
Abstract
Objective: To investigate the potential prognostic roles of polymorphisms in the X-ray repair cross-complementing group 1 (XPCC1), xeroderma pigmentosum group D (XPD) and excision repair cross-complementing group 1 (ERCC1) genes for patients with hepatocellular carcinoma (HCC) receiving transcatheter arterial chemoembolization (TACE). Methods: Clinical data and blood samples from 308 HCC patients receiving TACE were collected between January 2010 and December 2013. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RLFP) analyses was used to determine the genotypes of the XPCC1 (rs25487), XPD (rs13181) and ERCC1 (rs11615) genes. The relationships between the genotypes and the efficacy of TACE treatment were analyzed. Results: The XRCCI rs25487 polymorphism was associated with a favorable prognosis in HCC patients receiving TACE (p = 0.006), and patients carrying variant genotypes (A/A + G/A) were associated with significantly reduced risk of death compared with those with the wild genotype (G/G) (HR = 0.556; 95% CI = 0.354−0.874). These findings were supported by Kaplan-Meier survival curve analysis showing that median survival time for patients with A/A + G/A genotypes was significantly longer compared with those with the G/G genotype (11.2 month vs. 8.0 months; log rank p = 0.006). Stratified analyses revealed that A/A + G/A genotypes of XRCC1 rs25487 are associated with significantly reduced risk of death compared with the G/G genotype in patients grouped by tumor size, portal vein tumor thrombus (PVTT), alpha-fetoprotein (AFP) and TNM stage (all p < 0.05). The ERCC1 rs13181 and XPD rs11615 polymorphisms were not predictive of clinical outcome for HCC patients receiving TACE (both p > 0.05). Conclusion: The XRCC1 rs25487 polymorphisms are prognostic for HCC patients receiving TACE. The ERCC1 and XPD polymorphisms had no relationship to the clinical outcomes.
Introduction
A
The 5-year survival rate of HCC patients is 30-40% after curative resection, and the poor prognosis is largely due to increased tumor recurrence (Bouchard-Fortier et al., 2011). Transcatheter arterial chemoembolization (TACE) is a therapy recommended for intermediate-stage HCC patients to eradicate tumor and preserve liver function by arterial embolization (Peng et al., 2013). TACE limits tumor growth and tumor dissemination, however, its efficacy on the overall survival is yet to be conclusively demonstrated (Bouchard-Fortier et al., 2011).
DNA repair genes encode proteins involved in DNA repair to fix the damages caused by a variety of DNA-damaging agents, and thus ensuring genome integrity. DNA repair can proceed by four distinct pathways involving proteins that are both common and unique to these pathways: nucleotide excision repair (NER), base excision repair (BER), single-strand break repair (SSBR), and double-strand break repair (DSBR) (Yao et al., 2014). X-ray repair cross-complementing group 1 (XRCC1) protein encoded by the XRCC1 gene is mainly associated with the core activities in SSBR and BER pathways through directly regulating multiple DNA polymerases, such as DNA polymerase β, poly-ADP-ribose polymerase, and DNA ligase III.
On the other hand, xeroderma pigmentosum group D (XPD) and excision repair cross-complementing group 1 (ERCC1) proteins participate in NER pathway by stimulating the excision of the damaged DNA base (van Huis-Tanja et al., 2014; Yao et al., 2014). XRCC1, XPD, and ERCC1 play crucial roles in DNA repair pathways, and single-nucleotide polymorphisms (SNPs) of the three genes affect the long-term survival in cancer patients receiving chemotherapy and surgery due to the loss of DNA repair capacities (Zou and Yang, 2012; Qiu et al., 2013; Yamada et al., 2013; Wu et al., 2014).
More specifically, XRCC1 gene is located on chromosome 19 (19q13.2), and rs25487 (G/A substitution at position 28,152 on exon 10) was demonstrated with a higher risk of HCC (Li et al., 2014; Wu et al., 2014; Xu et al., 2015). XPD is a gene located at chromosome 19q13.3 and encodes a type of NER enzyme, has high variant frequencies in exon 23 (rs13181, codon 751 A/C), which may contribute to increased risk of HCC, especially in Asian populations (Flejter et al., 1992; Peng et al., 2014; Yang et al., 2015). ERCC1 rs11615 is a common SNP in the coding region, and ERCC1 overexpression is associated with chemosensitivity to cisplatin resistance in HCC specimens and cell lines, and may be correlated with survival rates in HCC patients, but without further investigations regarding the association of XRCC1 rs25487, XPD rs13181, and ERCC1 rs11615 SNPs with the prognosis of HCC patients (Ueda et al., 2011; Bassullu et al., 2012).
