
Abstract
Background: Bone disease in rheumatoid arthritis (RA) is a complex phenomenon where genetic risk factors have been partially evaluated. In the present study, we aimed to evaluate the relationship between polymorphisms of the receptor activator of the nuclear factor kappa B (RANK) gene; the receptor activator of the nuclear factor kappa B ligand (RANKL) gene; and RANKL levels with osteoporosis in postmenopausal RA patients. Design and Methods: One hundred seventy-two postmenopausal female patients and 176 age- and sex-matched controls were enrolled in the study. All subjects were genotyped for the presence of RANK C575T (rs1805034) and RANKL C290T (rs9525641) gene polymorphisms. RANKL levels, bone mineral density (BMD), and biochemical markers were also obtained. Results: Women with the RANK CC genotype were significantly (2X) more likely to develop osteoporosis than those with the TT genotype (p = 0.024). A significant association was also observed between the RANKL 290TT genotype and both BMD and RANKL levels. In addition, individuals with the -290TT genotype were twice as likely to develop osteoporosis as those with the CC genotype (p < 0.001). Conclusions: Postmenopausal women with RA, carrying either the RANKL-290T allele or possessing the RANK 575CC genotype were more likely to develop osteoporosis. Moreover, our results suggested that the polymorphism 290C>T could be considered a risk factor for genetic susceptibility to osteoporosis and low BMD.
Introduction
R
Osteoporosis is more frequent in patients with RA than in the general population due to active systemic inflammation characterized by low bone mass and microarchitectural deterioration of bony tissue, with a consequent increase in bone fragility and susceptibility to fractures (lez-Alvaro et al., 2007).
The receptor activator of the nuclear factor kappa B ligand (RANKL)/receptor activator of the nuclear factor kappa B (RANK)/osteoprotegerin (OPG) pathway plays an important role in the regulation of bone remodeling and osteoclast differentiation and contributes to osteoclastic bone resorption in RA patients (Kotake et al., 2001). Ligation of RANK with RANKL can promote the formation, activation, and survival of multinucleated osteoclasts during normal bone remodeling and a variety of pathologic conditions. The genes encoding these products are well accepted as candidate genes that influence the development of osteoporosis (Boyce and Xing, 2008; Tu et al., 2015).
Tumor necrosis factor receptor superfamily, member 11a (TNFRSF11A), spans 61 kb at 18q22.1 and is a 12-exon gene-encoding RANK (Anderson et al., 1997). Tumor necrosis factor ligand superfamily, member 11 (TNFSF11), spans 58 kb at 13q14 and is an 8-exon gene encoding RANKL (Lacey et al., 1998).
In the present study, we aimed to evaluate the relationship between RANK C575T (rs1805034) and RANKL C290T (rs9525641) gene polymorphisms and biochemical markers with osteoporosis in postmenopausal RA patients.
Subjects and Methods
This study comprised 172 postmenopausal female patients (mean age 57.4 ± 9.3), who were referred to the outpatient clinics of the Rheumatology Department, Faculty of Medicine, Zagazig University. Characteristics of the RA patients are presented in Table 1. The inclusion criteria for this study were a diagnosis of RA according to the American College of Rheumatology criteria (Arnett et al., 1988).
Results are expressed as mean ± SD.
RA group versus control group, p > 0.01.
BMD, bone mineral density; CRP, C-reactive protein; DAS, disease activity score; ESR, erythrocyte sedimentation rate; HAQ, Health Assessment Questionnaire; RA, rheumatoid arthritis; RANKL, receptor activator of nuclear factor kappa B ligand; RF, rheumatoid factor.
Patients with thyroid or parathyroid gland disease, other endocrine disorders, serious liver or kidney disease, and radiological abnormalities were excluded from this study. Patients who received estrogen, androgen, anticonvulsant or anticoagulant therapies were also excluded. The control group involved 176 apparently healthy volunteers; their age and ethnic origin were matched with the patients and they were from the same geographical region. This study was approved by the institutional review boards. Signed informed consent documents were obtained from all participants included in this study.
