
Abstract
Objective:
This meta-analysis aimed to identify the significance of serum osteopontin (OPN) level for the diagnosis of pancreatic cancer (PC).
Methods:
Through searching the following electronic databases—the Cochrane Library Database (Issue 12, 2013), Web of Science (1945-2013), PubMed (1966-2013), CINAHL (1982-2013), EMBASE (1980-2013), and the Chinese Biomedical Database (CBM) (1982-2013)—related articles were determined without any language restrictions. The STATA statistical software (version 12.0; Stata Corporation, College Station, TX) was chosen to deal with statistical data. Standard mean difference (SMD) and its corresponding 95% confidence interval (95% CI) was calculated. Eleven clinical case-control studies, which recruited 491 PC patients and 481 healthy controls, were selected for statistical analysis.
Results:
Combined SMD of OPN suggested that the serum OPN level in PC patients was significantly higher than that in healthy controls (SMD=3.58, 95% CI=2.42-4.74, p<0.001). Ethnicity stratified analysis indicated a higher serum OPN level in PC patients compared with control subjects among both Caucasians and Asians (Caucasians: SMD=2.62, 95% CI=1.33-3.91, p<0.001; Asians: SMD=4.54, 95% CI=2.80-6.27, p<0.001; respectively).
Conclusion:
The main finding of our meta-analysis revealed that an elevated serum OPN level may be used as a promising diagnostic tool for early identification of PC.
Introduction
H
The OPN protein, first identified as a bone matrix in 1986 in osteoblasts, is considered as an aspartic acid-rich, N-linked (SIBLING) glycosylated protein, which may be highly phosphorylated on serines and threonines according to the cell type (Scatena et al., 2007; Zhang et al., 2013). Acting as a phosphoglycoprotein produced by various tumor cells, OPN was initially characterized as a phosphoprotein secreted by transformed, malignant epithelial cells (Takahashi et al., 2009). Being one of the most critical extracellular structural proteins and an organic component of bone, OPN has various in vivo functions, such as cell adhesion and migration, immune and inflammatory response, apoptosis, and bone calcification (Ramaiah and Rittling, 2008; Wang and Denhardt, 2008). Evidence accumulated that OPN has been implicated in a number of physiological and pathological processes, including fibrosis, neointima formation, arterial occlusion by thrombus, inflammation, and pulmonary hypertension (Cho and Kim, 2009; Inoue and Shinohara, 2011). Detection of plasma OPN level may therefore be useful in the treatment of autoimmune diseases, cancer metastasis, and bone mineralization diseases (Chang et al., 2010; Murugaiyan et al., 2010; Mi et al., 2011). Indeed, numerous studies have been shown that the increased level of OPN was detected in the development and progression of hepatocellular carcinoma, breast cancer, cervical cancer, gastric carcinoma, and so on (Cho et al., 2008; Mi et al., 2009; Shang et al., 2012). More importantly, the elevated serum OPN level could act as a biomarker for metastatic progression and poor survival in patients with pancreatic ductal adenocarcinoma (Brand et al., 2011). Therefore, through taking part in the promotion of cell growth, metastasis, and cell adhesion reduction, the elevated serum levels of OPN may be responsible for the invasion and metastasis of the PC cells and finally lead to the deterioration of tumors (Zhivkova-Galunska et al., 2010). In the past few decades, several previous studies have indicated that an increased serum OPN level may be a biomarker of PC based on its important effect on malignant cell proliferation, tumor metastasis, and survival (Koopmann et al., 2006; Yang et al., 2007); some results are not entirely consistent (Zhu, 2011; Poruk et al., 2013). In this regard, it is worth performing a meta-analysis of all available data to assess the value of serum OPN level for the diagnosis of PC patients.