Therefore, our study was aimed to evaluate the roles of XRCC1 rs25487, XPD rs13181, and ERCC1 rs11615 SNPs in predicting the outcome of HCC patients receiving TACE.
Materials and Methods
Study subjects
A total of 308 patients with HCC were recruited from the Linyi People's Hospital affiliated to the Shandong University between January 2010 and December 2013. HCC diagnosis was based on the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology (Benson et al., 2009). Patients were enrolled if they: had a tumor size >5 cm or multiple tumors and could not be treated by radical operation; could not be treated by surgical resection if tumor is located around the gallbladder or around the hepatic hilar region great vessels; had poor liver function reserve although the tumor size is less than 5 cm, and did not have the condition of surgical operation; had no indication for surgery, previous history of other cancers, or blood transfusion and any antitumor therapy before blood collection. Patients were excluded if they had severe liver and renal insufficiency; severe jaundice; complete embolization of the main trunk of the portal vein; severe ascites; severe bleeding tendency; iodine allergy; severe hypertension; ineffective control of heart disease and diabetes.
Detailed clinical information of the enrolled HCC patients was collected through reviewing medical record or consulting with doctors in charge, including the date of diagnosis, HBV, tumor number, tumor size, PVTT, Child-Pugh score, serum AFP level, and TNM stage. According to the treatment, patients receive TACE as the first-line treatment and subsequent treatment; or patients receive TACE as the first-line treatment and gamma knife, radiofrequency ablation (RFA), etc. as subsequent treatments without receiving surgical treatment. After approval by the Ethics Committee of the Linyi People's Hospital affiliated to the Shandong University, written informed consents were obtained from the study subjects.
Follow-up information
The follow-up information was collected after 3-43 month hospital discharge and at every 3-month intervals. The survival time was defined from the time of first-line treatment to death or the last follow-up. Clinical data, including the treatment of patients, imaging examination, and serological test results, etc. were obtained by medical record review or direct consultation, and the registration form of HCC patients was also supplied after follow-up. All of the above information were recorded digitally and checked carefully for accuracy and completeness.
Specimen collection
Fasting peripheral venous blood (5 mL) was collected early in the morning, and put in ethylenediaminetetraaceticacid (EDTA) tubes and stored at 4°C. The Whole Blood Genomic DNA Isolation Kit (Tiangen Biotech Co. Ltd.) was used for DNA extraction. Accurate and detailed information about the blood sample collection was recorded and the basic information of all subjects was registered.
SNPs analyses
The SNP genotyping in three key genes, XRCC1, ERCC1, and XPD, involved in DNA repair was studied using polymerase chain reaction-restriction fragment length polymorphism according to the manufacturer's instructions (Matullo et al., 2001). The PCR primers were designed by Primer Premier 5.0 software (PREMIER Biosoft International) and were synthesized by Shanghai Sangon Biological Engineering Technology and Service Co. Ltd. Primer sequences and their lengths are listed in Table 1.
SNP, single nucleotide polymorphism; XRCC1, X-ray repair cross-complementing group 1; XPD, xeroderma pigmentosum group D; ERCC1, excision repair cross-complementing group 1.
The 25 μL-PCR system contained 100 ng genomic DNA, 125 ng primers, 12.5 μL 2× Taq Master Mix (Tiangen Biotech Co. Ltd.), and 9.5 μL dH2O. The PCR protocol on a Light Cycler (LC480) (Roche Diagnostics) for XRCC1 rs25487, ERCC1 rs11615, and XPD rs13181 SNPs was as follows: an initial denaturation step (94°C for 2 min) and 30 cycles of denaturation (94°C for 30 s) followed by annealing and extension steps (XPD 60°C, XRCC1 62°C, ERCC1 58°C for 30 s, 72°C for 45 s), and a final extension (72°C for 7 min). The PCR products were digested at 37°C overnight with restriction enzymes, and subsequently separated by electrophoresis in 0.3% agarose gels.
