
Abstract
Objective: To examine the association between apolipoprotein B (ApoB) XbaI polymorphisms (rs693) and coronary heart disease (CHD) risk among the Han Chinese population by systematically analyzing multiple independent studies. Methods: The Hardy-Weinberg equilibrium test was applied to check genetic equilibrium among genotypes for the selected literatures. The quality of the studies was assessed by using the NewcastleOttawa Scale. Power analysis was performed with Power and Precision V4 software. A fixed or random effect model was used on the basis of heterogeneity. Publication bias was quantified and examined with Begg's funnel plot test and Egger's linear regression test. The meta-analysis was performed by Stata 12.0 software. Results: A total of 10 eligible association studies were included in this meta-analysis, and the pooled sample consisted of 1195 CHD patients and 1178 health controls. No consistent inference regarding publication bias for the included studies was obtained by using the two above-mentioned methods. The pooled odds ratios (95% confidence intervals [CIs]) for X− versus X+ allele and X+X+ + X+X− versus X−X− genotype were 2.25 (1.40-3.62) and 2.21 (1.39-3.50), respectively. Conclusions: This meta-analysis indicated that ApoB XbaI allele confers a significant risk towards the development of CHD among the Han Chinese population.
Introduction
C
So far, the association between ApoB XbaI polymorphisms and CHD risk has been investigated by a number of case-control studies published in different countries. However, the conclusions from these studies are largely inconsistent. Particularly in China, the obvious inconsistent results across different studies were obtained, rendering interpretation of its genetic risk for Han Chinese people difficult and confusing. Most studies of Han Chinese population focused on the association of XbaI polymorphisms, a genetic variant of ApoB gene, with CHD risk, because it may play an important regulatory role for ApoB production.
Nevertheless, the association between XbaI polymorphisms and CHD susceptibility still remained unclear in Han Chinese population, with inconsistent findings across different studies. Since each single study was limited in adequate power and providing sufficient information for Han Chinese population, summarizing the results from these single studies for obtaining a consolidated and reliable conclusion regarding XbaI polymorphisms becomes essential. The aim of the meta-analysis was to integrate the findings from multiple studies to provide an overall assessment whether XbaI (rs693) polymorphisms is associated with CHD risk under the condition of enough large samples in a population of Han Chinese subjects.
Materials and Methods
Literature databases
Major electronic literature databases were systematically searched, which included MEDLINE database (www.ncbi.nlm.nih.gov/pubmed), Chinese VIP database (www.cqvip.com/), Chinese Wanfang database (wanfangdata.com.cn/), and China National Knowledge Infrastructure (CNKI) database (www-cnki-net.web.bisu.edu.cn/), up to April 2015, for all publications about the association between ApoB XbaI polymorphisms and CHD in Han Chinese population. The keywords, apolipoproteins B/ApoB, polymorphisms, and coronary artery disease/CHD, were searched in this study.
Selection criteria
Studies were selected according to the following inclusion criteria: case-control studies (either population based or hospital based ones), Chinese Han as the studied subjects, available genotypic and allelic data or summarized frequencies, and the diagnosis of CHD patients based on the 1979 WHO CHD Criteria. If there were multiple publications from the same study group, the most recent study was included in this meta analysis. Studies were excluded in the following situations. The study was a lecture, review, correspondence, or editorial letter. Studies without detail genotype frequencies were excluded. Hardy-Weinberg equilibrium (HWE) was checked for each eligible study and the studies whose healthy control groups failed HWE were excluded.
Quality assessment
The quality of the nonrandomized studies was assessed by using the NewcastleOttawa Scale, which is a star rating system (Stang, 2010; Wells et al., 2015). A full score is 9 stars, and a score range of 5-9 stars is considered to be high quality while a score range 0-4 is considered to be a poor quality (Ownby et al., 2006; Gong et al., 2015). The quality of studies was evaluated by several items: adequate definition of cases, representativeness of cases, selection of controls, definition of controls, control for the most important factor or the additional important factor, exposure assessment, same method of ascertainment for cases and controls, and nonresponse rate. Any disagreements on the NOS score of the studies were unified through a comprehensive reassessment by two reviewers.
Data extraction
Data of relevant studies was extracted by two reviewers independently with a standard data-collection form, including name of first author, year of publication, geographic region, genotype distribution for CHD patients and healthy control subjects, and p-values of HWE test in healthy control groups. When HWE in the controls was not reported in selected studies, an online program (www.pharmgat.org/IIPGA2/Bioinformatics/exacthwe) was used to test the HWE by chi-square test. Then, disagreements between reviewers were resolved through a group discussion so that a consensus was obtained.
Statistical analysis
We conducted our meta-analysis according to the PRISMA checklists (Supplementary Table S1). This meta-analysis was performed with Stata 12.0. Power analysis was performed using the Power And Precision V4 software. Heterogeneity among the studies was examined with χ2-based Q statistic (Lau et al., 1997). If there was statistically significant heterogeneity among studies (χ2 = 3.84; p < 0.05) (Rothwell and Robertson, 1997; Chu et al., 2012), a random effect model based on Dersimonian-Laird method was used to pool the data from different studies. Otherwise, a fixed effect model (Mantel-Haenszel method) (DerSimonian and Laird, 1986) was employed to analyze data. Odds ratios (ORs) with 95% confidence intervals (CIs) for risk allele or genotypes were calculated to assess the association between the XbaI polymorphisms and CHD risk. Then, publication bias was tested with Begg's funnel plot or Egger's linear regression test. Finally, a sensitivity analysis was conducted to evaluate the influence of each individual study.