Materials and Methods
Literature search and selection criteria
The identification of related articles was implemented through searching the following electronic databases without any language restrictions: PubMed, Springer Link, Karger Medical and Scientific Publishers, Chinese Biomedical Database (CBM), Chinese National Knowledge Infrastructure (CNKI), and Google scholar. We employed a search strategy of highly sensitivity in combination with the following keywords and MeSH terms: (“osteopontin” or “OPN” or “sialoprotein 1” or “bone sialoprotein 1” or “secreted phosphoprotein 1” or “uropontin” or “Eta-1” or “2ar”) and (“pancreatic neoplasms” or “pancreatic cancer” or “pancreatic carcinoma” or “PC” or “pancreatic adenocarcinoma” or “pancreas cancer” or “pancreas carcinoma” or “pancreatic tumor”). The references of the present articles and reviews were also manually searched for additional potential studies.
The eligible studies included in our meta-analysis should meet the following three types of inclusion criteria: (1) must concern the diagnostic significance of serum OPN level for PC; (2) patients included in the current meta-analysis should be diagnosed with cytologically or histologically proven PC or PDAC; (3) enough information on serum OPN level should be supplied in eligible articles. Articles that did not meet the inclusion criteria were excluded. If authors published several studies of the same subjects, either the most recent or largest sample size publication was included.
Data extraction and methodological assessment
Two authors used a standardized form to independently collect relevant data from each included study. Controversial problems were resolved by discussion and consensus. By reviewing all the articles, two observers determined the inclusion and exclusion criteria. The language of publication, publication year of article, first author's surname, geographical location, design of study, total number of cases, sample size, the source of controls, cancer type, detection method, and serum OPN level.
Two observers separately assessed the methodological quality with the use of the Newcastle-Ottawa scale (NOS) criteria (Stang, 2010). The NOS criteria comprised three aspects: (1) subject selection: 0-4; (2) comparability of subject: 0-2; and (3) clinical outcome: 0-3. NOS scores ranged from 0 to 9, and a score with good quality should be ≥7.
Statistical analysis
To achieve rigorous statistical analysis, we used the STATA statistical software (version 12.0; Stata Corporation, College Station, TX) to deal with statistical data. Standard mean difference (SMD) and its corresponding 95% confidence interval (95% CI) was calculated. The statistical significance of pooled SMDs was evaluated by the Z-test. Tests for heterogeneity are commonly used to decide on methods for combining studies and for selection of the random-effects model or fixed-effects model. Between-study heterogeneity was assessed by Cochran's Q-statistic and I2 tests in our meta-analysis (Zintzaras and Ioannidis, 2005). A p-value<0.05 or I2>50% means that these studies were heterogeneous, and then the random-effects model was employed; otherwise, the fixed-effects model was implemented. We also made use of subgroup analysis to explore reasons for the detection of heterogeneity. A sensitivity analysis was also implemented to evaluate the influence of a single study on the overall estimate. Funnel plots and Egger's linear regression test were adapted to examine the presence of publication bias (Peters et al., 2006).
Results
Characteristics of included studies
A total of 65 articles relevant to the searched keywords were initially identified. We reviewed the titles and abstracts of all the articles and 34 articles were excluded; full texts and data integrity were then reviewed and another 17 articles were finally excluded. Another three studies were also excluded due to lack of data integrity (Fig. 1). Finally, nine clinical case-control studies with a total of 491 PC patients and 481 healthy controls were selected for statistical analysis (Kolb et al., 2005; Koopmann et al., 2006; Yang et al., 2007, 2010; Chen et al., 2010; Zhang et al., 2010; Chen and Li, 2011; Zhu, 2011; Poruk et al., 2013). The range of publication year of eligible studies was from 2005 to 2013 (Fig. 2). Overall, five studies were conducted among Asians and the other four studies among Caucasians. Two kinds of genotyping methods were adopted in eligible studies, including enzyme-linked immunosorbent assay and electrochemiluminescence immunoassay. NOS scores of all included studies were ≥5. The main characteristics and methodological quality of all included studies are listed in Table 1.
