
Abstract
Background: Rupture of vulnerable plaque with subsequent thrombus formation has been implicated as the most common pathogenic mechanism responsible for acute coronary syndrome (ACS). Angiographic coronary lesion complexity has been reported to reflect plaque vulnerability. Macrophage migration inhibitory factor (MIF) is a proinflammatory cytokine and might be involved in the pathophysiology of atherosclerotic plaque destabilization. Objective: This study was designed to investigate if serum MIF levels are associated with angiographic coronary lesion complexity in patients with coronary artery disease (CAD). Materials and Methods: A total of 232 consecutive CAD patients and 76 controls were recruited. CAD patients were subdivided according to the presence of ACS (n=138) or stable angina pectoris (SAP) (n=98). Coronary lesion morphology was assessed by coronary angiography. Serum MIF levels were measured by an enzyme-linked immunosorbent assay. Results: SAP patients had significantly higher serum MIF levels compared with healthy controls, and ACS patients had significantly higher serum MIF levels compared with SAP patients. In SAP patients, serum MIF levels were independently associated with the presence of complex coronary lesion. In ACS patients, serum MIF levels increased in conjunction with the extent of complex lesions. Conclusions: Serum MIF levels are a potential biomarker for reflecting the presence and severity of angiographically complex coronary lesion in CAD patients.
Introduction
A
Although the identification of vulnerable plaques remains a challenge, it has been reported that plaque vulnerability, such as plaque rupture, plaque hemorrhage, or thrombus formation, can be obtained from angiographically complex lesions (Maehara et al., 2002; Otsuka et al., 2006). However, as coronary angiography is an invasive procedure requiring catheterization, scientists and doctors hope to develop noninvasive alternatives such as blood biomarkers to detect vulnerable plaques even in asymptomatic patients with CAD.
Various studies have confirmed the strong correlation between inflammation and the development of vulnerable plaque (Seneviratne et al., 2013). Therefore, the investigators believe that inflammatory markers represent the potential predictors for vulnerable plaque. Macrophage migration inhibitory factor (MIF) is a proinflammatory cytokine, and the glucocorticoid-induced immunomodulator mainly produced by macrophages in response to a variety of inflammatory stimuli (Calandra et al., 1994). Previous studies have revealed that MIF is involved in the pathogenesis of sepsis, inflammatory and autoimmune diseases, and atherosclerosis (Lue et al., 2002; Calandra and Roger, 2003; Muller et al., 2012). Previous studies have demonstrated that serum MIF levels were increased in ACS patients (Muller et al., 2012) and correlated with signs of plaque instability in patients with carotid atherosclerosis (Schmeisser et al., 2005). However, the relationship between serum MIF levels and angiographically vulnerable plaque in CAD patients has never been fully elucidated. The aim of the present study was to evaluate serum MIF levels in patients with CAD and to assess its efficacy in the identification of angiographically complex coronary lesion.
Materials and Methods
Study population
We performed a single-center, prospective cross-sectional study. Patients enrolled in this study were patients who underwent diagnostic conventional coronary angiography for suspected CAD in Qilu Hospital between May 2013 and January 2015. A total of 232 consecutive CAD patients were recruited. CAD patients were subdivided according to the presence of ACS (n=138) or stable angina pectoris (SAP) (n=98). Besides, we also recruited 76 age- and sex-matched volunteers undergoing routine physical examination in our hospital during the same period as healthy controls. Patients with heart failure, cardiomyopathy, infective diseases, active inflammatory disease renal failure, severe liver complications, cancer, peripheral artery diseases, or hematological disorders were excluded from the study. Acute myocardial infarction (AMI) and unstable angina pectoris (UAP) were included in the ACS group. We defined AMI as chest pain that persisted for >30 min, arrival at hospital within 12 h of the onset of chest pain, new ST-T wave changes or a new left bundle branch block on a 12-lead electrocardiogram, and elevated cardiac markers (creatine kinase-myocardial bound or troponin I). We defined UAP as angina at rest, accelerated angina, or new-onset angina without elevation of cardiac markers. We defined SAP as no change in the frequency, duration, or intensity of angina symptoms within 6 weeks before admission. All participants provided written informed consent before enrollment in the study entry. The study protocol was approved by the Ethics Committee of Qilu Hospital.