Results
Characteristics of eligible studies
In total, 11 studies of the association between XbaI polymorphisms and CHD susceptibility in Han Chinese were identified. There were two studies (Ye et al., 1994, 1995) with data largely overlapped, thus one study (Ye et al., 1994) was excluded from this meta analysis. Then, 10 remaining studies were subjected to HWE test, and no study was excluded since they did not significantly deviate from HWE in healthy control group (p > 0.05). Hence, there were actually 10 studies (Ye et al., 1995; Huang et al., 1996; Shi et al., 1996; Li et al., 1997; Zhang et al., 2002, 2004; Su et al., 2002; Tang et al., 2007; Zhao et al., 2007; Huang and Xie, 2011) to be used in this meta-analysis, with a total of 1195 CHD patients and 1178 healthy control subjects. The detailed screening process was shown in Figure 1. The characteristics of the included studies were summarized in Table 1. Among these studies, all the subjects were from Chinese Mainland. One of the sources of controls was population-based, and nine were hospital-based. The mean age of all the subjects ranged from 43.2 to 60.0 years, and the gender was not evenly distributed in the 10 studies. Moreover, not all of the included studies were adjusted for covariates, such as total cholesterol, triglyceride, body mass index, and so on. As a result, the information for these covariates was not shown in Table 1. The quality of these studies was rated to be high according to the quality assessment scores calculated.
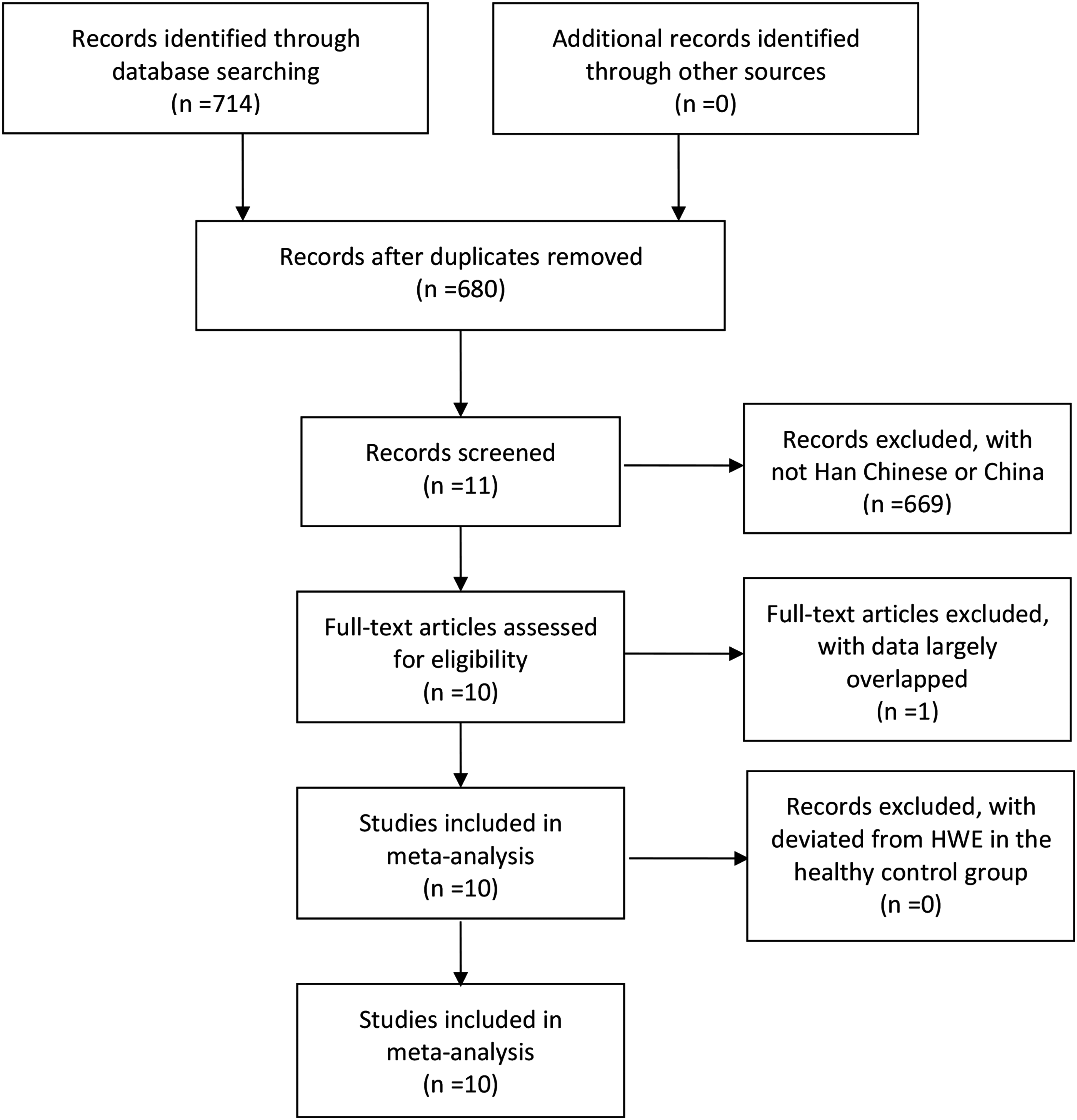
Flow chart of studies for inclusion in the meta-analysis.
pHWE, p-values of Hardy-Weinberg equilibrium test in healthy control groups, calculated by using a Chi-square test with Yates' continuity correction.
North includes Jilin, Shandong, and Beijing.
CHD, coronary heart disease.
Power analysis
Before this meta-analysis, a power analysis was conducted by using the Power And Precision V4 software to verify whether the included studies could offer adequate power (≥80%). With data provided by the 10 studies, the statistical power of 0.995 and 0.998 could be achieved for allelic and genotypic association analysis (under the allelic and dominant genetic model), respectively.
