
Abstract
Objective:
Previous studies have investigated the association between tumor necrosis factor-alpha (TNF-α) -308G/A polymorphism and risk of immune thrombocytopenia (ITP), but the reported results have been inconsistent. Thus, a systematic meta-analysis was performed to resolve this discrepancy.
Methods:
Electronic databases and the cited references of the obtained published articles were manually searched. Quality assessment of each study was conducted using the Newcastle-Ottawa Scale (NOS). All case-control studies were used to assess the strength of the association. Statistical analysis was performed using Stata version 12.0.
Results:
Eight high-quality studies, including 947 patients and 1911 controls, were selected for the final meta-analysis. There was no significant association between TNF-α -308G/A polymorphism and ITP in overall and Asian populations. However, a significant positive association was observed between them in the dominant genetic model (AA+AG versus GG) in the Caucasian population (OR = 1.35, 95% confidence interval [CI]: 1.07-1.71, PH = 0.173).
Conclusions:
Our finding suggested that TNF-α -308G/A might be involved in development of ITP in the Caucasian population, but not in the Asian population. Among Caucasians the A allele (AA+AG) was associated with ITP. However, larger-scale studies are required to confirm our findings.
Introduction
I
TNF-α is a potential proinflammatory cytokine that plays a prominent role in the inflammatory and immune response, and it is involved in regulation of cell proliferation and differentiation (Qidwai and Khan, 2011). SNPs are common in the promoter region of TNF-α. Several polymorphisms such as -238A/G (rs361525), -308G/A (rs1800629), -857C/T (rs1799724), -863C/A (rs1800630), and -1031T/C (rs1799964) in the region were reported to influence the expression of TNF-α (Hellmig et al., 2005; Somi et al., 2006). Moreover, overexpression of TNF-α was observed in many inflammatory diseases, such as type 2 diabetes mellitus, allergic disease, and autoimmune disease (Schulz et al., 2014; Sefri et al., 2014; Li et al., 2015). Previous studies reported that TNF-α -308G/A could affect its transcription (Messer et al., 1991; Bidwell et al., 1999), and the locus was speculated to increase the risk and exacerbate the outcome of ITP.
Despite numerous previous studies that reported the relationship between TNF-α -308G/A and ITP in various populations and regions (Foster et al., 2001; Satoh et al., 2004; Rocha et al., 2010; Okulu et al., 2011; Pehlivan et al., 2011; Sarpatwari et al., 2011; El Sissy et al., 2014; Wang et al., 2014; Pavkovic et al., 2015; Yadav et al., 2016), the results were not consistent and conflicting. Some studies demonstrated no significant association between them (Satoh et al., 2004; Okulu et al., 2011; Wang et al., 2014; Yadav et al., 2016). However, others demonstrated that A allele of the locus was associated with an elevated cytokine production, contributing to increased risk of ITP (Foster et al., 2001; Pehlivan et al., 2011; Sarpatwari et al., 2011). Therefore, to better clarify the association, this meta-analysis aimed to synthesize data from different studies to elucidate whether TNF-α -308G/A polymorphism was associated with increased susceptibility to ITP.
Materials and Methods
Literature search
All case-control studies concerning association between TNF-α -308G/A and ITP were identified by searching relevant electronic databases of PubMed, Web of Science, Ovid, Scopus, Chinese Biomedical Literature Database, Wan Fang DATA, and China National Knowledge Infrastructure until March 2016. The following keywords were included: tumor necrosis factor OR TNF AND polymorphism OR variant OR variation OR mutation OR genotype AND ([immune thrombocytopenia] OR [idiopathic thrombocytopenic purpura] OR [immune thrombocytopenic purpura] OR [idiopathic thrombocytopenia] OR ITP). In addition, all relevant references mentioned in the full-text publications were manually searched to retrieve potential studies.