Angiographic analyses
Coronary angiography was carried out through the right radial artery or the femoral artery approach by conventional multiposition projection in the catheterization of our hospital. Angiograms were analyzed by two experienced interventional cardiologists unaware of the laboratory values. Coronary stenosis was assessed morphologically according to the Ambrose classification and was classified as either simple or complex (Ambrose et al., 1986). Briefly, complex lesions were defined according to the presence of at least one of the following features: (1) irregular morphology or scalloped borders, or both; (2) overhanging or abrupt edges perpendicular to the vessel wall; (3) plaque ulceration; (4) the presence of filling defects consistent with intracoronary thrombus. Coronary lesions with no complex features were classified as simple lesions.
Blood collection and biochemical analyses
Blood samples were taken under fasting conditions directly before coronary angiography. Venous blood was drawn from the antecubital vein with minimal tourniquet pressure into serum separator tubes. Samples were allowed to clot for 30 min and stored at −80°C until analysis. Serum fasting blood glucose (FBG), triglyceride, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-c), and high-density lipoprotein cholesterol (HDL-c) were measured on a Hitachi 7600 Automatic Biochemical Analyzer (Hitachi Co., Tokyo, Japan) using the standard laboratory protocol. Quantitative determination of MIF levels in the serum was performed using the commercial immunosorbent assay (enzyme-linked immunosorbent assay) kits with an intra- and interassay coefficient of variation of both <10% according to the manufacturers' protocols (R&D Systems, Minneapolis, MN).
Statistical analyses
Data were analyzed using SPSS 16.0 for windows (SPSS, Inc., Chicago, IL), results for normally distributed continuous variables are expressed as the mean±standard deviation, and continuous variables with non-normal distribution normality were expressed as the median value (interquartile range). Comparisons between two groups were performed using the unpaired t-test, Mann-Whitney U test, or the chi-square test, as indicated. Comparisons of three or more groups were performed by the one-way analysis of variance, Kruskal-Wallis test, or chi-square test, when appropriate. Bonferroni-corrected post hoc test was employed to adjust the observed significant level for multiple comparisons if the null hypothesis was rejected. Multivariate logistic regression was performed to assess the presence of complex lesion in patients with SAP. Values of p<0.05 were considered significant.
Results
Baseline characteristics
In Table 1, the baseline clinical and laboratory characteristics of the subjects are depicted. With a mean age of 61 years and 63% males, the study population reflects a relatively typical population of patients with CAD. Compared with healthy controls, CAD patients had significantly higher blood pressure, FBG, TC, and LDL-c levels. CAD patients also had significantly lower HDL levels compared to healthy controls. In CAD patients, ACS patients had significantly higher LDL-c levels compared with SAP patients.
All values are mean±standard deviation, median value (interquartile range), or n (%).
p<0.05 compared with healthy controls.
p<0.05 compared with SAP patients.
ACEI, angiotensin-converting enzyme inhibitor; ACS, acute coronary syndrome; ARB, angiotensin receptor blocker; BMI, body-mass index; DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol; MIF, migration inhibitory factor; SAP, stable angina pectoris; SBP, systolic blood pressure; TC, total cholesterol; TGs, triglycerides.
Serum MIF levels in subjects
As shown in Table 1, SAP patients had significantly higher serum MIF levels compared with healthy controls (1.35 [0.88-3.05] vs. 0.18 [0.14-0.33] ng/mL, p<0.05). In CAD patients, ACS patients had significantly higher serum MIF levels compared with SAP patients (3.06 [1.97-5.20] vs. 1.35 [0.88-3.05] ng/mL, p<0.05).
Serum MIF levels in SAP patients
Patients with SAP were divided into the following two groups: simple lesion (n=50) and complex lesion (n=48) according to the presence or absence of angiographically complex coronary lesions. As shown in Figure 1, SAP patients with a complex lesion had significantly higher serum MIF levels compared to those with a simple lesion (1.98 [1.02-4.01] vs. 0.98 [0.67-2.23] ng/mL, p<0.05). Multivariate logistic regression demonstrated that serum MIF levels were independently associated with the presence of complex coronary lesion in SAP patients (OR: 1.46, 95% CI: 1.13-1.88; p=0.004) (Table 2).