Association between XbaI polymorphisms and CHD susceptibility
According to the result of allelic heterogeneity analysis, there was statistical significance (p = 0.013) among the included studies under the allelic genetic model (X− vs. X+). Heterogeneity was observed in these studies. Therefore, a random effect model was selected for estimating the overall allelic risk. The pooled OR (95% CI) of XbaI (X− vs. X+ allele) is shown in Figure 2. The overall allelic OR (95% CI) was 2.25 (1.40-3.62) under the allelic genetic model, indicating that this X+ allele brought a modest-size allelic risk of CHD to Han Chinese population. Furthermore, heterogeneity among these studies were evaluated under the dominant mode (X+X+ + X+X− vs. X−X− genotype) for examining the association between genotypes and CHD. Statistical significance (p = 0.035) was revealed in the result of heterogeneity testing for the eligible studies. Therefore, a random effect model was also employed to merge data. Figure 3 shows the pooled OR (95% CI) for these studies under the dominant mode. The overall OR (95% CI) was 2.21 (1.39-3.50), also interpreted to be a modest-size risk of CHD.
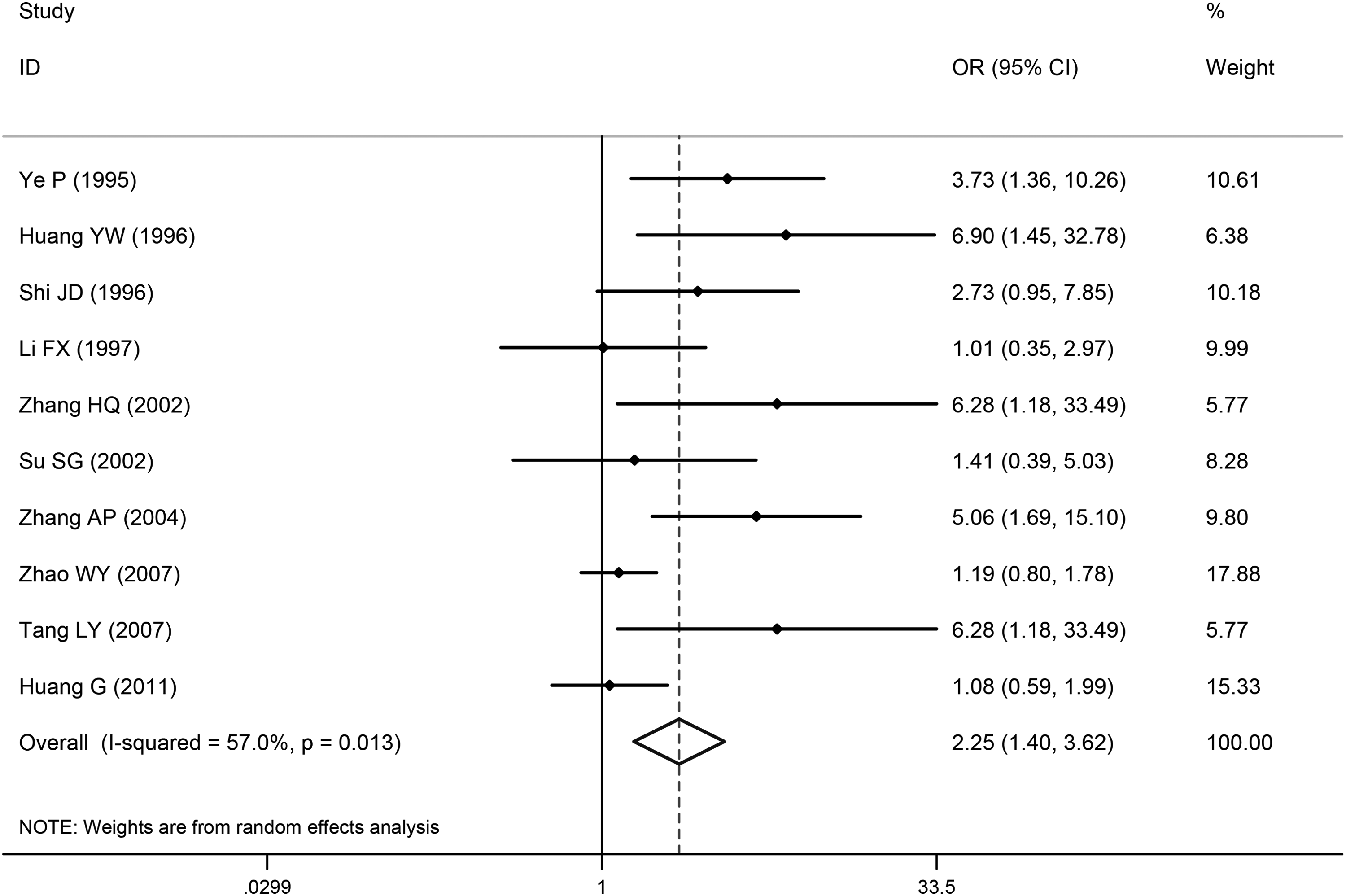
Forest plot of the association between CHD and XbaI for X− versus X+ allele. CHD, coronary heart disease; CI, confidence interval; OR, odds ratio.