Inclusion and exclusion criteria
The inclusion criteria were included as follows: (1) ITP patients were confirmed according to the diagnostic criteria used by the International Working Group (Rodeghiero et al., 2009; Neunert et al., 2011); (2) the case-control studies evaluated association between TNF-α -308G/A and ITP; (3) sufficient information in cases and controls could be acquired to estimate odds ratio (OR) with 95% confidence interval (CI); and (4) the studies contained no restricted language. Meanwhile, duplicate study and a study without detail genotype data or the data not in agreement with Hardy-Weinberg equilibrium (HWE) were excluded in our study.
Data extraction
The data of the eligible studies were independently extracted by two investigators (Jing Zhang and Yan-Mei Xu). Any discrepancies were resolved after discussion, and a consensus was ultimately reached. The following information was extracted: name of the first author, year of publication, country, ethnicity, disease type, mean age, sample size, genotype distribution in cases and controls, and p-value of HWE in controls.
Quality assessment
The quality of each study was assessed independently by two investigators (Yan Wang and Fan Sun) in accordance with the Newcastle-Ottawa Scale (NOS), which awarded studies with a star scoring scale (Stang, 2010). A study can be given a maximum of one star for each numbered item within the Selection and Outcome. A maximum of two stars can be assigned for Comparability. High-quality studies are indentified with a NOS score of five or more, whereas those with less than a score of five were considered to be low-quality studies.
Statistical analyses
The association between TNF-α -308 G/A and ITP was assessed by pooled OR with 95% CI. Meta-analyses were performed for all genetic models. HWE in controls was evaluated by the chi-square test (Wang, 2012). Heterogeneity among studies was examined with the inconsistency index (I2) statistic (Higgins et al., 2003). If the value of I2 was more than 50% and a p-value of heterogeneity test (PH) was less than 0.10, the random effect model would be used to calculate the pooled OR. Otherwise, a fixed effects model was used to assess the heterogeneity (Zintzaras and Ioannidis, 2005). Sensitivity analysis was conducted to assess the effect of each study by excluding one study at a time. Publication bias was detected by Begg's funnel plot and Egger's regression test (Egger et al., 1997), and p < 0.05 was considered as a significant publication bias. All statistical analyses were performed with Stata 12.0 software (StataCorp, College Station, TX).
Results
Study characteristics
The search strategy initially identified 494 potentially relevant studies based on the inclusion criteria, and 55 duplicate publications were excluded. By screening the title and abstract, we deemed 413 articles to be incongruous with the aim of our study. Thus, 26 records remained, of which 15 were removed for not being related to the TNF-α -308G/A polymorphism and just one was removed for lack of providing the accurate genotype data. However, genotype distributions of the locus in two studies were not in accordance with HWE test (Foster et al., 2001; Satoh et al., 2004). At last, a total of eight case-control studies, including 947 cases and 1911 healthy controls, were included in the final meta-analysis (Rocha et al., 2010; Okulu et al., 2011; Pehlivan et al., 2011; Sarpatwari et al., 2011; El Sissy et al., 2014; Wang et al., 2014; Pavkovic et al., 2015; Yadav et al., 2016) (Fig. 1). Five eligible studies are described in Table 1, and the detail quality assessment of the case-control studies is listed in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/gtmb).