The 485 bp PCR product of XRCC1 rs25487 polymorphism was digested with Pvu II (TaKaRa Bio, Inc., Bao Biological Engineering (Dalian) Co., Ltd.): wild-type GG homozygote (485 bp), variant GA heterozygote (485 bp, 396 bp, 89 bp), and variant AA homozygote (396 bp, 89 bp). The 290 bp PCR product of XPD rs13181 polymorphism was digested with Pst I (TaKaRa Bio, Inc., Bao Biological Engineering (Dalian) Co., Ltd.): wild-type AA homozygote (290 bp, 146 bp), variant AC heterozygote (290 bp, 227 bp, 146 bp, 63 bp), and variant CC homozygote (227 bp, 146 bp, 63 bp). The 208 bp PCR product of ERCC1 rs11615 was digested with Bsrd I (TaKaRa Bio, Inc., Bao Biological Engineering (Dalian) Co., Ltd.): wild-type TT homozygote (128 bp), variant CT heterozygote (208 bp, 128 bp), and variant CC homozygote (208 bp).
Statistical analysis
Data analysis was performed using SPSS software for Windows (Version 18.0; SPSS). Measurement data were tested by χ2 test. Enumeration data were presented by percentage or rate. The relative association was estimated by hazard ratio (HR) with 95% confidence intervals (CIs) using Cox's proportional hazards regression model. Univariate analysis was used to observe prognostic factor for HCC patients receiving TACE. Survival-free curves were estimated by the Kaplan-Meier technique and compared with use of the two-sided log-rank test. p less than 0.05 was considered statistically significant.
Results
Characteristics of study populations
Among the 308 enrolled HCC patients (median age, 53 years; range, 25-80 years), 268 patients were men, 269 patients had HBV-associated HCC, 213 patients had cirrhosis, Child-Pugh A in 283 patients, tumor size ≥5 cm in 226 patients, tumor number ≥2 in 117 patients, PVTT in 95 patients, AFP ≥200 μg/L in 169 patients, and TNM stage I + II and III in 113 patients and 195 patients, respectively. The 272 patients received TACE as the first-line treatment and subsequent treatment; 36 patients received TACE as the first-line treatment and gamma knife, and RFA radiotherapy as the subsequent treatment. Overall, the median survival time (MST) of all patients was 10.7 months. The median follow-up time was 11 months (range, 3-43 months). There were 216 deaths caused by HCC in the last follow-up (Table 2).
HBV, hepatitis B virus; PVTT, portal vein tumor thrombus; AFP, alpha-fetoprotein; TNM, tumor-node-metastasis; TACE, transcatheter arterial chemoembolization.
Associations of XRCC1, ERCC1, and XPD SNPs with prognosis of HCC in patients receiving TACE
The genotype distributions of studied polymorphisms were consistent with Hardy-Weinberg predictions in the study subjects confirmed by a goodness of fit test (all p > 0.05).
The results of the Cox's proportional hazards regression model showed that XRCCI rs25487 polymorphism was associated with better prognosis of HCC in patients receiving TACE (p = 0.006) and the variant genotypes (A/A + G/A) significantly reduced the risk of death of HCC patients compared with wild genotype G/G (HR = 0.556; 95% CI = 0.354-0.874). Polymorphisms of XPD rs13181 and ERCC1 rs11615 had no relevance to the prognosis of HCC in patients receiving TACE (both p > 0.05) (Table 3). Kaplan-Meier survival curves showed that the MST in patients with XRCC1 variant genotypes (A/A+G/A) was lengthened compared to those with wild genotype GG (11.2 month vs. 8.0 months; log rank p = 0. 006) (Fig. 1).