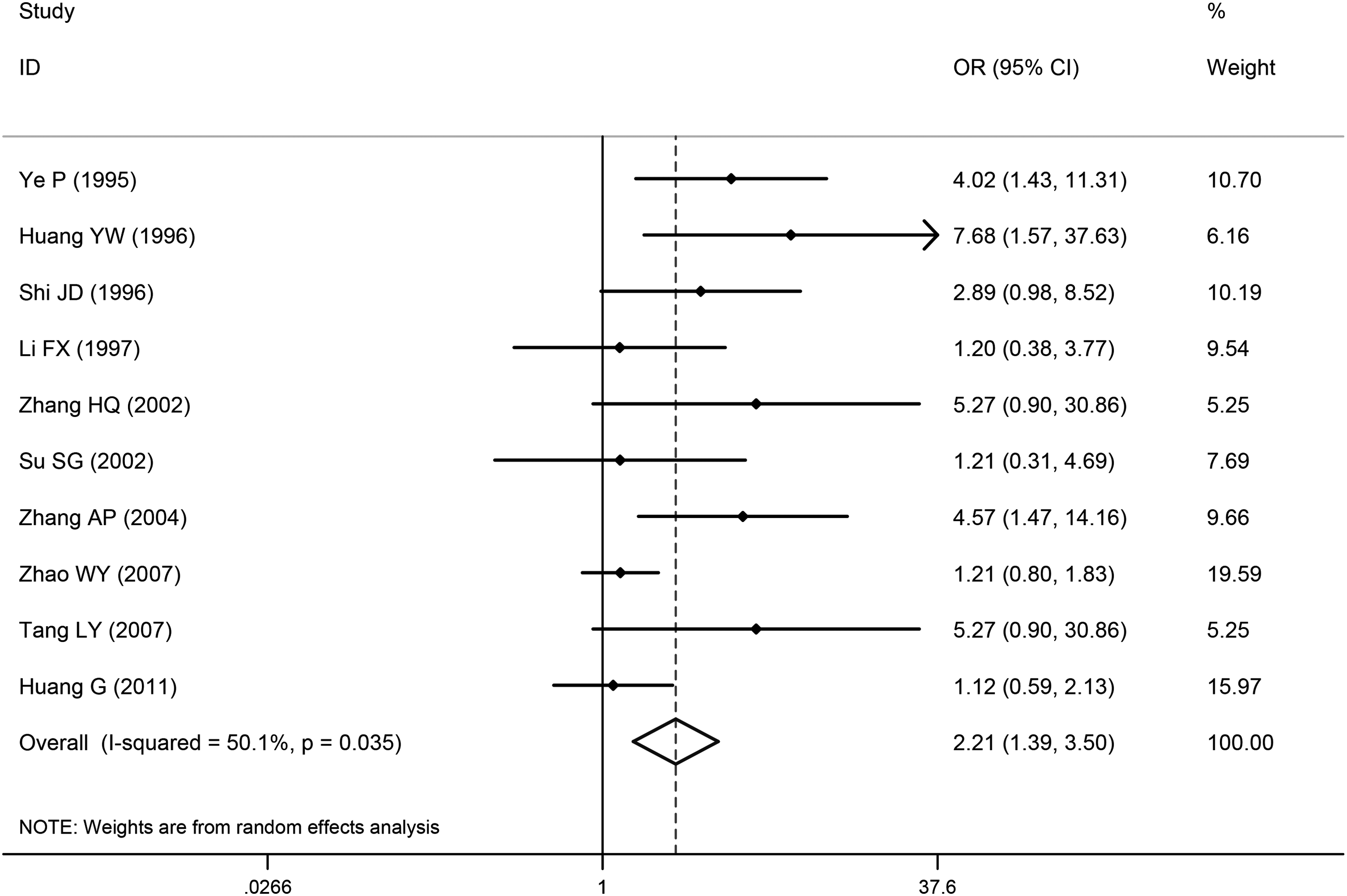
Forest plot of the association between CHD and XbaI for X+X+ + X+X− versus X−X− genotype.
Finally, to explore the geographical differences in the included Han Chinese samples, a stratification analysis by geographical areas (northern and southern China) was performed. Under the allelic genetic model (X− vs. X+) (Fig. 4), XbaI locus had a modest-size risk of CHD for both northern and southern Chinese, with ORs of 1.79 (95% CI: 1.08-2.97) and 3.90 (95% CI: 1.69-8.97), respectively. Similar result was also observed under the dominant genotypic mode (X+X+ + X+X− vs. X−X− genotype) (Fig. 5). The ORs (95% CIs) for the two geographical groups were 1.85 (1.13, 3.02) and 3.60 (1.48, 8.77), respectively. From both allelic and genotypic analyses, it can be seen that XbaI locus had a higher risk in Southern Chinese than Northern Chinese.
