
Abstract
Background: Demonstrating the presence of myelodysplastic syndrome (MDS)-specific molecular abnormalities can aid in diagnosis and patient management. We explored the potential of using peripheral blood (PB) cell-free DNA (cf-DNA) and next-generation sequencing (NGS). Materials and Methods: We performed NGS on a panel of 14 target genes using total nucleic acid extracted from the plasma of 16 patients, all of whom had confirmed diagnoses for early MDS with blasts <5%. PB cellular DNA from the same patients was sequenced using conventional Sanger sequencing and NGS. Results: Deep sequencing of the cf-DNA identified one or more mutated gene(s), confirming the diagnosis of MDS in all cases. Five samples (31%) showed abnormalities in cf-DNA by NGS that were not detected by Sanger sequencing on cellular PB DNA. NGS of PB cell DNA showed the same findings as those of cf-DNA in four of five patients, but failed to show a mutation in the RUNX1 gene that was detected in one patient's cf-DNA. Mutant allele frequency was significantly higher in cf-DNA compared with cellular DNA (p = 0.008). Conclusion: These data suggest that cf-DNA when analyzed using NGS is a reliable approach for detecting molecular abnormalities in MDS and should be used to determine if bone marrow aspiration and biopsy are necessary.
Introduction
M
Molecular evaluation can be helpful in providing objective means for the demonstration of abnormal mutant clone and confirmation of the diagnosis of MDS (Itzykson et al., 2013; Bejar et al., 2011; Haferlach et al., 2014; Thol et al., 2012; Malcovati et al., 2014). Due to the cytopenia in PB, molecular studies of DNA extracted from cells in PB may not be able to identify abnormal clones with adequate sensitivity; hence, bone marrow is considered more reliable for detecting molecular abnormalities and confirming diagnosis of MDS. Furthermore, the detected abnormalities have clinical implication on prognosis and determining therapy. In addition, it is important to test using sensitive methods that are capable of detecting the presence of subclones that may dictate the overall prognosis (Bejar et al., 2013). However, since MDS is a disease of excessive apoptosis in bone marrow, DNA resulting from this apoptosis is abundant in circulation because hematopoietic cells are immersed in blood; these cells pour their contents during apoptosis or necrosis through blood in the form of apoptotic bodies, exosomes, microvessels, or DNA-protein complexes (Giles and Albitar, 2007).
In this study, we used high sensitivity sequencing with a next-generation sequencing (NGS) platform and compared cell-free DNA (cf-DNA) sequencing using NGS with PB cellular DNA sequencing by both Sanger sequencing and NGS. We compared with Sanger sequencing because at this time, it remains the standard procedure that is accepted, tested, and reimbursed by most insurance companies, while NGS is not reimbursed. We demonstrate that NGS using cf-DNA is reliable for the confirmation or ruling out the diagnosis of early MDS.
Materials and Methods
Patients and samples
PB samples were collected from 16 patients confirmed to have MDS by bone marrow evaluation and from four age-matched normal controls. All patients had blasts <5%. This included patients with refractory cytopenia with unilineage dysplasia, refractory cytopenia with multilineage dysplasia, and RARS. We extracted cf-DNA from plasma and cellular DNA from PB cells. The characteristics of the patients are listed in Table 1. All works were performed with institutional review board (IRB) approval.
DNA isolation
Total nucleic acid was isolated from plasma using NucliSENS EasyMAG automated platform (BioMerieux, Marcy-l'Étoile, France). DNA was then quantified using Qubit 2.0 Fluorometer (Thermo Fisher Scientific, Waltham, MA) and adjusted accordingly.
DNA from PB cells was isolated using a QIAamp DNA Blood Mini Kit (QIAGEN, Valencia, CA) in both manual and automated (QIAcube) extractions according to the manufacturer's instruction. Extracted DNA was then quantified using a NanoDrop 2000 (Thermo Fisher Scientific) instrument and adjusted to ∼50-100 ng/μL with H2O.
Gene sequencing
Using Sanger sequencing and NGS, we analyzed mutations in the following genes: ASXL1, ETV6, EZH2, IDH1, IDH2, NRAS, CBL, RUNX1, SF3B1, SRSF2, TET2, TP53, U2AF1, and ZRSR2. Sanger sequencing was performed using standard approach. The sequencing covered exon 12 of ASXL1 gene, the 8 exons of etv6, the 20 exons of EZH2 gene, exon 4 of IDH1 and IDH2, exon 2 of NRAS, exons 8 and 9 of CBL gene, exons 1-6 of RUNX1 gene, exons 13-16 of SF3B1 gene, exon 1 of SRSF2 gene, exons 3-11 of TET2, and exons 5-11 of TP53 gene. The primer pairs were designed to encompass >90% of reported mutations in these genes. Polymerase chain reaction products were purified and sequenced in both forward and reverse directions using an ABI PRISM 3730XL Genetic Analyzer (Applied Biosystems, Foster City, CA). Sequencing data were base-called using sequencing analysis software and assembled and analyzed with SeqScape software (Applied Biosystems).