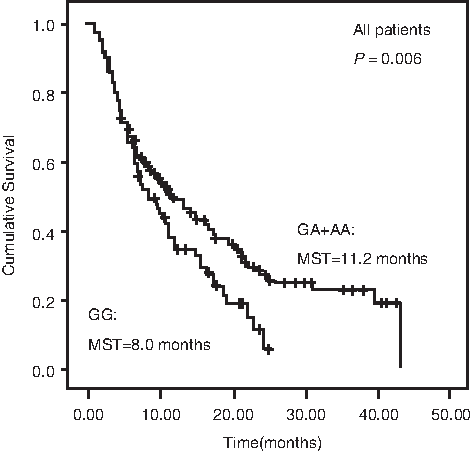
Kaplan-Meier survival curves of XRCC1 rs25487 single-nucleotide polymorphism in HCC patients. Kaplan-Meier survival curves showed that the MST in patients with XRCC1 variant genotypes (A/A+G/A) was lengthened compared to those with wild genotype GG. HCC, hepatocellular carcinoma; MST, median survival time; XRCC1, X-ray repair cross-complementing group 1.
HCC, hepatocellular carcinoma; HR, hazard ratio; CI, confidence interval.
Distribution of genotypes of XRCC1 rs25487 regarding clinical features
There were statistically significant differences between the wild genotype G/G and variant genotypes (A/A+G/A) in gender, HBV infection, cirrhosis, PVTT, serum AFP level, and TNM stage (all p < 0.05), whereas no statistically significant difference existed in age, tumor size, tumor number, or therapy method (all p > 0.05) (Table 4).
Genotypes of XRCC1 rs25487 and prognosis of HCC in patients receiving TACE stratified by different clinical features
In our stratified analyses, we found that variable genotypes (A/A+G/A) of XRCC1 rs25487 significantly reduced the risk of the death of HCC compared with the wild genotype G/G in patients with age >53 years (HR = 0.412; 95% CI = 0.223-0.764, p = 0.002), cirrhosis (HR = 0.356; 95% CI = 0.160-0.794, p = 0.005), tumor size ≥5 cm (HR = 0.467; 95% CI = 0.230-0.949, p = 0.019), serum AFP level ≥200 μg/L (HR = 0.528; 95% CI = 0.292-0.956, p = 0.016), and TNM stage III tumors (HR = 0.537; 95% CI = 0.299-0.967, p = 0.023) (Table 5). Additionally, statistically significant differences existed among the different genotypes of XRCC1 rs25487 and their respective prognostic values in HCC patients, as revealed by Kaplan-Meier survival curves and log-rank test (Fig. 2A-E).

Genotypes of XRCC1 rs25487 and the prognosis of HCC patients receiving TACE stratified by different clinical features; variable genotypes (A/A+G/A) of XRCC1 rs25487 significantly reduced the risk of the death of HCC compared with the wild genotype G/G in patients with age >53 years
Associations of clinical features with prognosis of HCC in patients receiving TACE
The prognostic factors of HCC in patients receiving TACE were analyzed using Cox's proportional hazards regression model. In univariate analysis, the tumor size ≥5 cm, positive PVTT, AFP ≥200 μg/L, and TNM stage III were associated with poor prognosis of HCC in patients receiving TACE (all p < 0.05). However, there were no significant differences among age, gender, HBV (positive or negative), cirrhosis, tumor number, Child-Pugh score (grade A or grades B/C), or TACE therapy alone (all p > 0.05). In multivariate analysis, there were significant relationships with prognosis as to the tumor size (HR = 0.505; 95% CI = 0.398-0.641, p < 0.001), PVTT (HR = 1.329; 95% CI = 1.160-1.524, p < 0.001), serum AFP level (HR = 1.632; 95% CI = 1.292-2.062, p < 0.001), and TNM stage (HR = 1.554; 95% CI = 1.166-2.070, p = 0.004) (Table 6).
Discussion
Our study strongly suggests that the outcomes in HCC patients receiving TACE are associated with tumor size, PVTT, serum AFP level, and TNM stage and these factors may be crucial prognostic indicators in HCC patients receiving TACE. Previous study indicated that the independent predictors for HCC patients are Child-Pugh score, tumor number, size, serum AFP level, and lung function after TACE therapy (Takayasu et al., 2012). Before surgery, evaluation of tumor size, tumor, location of the tumor, number of nodules, and degree of lesion and vascular invasion can lead to better treatment choices, leading to higher survival rate (Clavien et al., 2012). Evidence suggests that the outcome in HCC patients treated with TACE is related to tumor size and stage that reflects rapid tumor progression, including lymph node metastasis (Bruix et al., 2012; Utsunomiya et al., 2014).