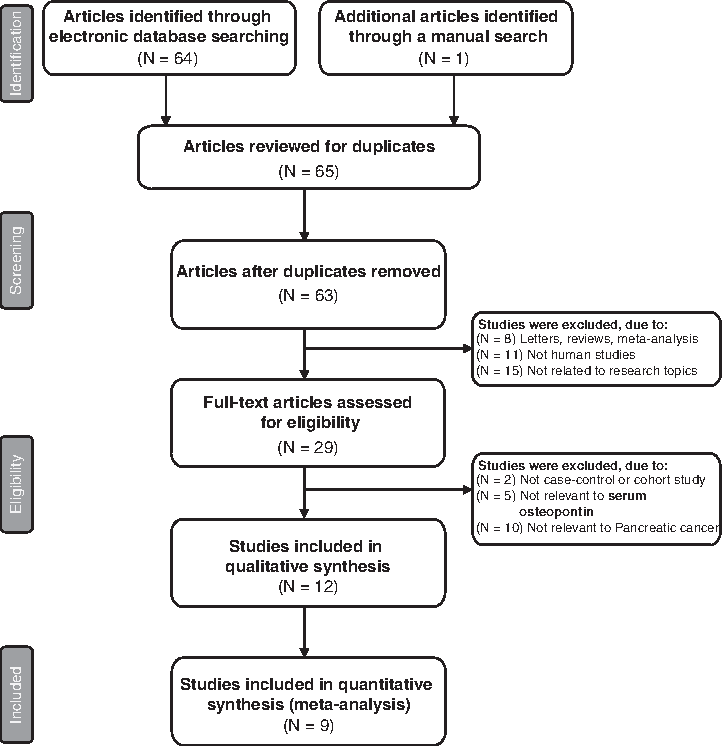
Flowchart of literature search and study selection. Nine studies were included in this meta-analysis.
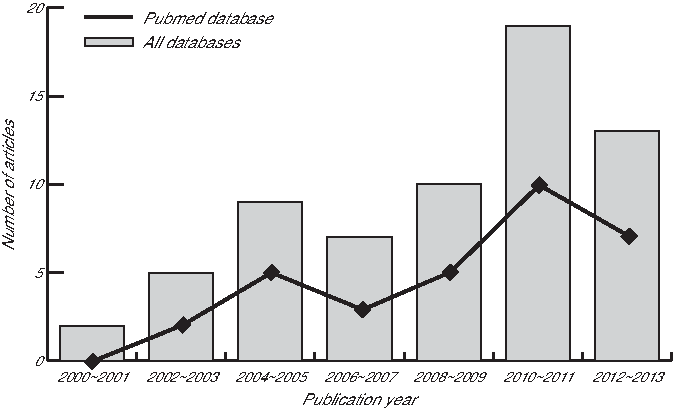
The distribution of topic-related literature in the electronic database over the last decade.
ECLI, electrochemiluminescence immunoassay; ELISA, enzyme-linked immunosorbent assay; F, female; M, male; NOS, Newcastle-Ottawa scale; OPN, osteopontin; PC, pancreatic cancer; PDAC, pancreatic adenocarcinoma.
Quantitative data synthesis
Due to the presence of apparent heterogeneity between studies (all p<0.05), we implemented the random-effects model. The results of the current meta-analysis revealed that the serum OPN level in PC patients was significantly higher than that in healthy subjects (SMD=3.58, 95% CI=2.42-4.74, p<0.001) (Fig. 3).
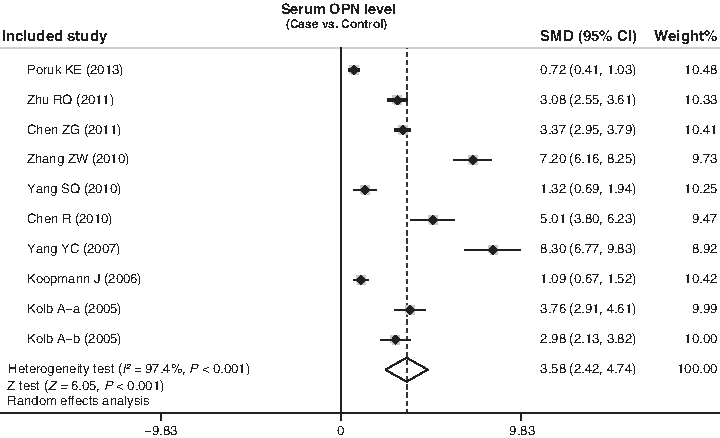
Forest plots for the significance of serum osteopontin (OPN) level for the diagnosis of pancreatic cancer.