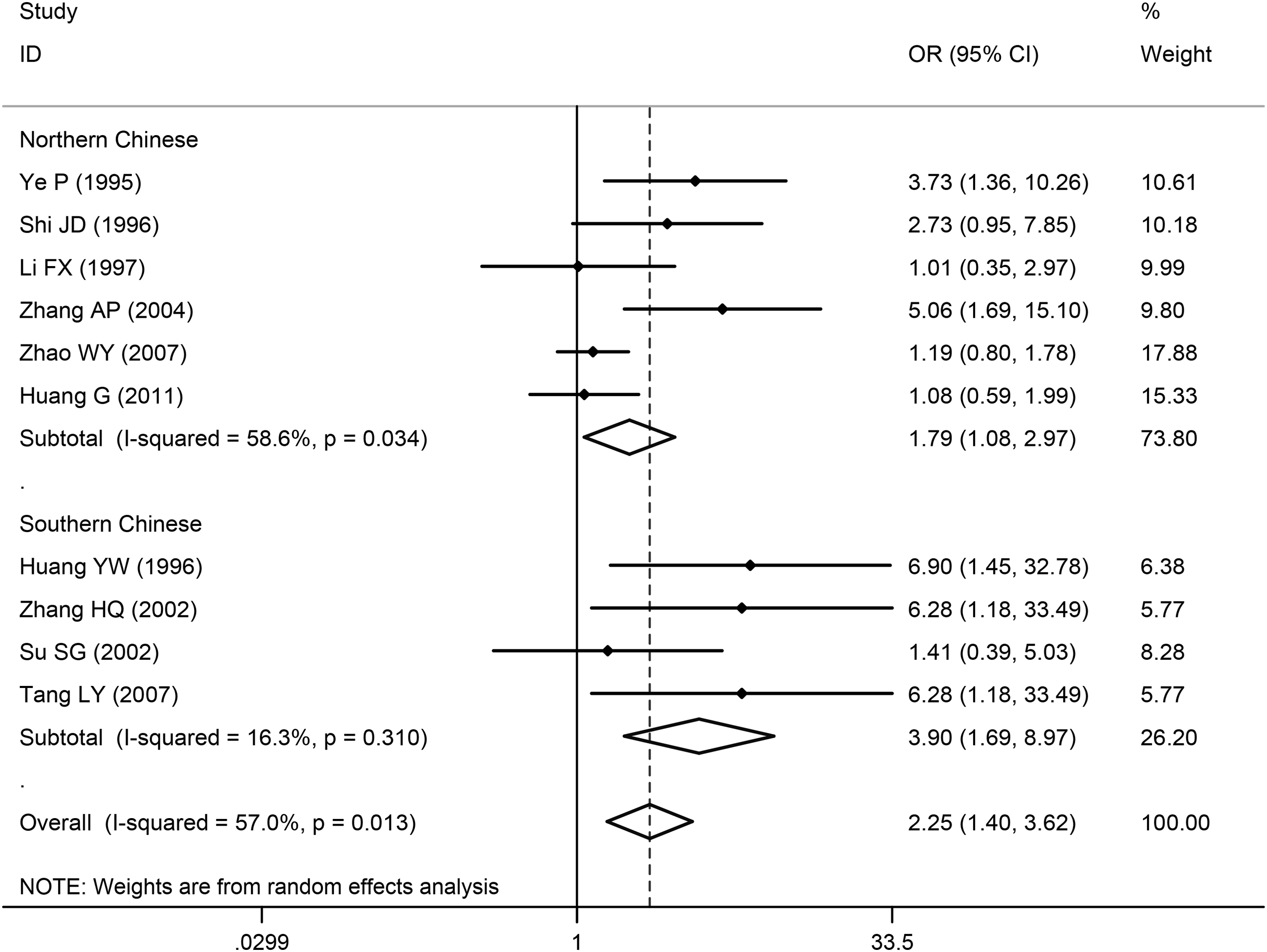
Subgroup analysis by geographical areas for the association between CHD and XbaI for X− versus X+ allele.
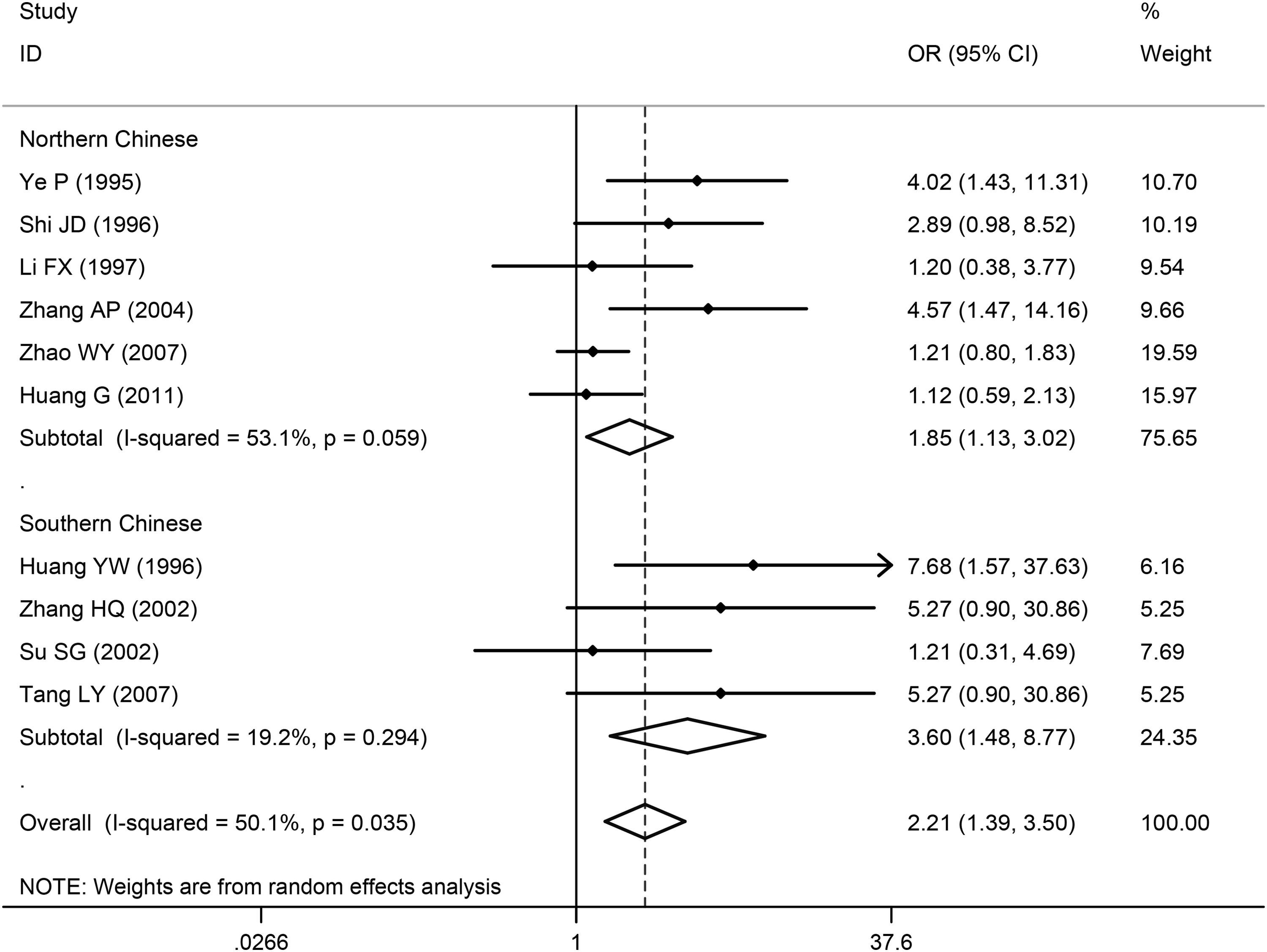
Subgroup analysis by geographical areas for the association between CHD and XbaI for X+X+ + X+X− versus X−X− genotype.