NGS was performed using an Illumina MiSeq system (San Diego, CA); NGS, amplification, and indexing were performed as recommended by the manufacturer. Amplicons were confirmed for each sample by running an agarose gel. Samples were pooled and the experiment sheet was generated using Illumina Experiment Manager. An amplicon-based custom primer set was designed for our NGS using DesignStudio (www.illumina.com/designstudio). Library preparation and sequencing using MiSeq were performed according to the manufacturer's instruction. Human genome build 19 (hg19) was used for alignment. MiSeq Reporter was used for analysis, and Variant Studio was used for calling. For confirmation of variant calling, NextGENe software (SoftGenetics, State College, PA) was also used. Hot spots and abnormalities were confirmed using integrative genomic viewer. Average sequencing coverage across the entire coding regions was 4,000 in 94% of the sequenced amplicons. Uniformity was >90% for any run to be acceptable. Allele frequency for mutation was set at 5%. Positive, negative, and sensitivity control (5%) were used with each patch. This reliably allowed detection of mutations if present in at least 3% of mutant DNA.
Results
Confirming the presence of neoplastic abnormal MDS clone using cf-DNA
The 16 patients studied were confirmed to have MDS through the examination of bone marrow samples and complete cytogenetic and molecular evaluation. The characteristics of the patients are listed in Table 1. One of the 16 patients had chronic myelomonocytic leukemia and the rest had refractory anemia. Nine patients (56%) were males. All 16 patients had refractory anemia, two with ring sideroblasts. Cytogenetic data of bone marrow showed one patient with complex abnormalities, one with trisomy 8, and one with deletion in the long arm of chromosome 6. Upon deep sequencing of the plasma cf-DNA, all 16 patients showed at least one mutated gene, confirming the presence of an abnormal clone consistent with MDS (Table 2). No abnormality was detected in any of the four samples from normal control individuals. Eight patients (50%) showed mutation in one gene and the remaining eight patients (50%) showed mutations in two or more genes (Fig. 1).
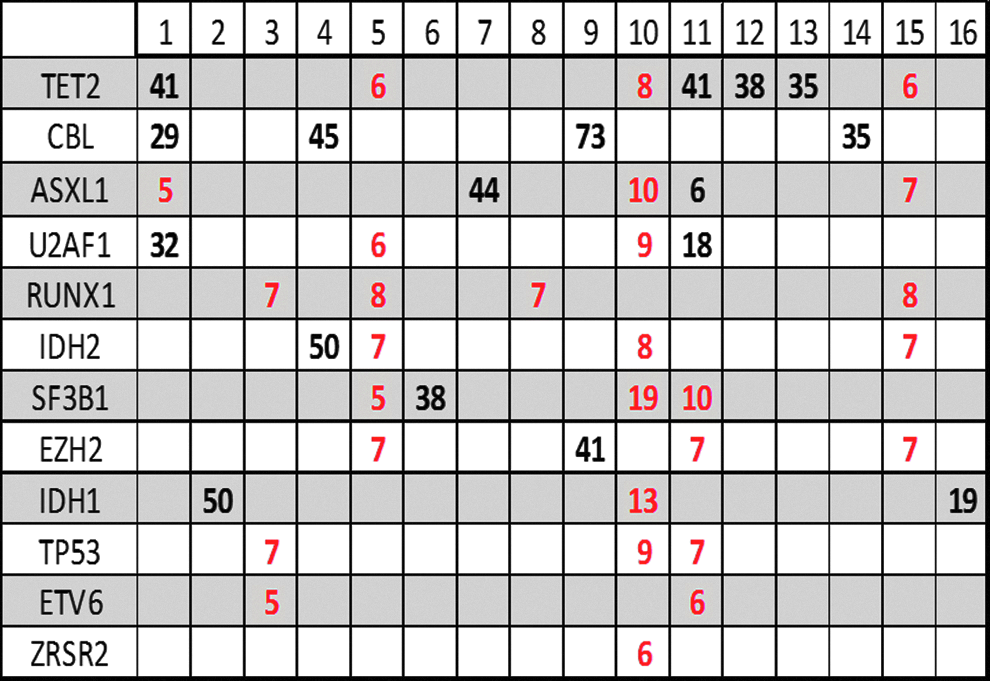
Mutation analysis in 16 patients. The percentage of the mutant allele is shown and indicates the presence of mutation. Black color indicates mutation detected by both Sanger sequencing of cellular DNA and NGS of cf-DNA. Red color indicates mutation detected in cf-DNA, but not in cellular DNA. cf-DNA, cell-free DNA; NGS, next-generation sequencing.
NGS, next-generation sequencing.
Our goal is not to directly compare cellular DNA with cf-DNA, but rather to demonstrate that cf-DNA using NGS can provide a new utility as a clinically useful test.