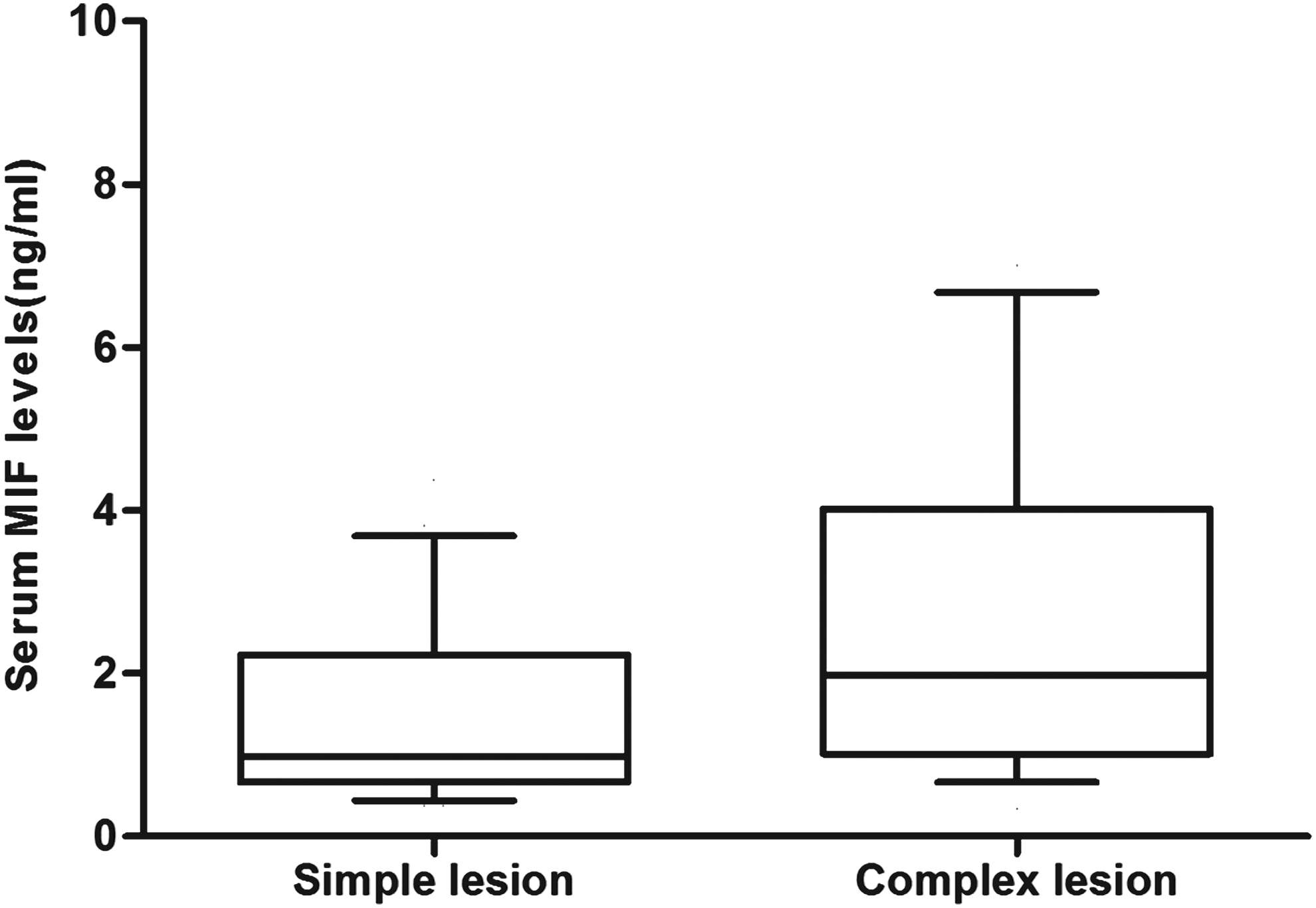
Box-and-whisker plot showing serum migration inhibitory factor (MIF) levels in stable angina pectoris patients with simple (n=50, left) and complex lesions (n=48, right).
CI, confidence interval; OR, odds ratio.