Publication bias
Publication bias was evaluated by Begg's funnel plot test and Egger's linear regression test. The funnel plots (Figs. 6 and 7) showed the association between CHD and XbaI for X− versus X+ allele and X+X+ + X+X− vs. X−X− genotype, respectively. The shapes of the two funnel plots were roughly symmetrical. The p-values for Begg's test of XbaI X− versus X+ allele and X+X+ + X+X− versus X−X− genotype were 0.128 and 0.128, respectively, indicating that no significant publication bias was observed in the included studies. Nevertheless, Egger's linear regression test gave an inconsistent inference, and the p-values for the allelic and genotypic association were 0.007 and 0.010, respectively. In short, the two tests commonly used for identifying potential publication bias produced contradictory results.
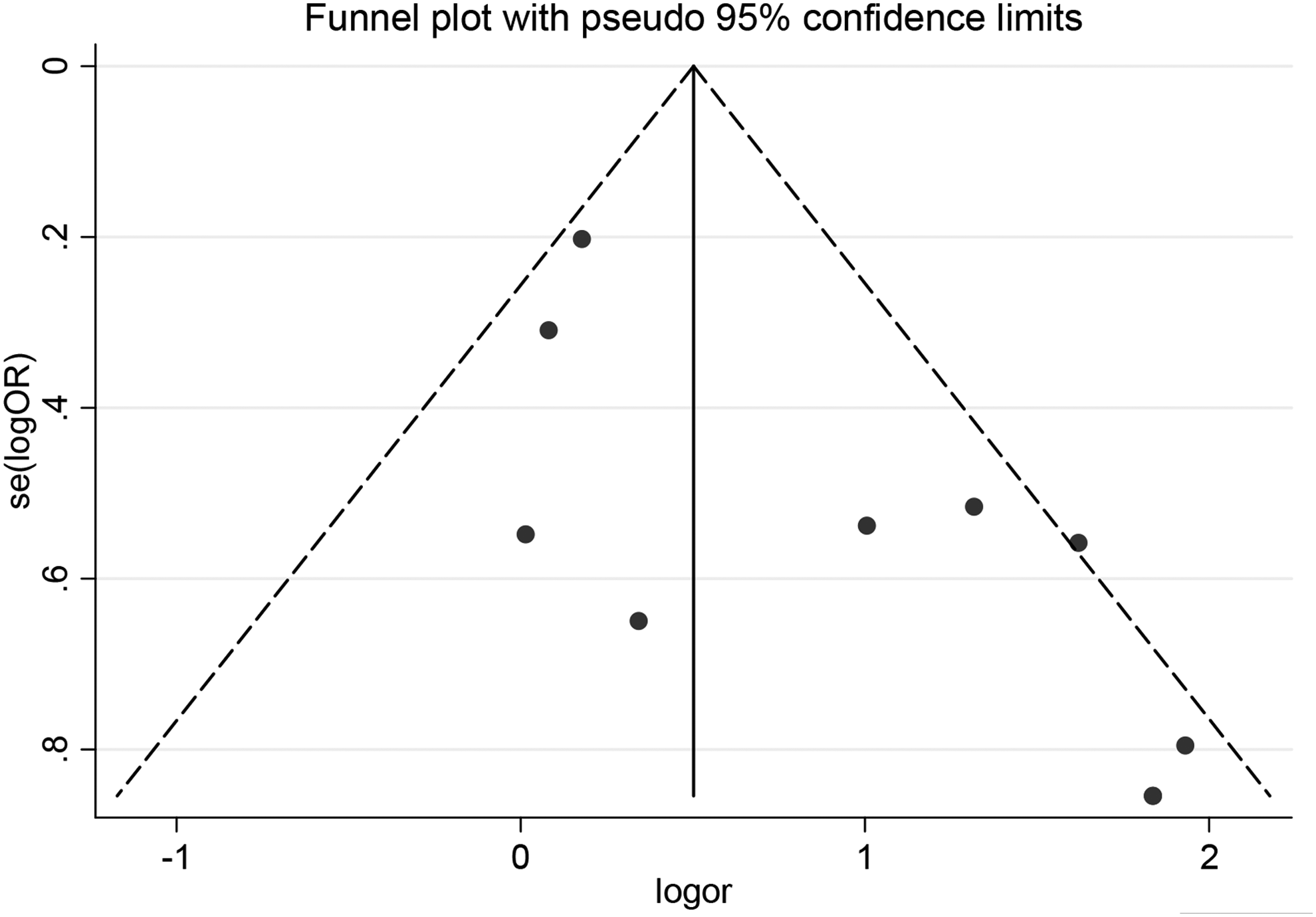
Funnel plot of the association between CHD and XbaI for X− versus X+ allele.