Measurement of the clinical variables in RA patients
The demographic and clinical characteristics of the patients such as age, duration of RA disease, duration of morning stiffness, and tender/swollen joint count are presented in Table 1. Disease activity score (DAS) of every patient was assessed by the DAS equation (Prevoo et al., 1995). DAS-28 score greater than 5.1 is considered to be indicative of high disease activity, while that ranging from 5.1 to 3.2 is of moderate disease activity and finally that less than 3.2 is of low disease activity.
Functional assessment was carried out using the Health Assessment Questionnaire (HAQ). Scores from 0 to 1 represent mild to moderate disabilities and scores from 1 to 2 indicate moderate to severe disabilities, as well as the scores from 2 to 3 represent severe to very severe disabilities (Guillemin et al., 1994).
Measurement of laboratory tests in RA patients
RF was assayed by nephelometry, whereas value ≥20 IU/mL was regarded as a positive sign for RA. Serum RANKL and hs-CRP (C-reactive protein) were assayed by the high-sensitivity enzyme-linked immunosorbent assay, and the normal value of CRP for RA patients equals to <10 μg/mL of the laboratory tests.
DNA extraction and identification of genotypes
Genomic DNA was extracted from EDTA whole blood using a spin column method according to the protocol (QIA amp Blood Kit; Qiagen GmbH, Hilden, Germany).
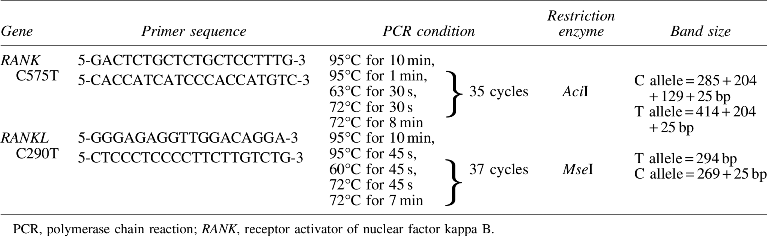
RANK C575T (rs1805034) and RANKL C290T (rs9525641) genotypes were identified in all subjects using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). RANK genotype was determined according to Zupan et al. (2010). RANKL (rs9525641) polymorphism was also determined according to Mencej et al. (2006). Primers were used for the PCR applying the specific cycling conditions (Table 2). The PCR was performed in a final volume of 25 μL containing 10 μL genomic DNA, 2 μL of each primer (Promega, Madison, WI), and 1× PCR mix (Taq PCR Master Mix Kit; Qiagen GmbH).
Measurements of BMD and radiological assessment
Bone density scanning, also called dual-energy X-ray absorptiometry, is used to measure the bone mineral density (BMD). The threshold for establishing a diagnosis of osteoporosis was based on the World Health Organization (WHO, 1994) definition, that is, BMD ≥ 2.5 standard deviation (SD) below the young adult mean (or T-Score ≤ −2.5). Osteopenia was defined as BMD between 1 and 2.5 SD below the young adult reference mean (T-Score ≤ −1.0 and > −2.5).
Anteroposterior plain radiographs of both hands and wrists were performed and scored using the Sharp method (Sharp et al., 1985), for the presence or absence of joint erosion.
Statistical analysis
The results for continuous variables are expressed as mean ± SD. The means of the three genotype groups were compared in a one-way analysis of variance (ANOVA). Genotype frequencies were tested for Hardy-Weinberg equilibrium, and any deviation between the observed and expected frequencies was tested for significance using the chi-square (χ2) test. The statistical significances of differences in frequencies of variants between the groups were tested using the χ2 test. In addition, the odds ratios (ORs) and 95% confidence intervals (CIs) were calculated as a measure of the association of the RANK and RANKL polymorphic sites with RA and osteoporosis. A difference was considered significant at p < 0.05. All data were evaluated using SPSS version 10.0 of Windows.
Results
Basic characteristics of the study subjects
The mean age of cases and controls was 57.4 ± 9.3 and 55.1 ± 3.8 years, respectively. In postmenopausal women with RA, the mean disease duration was 10.6 years, the mean ± SD rheumatoid factor concentration was 77.5 ± 79.3 IU/mL, and the mean ± SD CRP and the erythrocyte sedimentation rate (ESR) were 16.2 ± 14.8 μg/mL and 47.5 ± 32.9, respectively. High serum level of RANKL (10.83 ± 8.9) and BMD (2.18 ± 0.8) were observed in RA patients compared to controls. The mean DAS value was 4.4, while the mean HAQ disability index was 1.5. Sixty-eight percent of patients had RF positive, and 34% of them had erosion (Table 1).