Serum MIF levels in ACS patients
ACS patients were divided into the following three groups: no complex lesion (n=12), one complex lesion (n=75), and multicomplex lesion (n=51) according to the number of angiographically complex coronary lesions. As shown in Figure 2, a significant positive correlation was found between increments in serum MIF levels and number of complex lesions (1.89 [0.66-2.30] ng/mL in the no complex lesion group, 2.68 [1.97-4.76] in the one complex lesion group, and 3.94 [2.35-5.36] in the multicomplex lesion group; p<0.05) in ACS patients.
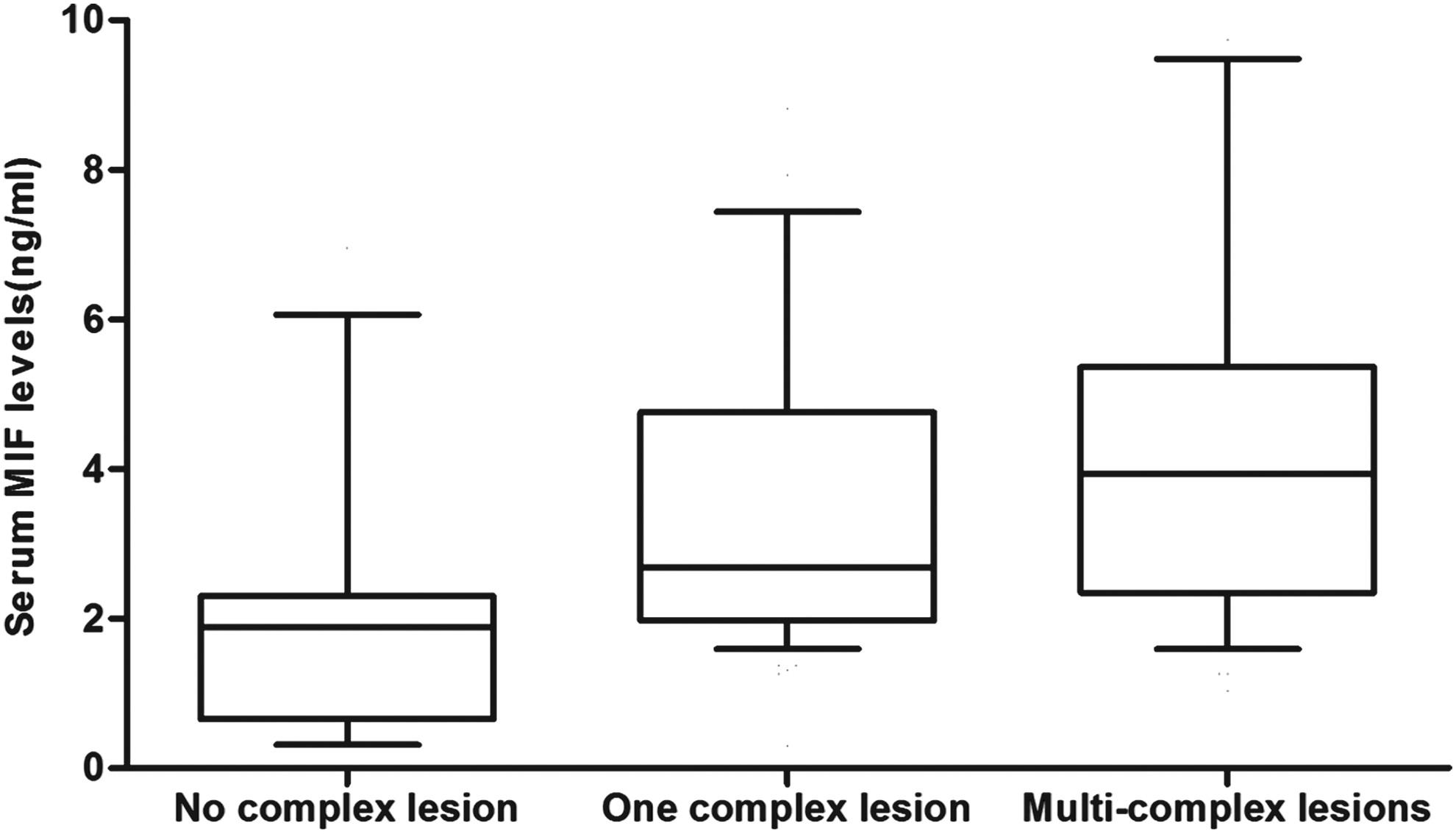
Box-and-whisker plot showing serum MIF levels in acute coronary syndrome patients with no (n=12, left), one (n=75, middle), and multicomplex lesions (n=51, right).