Serum AFP level is useful for predicting the outcome of HCC in patients, and higher level of AFP is associated with poor prognosis (Toyoda et al., 2011), while lower AFP levels are associated with prolonged postoperative disease-free survival and reduces the recurrence risk in HCC patients (Chung et al., 2011). HCC patients with PVTT are at advanced stages, and patients with PVTT have extremely poor prognosis, suggesting that PVTT in HCC patients influences disease prognosis after TACE treatment (Tawada et al., 2014). Stratification of these risk factors may help identify optimal treatment regimens before surgery and increase survival rates of postoperative HCC patients (Yoon et al., 2012).
The main finding in our study is that the XRCC1 rs25487 polymorphism is related with better prognosis in HCC patients receiving TACE. On the other hand, the SNPs of two other DNA repair genes, XPD rs13181 and ERCC1 rs11615, do not show any correlation with the outcomes. Importantly, the variant genotypes (A/A+G/A) of XRCC1 rs25487 polymorphism significantly decreases death risk in the following patients groups: age >53 years group, positive PVTT, AFP ≥200 μg/L group, and TNM stage III group.
In addition, evidence suggested that HCC patients with XPD 751 (rs13181) Gln/Gln genotype showed a significantly lengthened survival time relative to those carrying Lys/Lys and Lys/Gln genotypes (Yue et al., 2013) and overexpressed ERCC1 levels were found to be correlated with therapy modalities and survival rates in HCC patients, but limited in the protein level (Ueda et al., 2011). Biological mechanisms of these diversities are complex, and studies with large sample size and well-designed study protocol are needed to validate these associations. The associations of XRCC1 and various cancer types such as breast cancer, head and neck cancer, and gastric cancer have been reported, and it is unclear whether the polymorphisms impair XRCC1 protein function by destroying its DNA repair capacity (Alanazi et al., 2013).
The polymorphism in XRCC1 rs25487 may function as a predictive marker, and patients carrying variant genotypes (A/A+G/A) exhibit increased median overall survival than the wild G/G genotype (www.doc88.com/p-8052917572149.html). XRCC1 protein is involved in DNA repair pathways through interacting with other DNA repair enzymes, and mutant XRCC1 may result in adverse effects such as genetic instability, cell death, mutagenesis, and carcinogenesis (Yue et al., 2013). HBV infections are a major risk factor in HCC development, and XRCC1 rs25487 polymorphism may modify clinical progression of hepatitis patients to HCC disease (Jung et al., 2012).
Consistent with our results, several studies have shown that XRCC1 rs25487 polymorphism is not a risk factor of HCC, and AA genotype may serve a protective role against HCC, implying that XRCC1 rs25487 is associated with better prognosis of HCC patients (Liu et al., 2011; Li et al., 2013a; Zhang et al., 2014). In our study, we speculate that reduced XRCC1 DNA repair capacity, due to XRCC1 rs25487 polymorphism, may further enhance the TACE efficacy by causing higher DNA damage and cell killing, and might thus contribute to better prognosis.
However, there are some limitations in this study that should be noted. First, our study was limited by analyzing a single XRCC1 SNP site and lacked haplotype analysis. Second, we did not assess the interactions between gene and environment because of insufficient data. Specific environmental conditions may be modifiers to gene polymorphisms. Third, the study did not consider the possibility of linkage disequilibrium between SNP-SNP interactions.
In conclusion, our study demonstrated that the outcomes in HCC patients receiving TACE were associated with tumor size, PVTT, serum AFP level, and TNM stage. Importantly, XRCC1 rs25487 was associated with better prognosis of HCC in patients receiving TACE. Variant genotypes (A/A+G/A) of XRCC1 rs25487 polymorphism could significantly decrease death risks of HCC patients than those carrying wild-type GG genotype.
Footnotes
Acknowledgments
The authors would like to thank the doctors and nurses from the Linyi People's Hospital affiliated to the Shandong University for helping with data and blood sample collection. The authors also thank the reviewers for their precious comments on this article.
Author Disclosure Statement
The authors have no financial or nonfinancial conflicts of interest to declare.