Ethnicity stratified analysis findings showed that the elevated serum OPN level was significantly related to the development in PC patients among both Caucasians and Asians (Caucasians: SMD=2.62, 95% CI=1.33-3.91, p<0.001; Asians: SMD=4.54, 95% CI=2.80-6.27, p<0.001; respectively) (Fig. 4). We also performed a subgroup analysis by sample size, cancer type, and detection method; we observed a significant association between the increased serum OPN level and the development of PC in all these groups (all p<0.005) (Fig. 4).
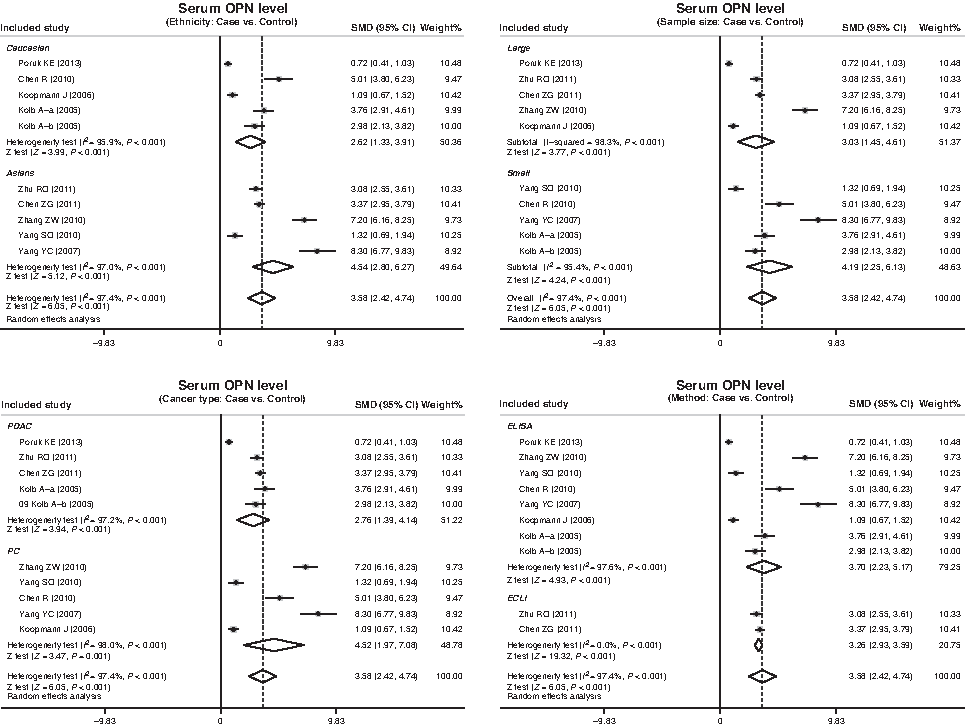
Subgroup analyses by ethnicity, sample size, cancer type, and detection method for the diagnosis of pancreatic cancer.
To assess the influence of each individual study on the pooled SMDs, we performed a sensitivity analysis by omitting individual studies. The results of sensitivity analysis indicated that the removal of any single study could not affect the overall pooled SMDs (Fig. 5). There was strong evidence for asymmetry presented in the funnel plots (Fig. 6). The presence of publication bias was also strongly demonstrated by Egger's test (t=3.71, p=0.006).

Sensitivity analysis of the summary odds ratio coefficients for the diagnosis of pancreatic cancer.
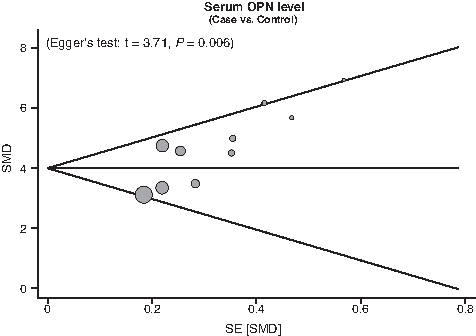
Funnel plot of publication biases for the diagnosis of pancreatic cancer.