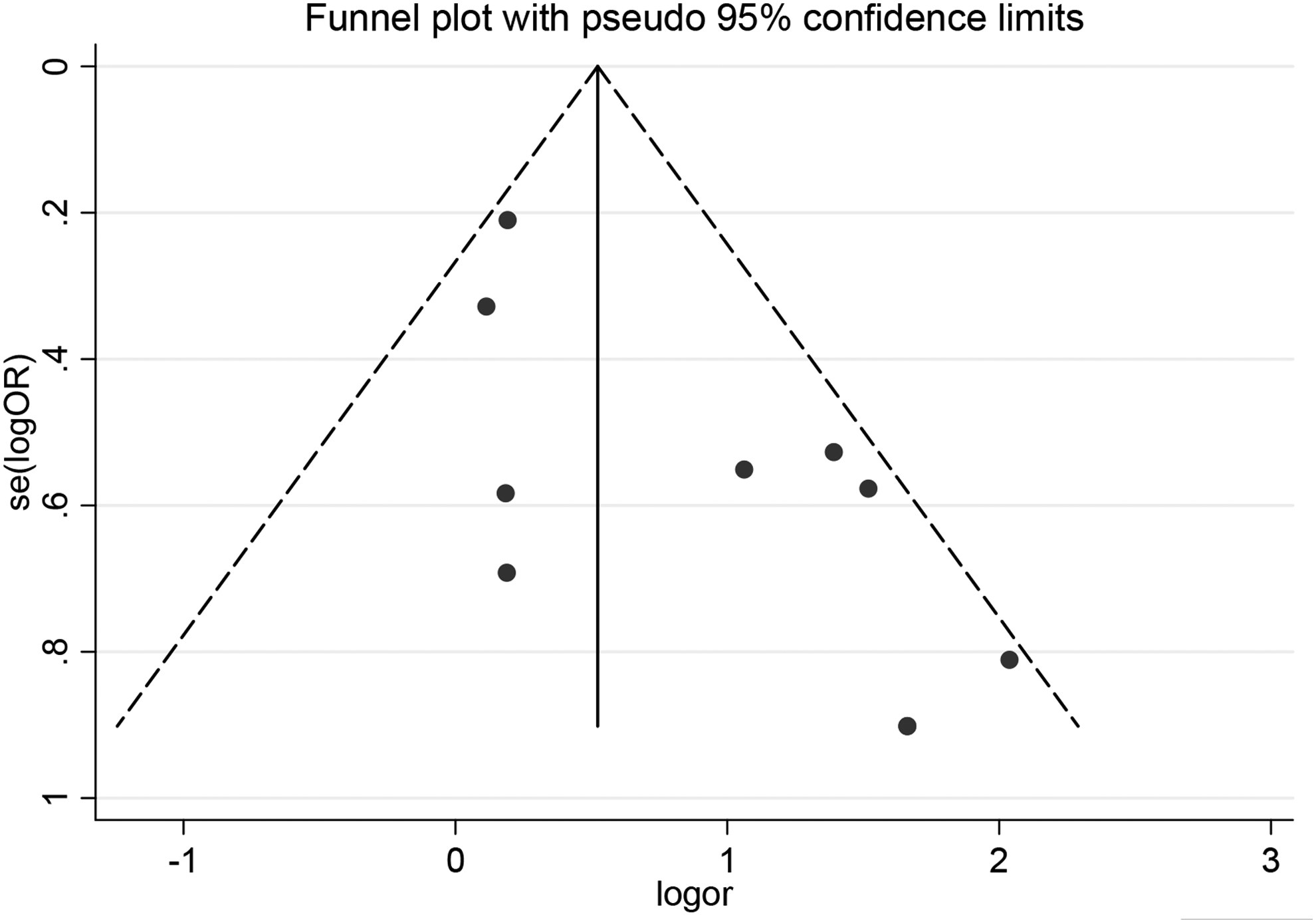
Funnel plot of the association between CHD and XbaI for X+X+ + X+X− versus X−X− genotype.
Sensitivity analysis
Finally, a sensitivity analysis was performed to explore individual study's influence on the pooled results by deleting one single study each time from the pooled analysis. The pooled ORs were compared with the overall OR under different genetic models. This sensitivity analysis demonstrated that none of the studies influenced the pooled OR greatly. The leave-one-out OR estimates ranged from 2.00 (1.26-3.21) to 2.60 (1.52-4.47) for X− versus X+ allele, and 1.98 (1.28-3.08) to 2.56 (1.51-4.34) for X+X+ + X+X− versus X−X− genotype, respectively, indicating that the pooled estimates of allelic and genotypic risks obtained in this study were statistically robust.
Discussion
ApoB gene, situated on human chromosome 2p24-p23, encodes the main apolipoprotein of chylomicrons and low-density lipoproteins. ApoB is an important structural component of all atherogenic lipoproteins (LDL, intermediate density lipoprotein [LDL], and very low density lipoprotein [VLDL]). Genetic variations of the ApoB gene may affect plasma and lipid levels, thus influencing atherogenesis (Nikolajevic Starcevic et al., 2014). Its function as a recognition signal for cellular binding and internalization of LDL particles by the ApoB receptor maintains cholesterol balance in the blood (Disterer et al., 2013; Corsetti et al., 2014). ApoB gene plays the key role in the accumulation of lipid and regulates the balance of cholesterol (Paulweber et al., 1990; Pencina et al., 2015). XbaI locus often has a mutation, which was considered to increase the susceptibility of atherosclerosis of coronary artery (Myant et al., 1989; Genest et al., 1990). The mutant is produced in the 2488 genetic codon on the ApoB gene exon 26, causing the change where glutamic acid is turned into diaminocaproic acid (ACC>ACT). Turner et al. (1995) reported that the protein structure of ApoB was transformed by this gene mutation, thus weakening the binding abilities between LDL and LDL receptors and affecting the catabolic rate of LDL, eventually leading to failure to remove ApoB and accumulation of LDL in the plasma. Consequently, such dyslipidemia would accelerate the development of atherosclerosis. Therefore, the results of this meta-analysis could be reasonably interpreted from these biological mechanisms.
