-4 in CD with OAD could highlight the fact that these autoimmune diseases share a common gene or, more likely, a set of causative genes.
It is interesting to note from our previous study that a correlation of anti-tTG IgA with sCTLA-4 concentrations existed throughout the entire CD patient cohort, as well as between the amount of serum sCTLA-4 and the grade of gut mucosa damage (graded as Marsh classification). These suggest a possible immunomodulatory effect of this soluble molecule on cytotoxic T-lymphocyte functions. The present observation highlights the possible pathogenetic role of sCTLA-4 in multiple autoimmune diseases, also on the basis of previously in vitro experiments (Saverino et al., 2007; Saverino et al., 2010; Simone et al., 2013). This may be consistent with the general hypothesis that common etiology paths lead to the development of autoimmune diseases in genetically predisposed individuals. In fact, autoimmune diseases altogether are likely to be the result of hyperactivity of both innate and adaptive immune responses in populations that underwent a positive selection pressure. Recently, several hypotheses are developed trying to underlie the role of specific alleles in the pathogenesis of inflammatory diseases. One of the most fascinating is regarding the selective pressure played by bacterial infections on several loci commonly associated to autoimmune diseases, such as CD, that could be responsible for the normal on-going of the immune response (Zhernakova et al., 2010). These speculations could be consistent with the so-called hygiene hypothesis, which suggests that the changing of hygiene conditions in our lifetimes makes the protective effects of immune responses (evolved in a milieu of high exposure to pathogens) deleterious and possibly a contributory cause of inflammatory diseases (Raj et al., 2013).
Footnotes
Acknowledgment
This study was supported by a grant to DS from University of Genova (PRA), Italy. University of Genova (Italy) had no involvement in study design, nor in the collection, analysis and interpretation of data, or in the writing of the report and in the decision to submit the paper for publication.
Author Disclosure Statement
No competing financial interests exist.