Discussion
We aimed to evaluate the potential significance of serum level of OPN for diagnostics. Our results showed that the serum OPN level in patients with PC was significantly higher than in the control participants, suggesting that the level of OPN may be essential as a therapeutic approach for predicting the invasion and metastasis of PC cells. It is noteworthy that OPN is a crucial adhesive bone matrix protein that plays an important role in immune cell recruitment, wound healing, and tissue remodeling (Takenaka et al., 2013). An increased expression of OPN is found to occur not only in pathologic conditions such as inflammation or ischemia but also in many types of malignancies (Sreekanthreddy et al., 2010; Rud et al., 2013). However, up to now, there is only limited information about the role of OPN in pancreatic diseases, not to mention the possible mechanisms of increased OPN expression and induction in PC. As a matter of fact, OPN itself contains several adhesive amino acid sequences, which would contribute to the interaction with cell surface receptors like CD44 and integrins (Ramaiah and Rittling, 2008). With respect to this, OPN is therefore known to play a critical role in cell adhesion and metastasis based on one of its binding domains on the arginyl-glycyl-aspartic acid sequence that interacts with integrins and the extracellular matrix (Narisawa et al., 2013). For the above reasons, the elevated level of OPN could stimulate cell migration and tumor growth by acting as a proangiogenic factor and by strengthening invasiveness and metastasis of tumor cells through binding to CD44 and certain integrins and, therefore, resulting in the invasion and metastasis of human tumor cells (Kolb et al., 2005). We therefore hypothesized that the intrinsic OPN excess production may be at least, in part, conducive to the aggressive and invasive behavior of human PC. This result agreed with the conclusions of the study conducted by Poruk et al. (2013) who showed a significant association between the increased serum level of OPN and the invasiveness of PC cells as well as the growth of metastases, supporting that OPN may serve as a serum marker for PC. Similarly, Kolb et al. (2005) also provided further evidence of the importance of OPN in the biology of PC and that blockade of OPN might be useful as a therapeutic approach to inhibit invasion and metastasis of PC cells.
In our meta-analysis, we had dealt with numerous heterogeneity problems. Further subgroup analysis by ethnicity identified that the increased level of OPN may be significantly associated with a decreased overall survival rate in PC patients among both Caucasian and Asian populations. The present meta-analysis indicates that ethnicity difference may not have an impact on the heterogeneity of outcomes in the pathogenesis of PC.
Although our meta-analysis was a practical way to generate a more powerful estimate of true effect size with less random error than individual studies, it did come with some potential limitations. First, we did not take into account unpublished articles and abstracts since a myriad of needed information could not be successfully obtained. In this regard, due to the small number of studies, our results did not include all the data from all trials to evaluate the relationship of serum OPN level with the pathogenesis of PC. Nevertheless, our meta-analysis managed to overcome the limits of size or scope in individual studies to acquire more reliable and general information from each study. A second limitation of our meta-analysis is the fact that the results of meta-analysis might lack reliability to some extent since it is a retrospective study, which may induce potential publication bias. Especially, we enrolled eligible English studies, only which may relate to the occurrence of potential biases because of excluding parts of qualified studies based on language criteria. Another potential limitation is that our meta-analysis may still be underpowered to acquire original data from the included studies. Despite the above limitations, this is the first example of meta-analysis on the association of serum OPN level with the development of PC. More importantly, our meta-analysis uses a statistical approach to combine the results from multiple studies. To achieve strong objectivity, all the research methods were carried out using strict inclusion and exclusion criteria. Besides, inconsistency of results was rigorously quantified and analyzed in our meta-analysis, leading to a more reliable conclusion.
In conclusion, the present meta-analysis suggests that an elevated serum OPN level may be used as a promising diagnostic tool for early identification of PC. Nevertheless, due to several limitations addressed previously, further clinical research8 with more integral data and larger sample size is warranted to obtain a more generally applicable statistical analysis.
Footnotes
Acknowledgments
This work was supported by the Scientific Research Fund of Liaoning Province Education Department (No. L2010627). The authors would like to acknowledge the reviewers for their helpful comments on this article.
Author Disclosure Statement
No competing financial interests exist.