Discussion
We assessed the relationship between the MIF and angiographically complex coronary lesion in CAD patients. We revealed that a higher serum MIF level was an independent predictor of complex coronary lesion in SAP patients. Among ACS patients who had significantly higher serum MIF levels compared with SAP patients, those with multiple complex lesions had significantly higher MIF levels than those with single/no complex lesion. Our findings support a link between MIF activation and plaque instability in CAD patients.
It has been suggested that angiographically demonstrated complex lesions represent vulnerable plaques prone to disruption or truly disrupted plaques (Garcia-Moll et al., 2000). Various studies have confirmed that inflammatory and immunologic mediators may play a central role in plaque rupture (Drakopoulou et al., 2011). A variety of inflammatory markers and cytokines, including tumor necrosis factor (TNF)-α, interleukin (IL)-1β, IL-6, IL-12, and interferon (IFN)-γ, have been seen to be associated with vulnerable atherosclerotic plaque and their progression to the clinical syndromes (Dubey et al., 2008). MIF is a chemokine-like protein and, therefore, takes over many chemokine-like functions regarding the recruitment of inflammatory cells and the introduction of inflammatory cytokines such as TNF-α, IL-1β, and IL-8 (Muüller et al., 2012; Schmeisser et al., 2005). Besides, a significant correlation between MIF and matrix metalloproteinase (MMP) concentrations was found in a Chinese population (Yang et al., 2008). Local release of MMPs may degrade the extracellular matrix and further destabilize the atherosclerotic plaque (Johnson, 2007). Therefore, MIF holds the potential to be explored as a biomarker for complex lesions due to its pathophysiological role in the formation of vulnerable plaque.
Clinical stability in SAP patients is not necessarily indicative of atheromatous plaque stability, that is, absence of vulnerable plaque. SAP patients with vulnerable plaques have a high risk for ACS. In the present study, we demonstrated that about 49% of SAP patients were with angiographically complex lesions. This result is in accordance with previous studies (Hangartner et al., 1986; Zhao et al., 2011). We also revealed that SAP patients with complex lesions had significantly higher serum MIF levels compared to those with simple lesions. Moreover, multivariate logistic regression demonstrated that serum MIF levels were independently associated with the presence of complex coronary lesion in SAP patients after adjusting for potential confounders. These results concurred with several lines of evidence point to the role of MIF in vulnerable plaque and suggested that MIF in serum might be a potential biomarker for predicting the presence of vulnerable plaque in SAP patients.
In the present study, we found that ACS patients had significantly higher serum MIF levels compared with SAP patients. We further assessed the relationship between serum MIF levels and the number of complex lesions in ACS patients. We revealed that serum MIF levels elevated with the increment of complex lesions in ACS patients. The number of complex lesions may have prognostic importance because multiple complex lesions correlate with adverse clinical outcomes in ACS patients (Goldstein et al., 2000). Therefore, our results suggested that MIF in serum might also be a prognostic marker of disease progression in ACS patients.
In the interpretation of our data, it is necessary to consider several important limitations. Only serum MIF levels were assessed in our study. We did not measure the other proinflammatory cytokines in the same samples, which may provide more valuable information on the pathophysiological role of MIF signaling pathways in vulnerable plaque. The results of our research will also share the limitations of the cross-sectional design and a relatively smaller sample size. Indeed, we have evaluated an association and not a causal relationship or predictability. Besides, coronary angiography provides insufficient information regarding true lesion complexity. More advanced imaging techniques, such as virtual histology intravascular ultrasound, optical coherence tomography, and magnetic resonance image, are needed to further evaluate complex coronary lesions and to verify the association between MIF and vulnerable plaques.
In conclusion, our findings suggest that MIF in serum could be a potential biomarker for reflecting the presence and severity of angiographically complex coronary lesion in CAD patients. However, further studies in a prospective cohort with a large population are warranted to verify our findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.