Recently, the association studies between ApoB XbaI (rs693) polymorphisms and CHD susceptibility have been a hot focus in the field of genetics and a number of candidate-gene studies for CHD in Han Chinese population have been reported. However, sample sizes of these studies were relatively small, with patients from 26 to 499, with healthy control subjects from 33 to 487, hence offering limited power to infer the relationship between XbaI and CHD. By searching literature, we found that the findings regarding this association were with obvious discrepancies across different studies. Therefore, it is highly demanded to systematically evaluate the association of XbaI with CHD before translation of this genetic finding into clinical practice. Our intent was to clarify the relationship between the genetics of ApoB XbaI polymorphisms and CHD. Hence, we performed a systematic meta-analysis on all of the available case-control studies to estimate population-wide effects of XbaI polymorphisms on the risk of CHD.
To the best of our knowledge, this study was the first meta-analysis to comprehensively investigate the association between XbaI polymorphisms and CHD in Han Chinese population. A total of 10 case-control studies for Han Chinese were included in this meta-analysis, accumulating 1195 CHD patients and 1178 controls. This meta-analysis demonstrated a strong association between XbaI and CHD, and that the carriers of X+ allele have a modest-size risk for developing CHD. However, a worldwide meta-analysis of the studies of very different ethnical populations (divided into Czech Republic, Norway, Brazil, Germany, etc.), performed by Chiodini et al. (2003), indicated that XbaI polymorphisms was not associated with CHD risk in these racial divisions. This discrepancy suggests that the genetic effect of XbaI might be race-specific. In addition, a list of epidemiological and design factors (e.g., age, gender, life style, study design, or limited sample size) might explain the inconsistent results across different ethnical populations. In the data collection for this meta analysis, we also found one previously published GWAS for Han Chinese (Lu XF, et al., 2012). Unfortunately, the SNP (rs693) under this study was not in the top list for that GWAS, and the raw (or summary) data for this locus is not available for further analysis. Therefore, we did not include that GWAS in this meta analysis.
Furthermore, to avoid potential racial admixture, we strictly restricted to Han Chinese subjects in this study. All the study subjects were of clear Han Chinese ancestry. However, we should recognize that Han Chinese now live in a vast area, geographical and culture discrepancies might be additional factors causing genetic heterogeneity. To clarify this issue, we have further performed a stratification analysis. In the included samples, four studies were from southern China, and the remaining six from northern China. The stratification analysis by the two geographical areas indicated that XbaI locus had a higher risk in Southern Chinese than Northern Chinese. This geographical difference might be due to the very different culture and habits (including diet, living environment, personality, customs, and so on) in the two large geographic areas. In addition, there was less genetic communication between the two geographic areas, which may lead to some population stratification. In addition to the heterogeneity of geographical origin, other factors, such as gender, age, sample size, source of controls, genotyping method, the criteria of disease diagnosis, gene-gene and gene-environment interactions, might contribute to heterogeneity as well. Unfortunately, any stratified analysis regarding these potential confounding factors could not be performed in this meta-analysis due to limited number of studies and lack of size of samples.
Despite the considerable efforts to test for possible association between XbaI polymorphisms and CHD risk, several limitations should be acknowledged in this study. First, the results were based on unadjusted covariates (the potential confounding factors) due to lack of original data from the included studies, which further limited the evaluation of the effects of gene-environment interactions during the CHD development. Second, only single locus SNP (rs693) in ApoB gene was analyzed in this study, and whether additional genetic variants contribute to this gene remains unclear. Furthermore, the joint effects of certain genotypes were not considered, which may be more discriminating as risk factors than a single genotype. Third, the pooled sample size for this meta analysis might not be large enough, leading to a limited statistical power to estimate the effect of this locus. And fourth, regarding the publication bias for the studies included in this meta analysis, the two commonly used methods (Begg's funnel plot test and Egger's linear regression test) gave a quite different inference. The reasons for this inconsistency might be due to the limited sample sizes or the small number of the included studies. However, the further performed sensitivity analysis to evaluate the influence of individual studies demonstrated that the results from this meta analysis were statistically robust, and were unlikely to be influenced greatly by individual studies.
In conclusion, by systematically integrating 10 association studies for Han Chinese, with 1195 CHD patients and 1178 healthy subjects, we found that XbaI (rs693) polymorphisms were statistically significantly associated with CHD in Han Chinese population, suggesting that X+ allele at this locus increases the risk for the development of CHD in this population. However, more large-scale independent studies and population-based association studies are still needed to consolidate this finding. Additionally, for a complex disease like CHD, which is considered being the result of the complicated interplays between multiple genes, and gene-environment interactions, an extended and rational research is further needed to identify the genes and environmental triggers interacting with XbaI and the functional involvement of this locus resulting in the molecular pathogenesis of CHD.
Footnotes
Acknowledgments
This study was supported in part by the National Natural Science Foundation of China (Grant Nos. 31071166 and 81373085), Natural Science Foundation of Guangdong Province (Grant No. 8251008901000007), Science and Technology Planning Project of Guangdong Province (Grant No. 2009A030301004), Dongguan City Science and Technology Project (Grant No. 2011108101015), and the Guangdong Medical University Funds (Grant Nos. JB1214, XG1001, XZ1105, and STIF201122).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.