Distribution of RANK and RANKL genotypes and alleles in RA patients and control groups
The genotype frequencies of the RANK and RANKL were in agreement with Hardy-Weinberg equilibrium in all groups (Table 3). Carriers of the T allele of RANK gene were significantly more likely to have RA (OR = 1.3, 95% CI = 1-1.8, p = 0.039). No significant difference in the frequencies of the RANKL genotype was observed between RA and control groups.
CI, confidence interval; OR, odds ratio.
Association of RANK and RANKL polymorphisms with osteoporosis in RA patients
RA patients with RANK 575CC genotype were more likely to develop osteoporosis compared to those with 575TT genotype (OR = 2.8, p = 0.024) (Table 4). Subjects carrying RANKL 290TT genotype were likely to develop osteoporosis two times more than those with 290CC genotype (OR = 2.5, p = 0.019).
Effect of RANK and RANKL gene polymorphisms on study parameters
Postmenopausal rheumatic women carrying 575TC genotype of the RANK gene showed a significant increase in disease activity represented by DAS-28 and ESR compared to 575CC genotype (Table 5). Rheumatic patients carrying RANKL 290TT genotype showed a significant increase in the levels of RANKL and BMD compared to patients carrying 290CC genotype. Meanwhile, patients carrying 290TC genotype had higher DAS-28 score compared to patients carrying 290CC genotype.
Results are expressed as mean ± SD.
Significant difference from CC of RANKL C290T.
Significant difference from CC of RANK C575T.
Correlation between RANKL level and clinical and laboratory findings of the rheumatoid patients
Serum RANKL levels showed positive correlation with RF (r = 0.18, p = 0.03), number of swollen joints (r = 0.17, p = 0.045), and DAS (r = 0.2, p = 0.017) (Table 6). In addition, positive correlation was found between RANKL level and BMD (r = 0.25, p = 0.003).
Discussion
Osteoporosis is more frequent in RA patients than in the healthy population. In patients with long-standing RA, the occurrence of osteoporosis ranges from 19% to 32% in the spine and from 7% to 26% in the hip (Maruotti et al., 2014). Osteoporosis in patients with RA is a silent disease that evolves in parallel with the underlying disease and gives a sign to exist only after the fracture (Xu et al., 2012). Osteoporosis is a polygenetic disease, where a growing number of variations in genes involved in bone metabolism and bone matrix proteins have been proven to be regulators of bone mass.
RANKL is the key cytokine involved in differentiation of osteoclasts from their precursor cells and promotes increased activity and survival of osteoclasts (Kong et al., 1999). RANK is the only receptor for RANKL and it is capable of initiating osteoclastogenic signal transduction upon binding of RANKL (Trouvin and Goeb, 2010). RANK is essential for osteoclastogenesis and RANK-deficient mice exhibit severe osteopetrosis (Kim et al., 2000).
Interestingly, the frequency of the C allele of the RANK C575T was lower in the Egyptian healthy controls (38.4%) compared with the Caucasian population (51%) and higher compared with the Korean population (33%) (Choi et al., 2005).
In this study, we have demonstrated that subjects carrying RANK 575T allele are more likely to develop RA than those carrying other allele. In the previous study, no significant association was found between RANK polymorphisms and susceptibility to RA (Assmann et al., 2010).
Postmenopausal rheumatic patients carrying 575CC genotype are more likely to develop osteoporosis than those who do not possess this genotype (Table 4). Meanwhile, there is no significant association between RANK gene polymorphism (rs1805034) and both of serum RANKL level and BMD (data not shown).
RANK polymorphism (rs1805034) was found to be associated with BMD in men, but not with that of women in the Chinese population (Hsu et al., 2006). On the contrary, RANK polymorphism was not associated with BMD in Korean postmenopausal women (Choi et al., 2005; Koh et al., 2007) and Slovenian population of Caucasian origin (Zupan et al., 2010).