NGS of cf-DNA is more sensitive than Sanger sequencing of PB cellular DNA
Five of the 16 patients (31%) showed mutations detected by NGS of cf-DNA, while Sanger sequencing of PB cellular DNA showed no evidence of mutation. These patients would have been considered negative for MDS if Sanger sequencing of cellular DNA had been used. Of the remaining 11 patients, 3 (27%) showed additional mutations that were not detected by Sanger sequencing. Overall, 8 of the 16 patients (50%) showed mutations in plasma cf-DNA by NGS that were not detected in whole blood DNA by Sanger sequencing.
Except for one, all mutations detected in cf-DNA by NGS and not by Sanger sequencing in cellular DNA had allele frequency <18% (Fig. 1). In one sample, Sanger sequencing was able to identify indel mutation in ASXL, which was reported by NGS to be at 6%. This is unusual considering the overall sensitivity of Sanger and most likely was due to the shift in alignment. In general, the detection level of Sanger sequencing is between 15% and 20%, while the NGS sequencing is ∼5% (Chen et al., 2015).
NGS is more sensitive using cf-DNA compared with using cellular DNA
Since the detection level of NGS is significantly better compared with Sanger sequencing, we tested PB cellular DNA using NGS and compared the results with cf-DNA in five samples. Four of the five pairs (80%) showed identical results and one sample showed a mutation in RUNX1 at 7% in cf-DNA that was not detected in DNA from cellular DNA. Most likely, this reflects the relative enrichment of plasma by tumor-specific DNA. To confirm this, we compared the mutant allele frequency as detected in cf-DNA with that detected in PB cellular DNA. Based on paired samples from five patients, the level of the mutant allele in the cf-DNA is significantly higher than that in the cellular DNA from PB cells (p = 0.008; Fig. 2). This suggests higher sensitivity and enrichment of neoplastic DNA in plasma (Fig. 2).

Levels (percentage) of mutant allele in cell-free plasma DNA compared with levels of mutant allele in cells by NGS in samples analyzed by NGS.
Discussion
Demonstration of molecular abnormality in a patient suspected of having MDS is very important for the confirmation of diagnosis, prediction of prognosis, and determining therapeutic approach. This is particularly important in regard to patients with early MDS (blasts in bone marrow <5%). In this group of patients, frequently the diagnosis remains speculative even after performing bone marrow aspiration and biopsy. Morphologic changes can be subtle and cytogenetic abnormalities may not be present. With recent advances in molecular characterization of MDS, the diagnosis of MDS is becoming more reliant on molecular testing in detecting the presence of an abnormal clone. Furthermore, the type of the detected molecular abnormality may provide significant information for predicting prognosis and determining clinical course and therapy.
In contrast, PB cytopenia, which is the major presenting symptom for suspecting MDS diagnosis, can be seen in several reactive processes and represents a diagnostic dilemma in determining whether bone marrow biopsy is needed or not.
Performing molecular studies using PB cells is a possible approach to confirm the presence of MDS. However, due to the cytopenia in PB, demonstrating molecular abnormalities in PB cells requires high sensitivity testing and NGS provides significantly better sensitivity than Sanger sequencing. Negative results do not always rule out the presence of MDS.
In using NGS on MDS patients with blast counts less than 5%, we were able to detect abnormalities in all cases. NGS when performed using cf-DNA is clearly superior to Sanger sequencing of PB cellular DNA. Although NGS was performed on cellular DNA in only a subset of patients, it shows that plasma cf-DNA is superior to cellular DNA in detecting molecular abnormalities and confirming MDS diagnosis. We also found that the cf-DNA is less diluted by normal cell DNA and more enriched by MDS-specific DNA. This was exhibited as shown by the significantly higher mutant allele detected in cf-DNA compared with cellular DNA using NGS (p = 0.008; Fig. 2).
Although we have not tested patients with more advanced MDS, previous studies (Ma et al., 2009; Yeh et al., 2009; Ma et al., 2008; Ma et al., 2007; Rogers et al., 2004; Ahmed et al., 2003; Jilani et al., 2003) show that these patients should have more circulating cf-DNA, thus the detection of molecular abnormalities to confirm the diagnosis of MDS should be easier in these cases.
This study was not intended to directly compare cellular DNA with cf-DNA, but rather to demonstrate that cf-DNA and NGS can provide a new clinical tool in the diagnosis of MDS.
In summary, the study suggests that cf-DNA is more reliable than PB cellular DNA in detecting molecular abnormalities in patients with MDS even when the blast count is less than 5%. Furthermore, NGS is more accurate than Sanger sequencing and should be considered as the method of choice for analyzing cell-free DNA confirming the diagnosis of MDS.
Footnotes
Acknowledgment
All funding for this work was provided by the NeoGenomics Laboratories.
Author Contributions
F.A. performed testing, collected data, and wrote the article; W.M. designed work, performed testing, and analyzed data; K.D. performed work, I.D.D. performed work and analyzed data; S.A. developed concept and contributed cases, M.T. developed concept and contributed cases; S.B. developed concept and contributed cases; and M.A. developed concept, analyzed data, and wrote the article.
Author Disclosure Statement
The authors listed work for NeoGenomics Laboratories, which offers diagnostic testing.