Shang et al. (2013) proved the associations between rs1805034 in the RANK gene and BMD in Chinese perimenopausal women, whereas a significant difference was found between TT and TC/CC, which suggests that single nucleotide polymorphism (SNP) rs1805034 could be more important in relation to the peak bone mass attained in young adulthood than in regulating the extent of bone loss after menopause. However, these differences were not considered to be relevant as no influence on BMD was found in total, perimenopausal, or postmenopausal women.
Our study showed that there was no significant difference in the frequencies of the RANKL genotype observed between the RA group and control group (Table 3). These results were consistent with the previous findings (Meadeb, 2009; Assmann et al., 2010).
In contrast to our results, the C allele of RANKL rs9525641 in the promoter was associated with earlier age at the onset of RA in European and American patients (Wu et al., 2004; Tan et al., 2010).
In our study, patients carrying -290TT genotype of RANKL gene were more likely to develop osteoporosis (Table 4). Moreover, patients carrying TT genotype had significantly greater BMD than those with CC genotype (Table 5). This result was in accordance with several studies (Mencej et al., 2006, 2008, 2009). In addition, patients carrying -290TT genotype showed a significant increase in the levels of RANKL compared to the other two genotypes. In contrast to our results, Mencej et al. (2008) found no significant differences in the frequencies of -290C>T of the RANKL gene promoter between nonosteoporotic and osteoporotic postmenopausal women. These results suggested that the polymorphism -290C>T could be considered a risk factor for genetic susceptibility to osteoporosis.
In our study, we had found an increase of serum RANKL in RA patients compared to controls (Table 1). These results were in agreement with previous studies (Ziolkowska et al., 2002; Vanderborght et al., 2004; Xu et al., 2012).
Eghbali-Fatourechi et al. (2003) reported that upregulation of RANKL in bone marrow cells can promote bone resorption, providing biological support for a functional role of RANKL in bone remodeling. As RANKL induces osteoclastogenesis, higher levels of RANKL could lead to increased bone loss and higher BMD.
The present study demonstrated that serum RANKL levels showed a positive correlation with BMD (Table 6). These results were consistent with the findings of the previous studies (Oelzner et al., 2007; Xu et al., 2012). A Korean and a Chinese study failed to reveal an association between RANKL and BMD. The reason for this discrepancy is unclear, but it may be due to ethnic differences (Liu et al., 2010).
In postmenopausal rheumatic women, there was a significant correlation between serum RANKL level and disease activity and severity parameters such as DAS-28 and RF (Table 6). This result is in agreement with previous studies (Hofbauer et al., 1999; González-Alvaro et al., 2007).
Hofbauer et al. (1999) reported that the serum levels of RANKL were related to disease activity because of the presence of high levels of RANKL in the inflamed joint of patients with RA, which were produced by infiltrating activated cells and resident synoviocytes under stimulatory effects of proinflammatory cytokines on the expression of RANKL.
Sequence variations in the promoter region of RANKL gene could result in altered binding of the various transcription factors and could thus affect the expression of RANKL gene. Any change in RANKL expression in the bone microenvironment may influence the RANKL/OPG ratio, which is associated with the bone resorption index and femoral neck fractures (Tsangri et al., 2004).
There were some potential limitations to this study. First, no data on fragility fractures and the quality of bone were available for the analysis. Second, a relatively small sample size allowed only a limited power to detect individual effects and interactions. By expanding the sample size, we could further investigate genetic influence of the studied genes on the development of osteoporosis. Third, in our study, no data on external factors that influence BMD such as dietary calcium and vitamin D intake, smoking habits, and physical activity were collected and analyzed. However, our group was ethnically homogenous, and the participants originate from the same environment and have similar lifestyles.
Conclusion
In postmenopausal women with RA, patients carrying RANKL-290T allele were more likely to develop osteoporosis than those carrying -290C allele. In addition, patients carrying RANK 575CC genotype were more likely to develop osteoporosis compared to those with 575TT genotype. Moreover, these data suggest that patients carrying 290TT genotype are significantly associated with RANKL level in blood, which could contribute to the bone loss characteristic and the generation of osteoporosis in these patients. These results suggested that the polymorphism 290C>T could be considered a risk factor for genetic susceptibility to osteoporosis and low BMD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.