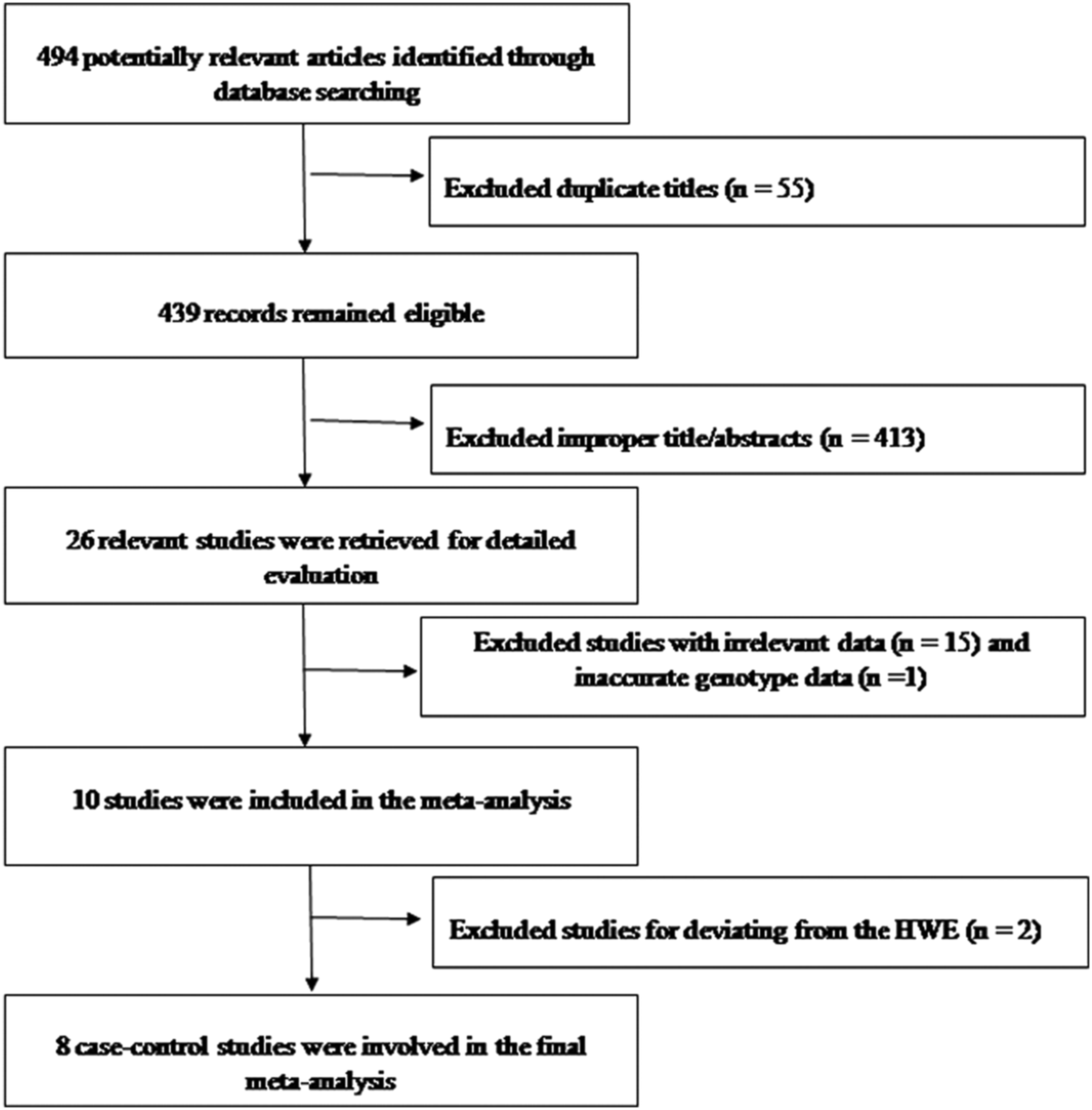
Flow diagram of study selection process.
HWE, Hardy-Weinberg equilibrium; NA, not available; NOS, Newcastle-Ottawa Scale.
Overall analysis
Overall, eight eligible studies were pooled in this study; no evidence of a significant association was observed between TNF-α -308G/A and ITP risk in any genetic model (dominant model: A/A+A/G versus G/G, OR = 1.11, 95% CI = 0.80-1.53, I2 = 52.4%, PH = 0.04; allele model: G versus A: OR = 0.87, 95% CI = 0.60-1.25, I2 = 70.3%, PH = 0.001; A/G versus G/G: OR = 0.87, 95% CI = 0.71-1.07, I2 = 17.2%, PH = 0.294) (Supplementary Figs. S1 and S2; Fig. 2). As some studies in our meta-analysis reported that the distribution of AA was absent among patients and controls (Okulu et al., 2011; Pehlivan et al., 2011; Wang et al., 2014; Yadav et al., 2016), data of the two genetic models (GG versus AA and AG+GG versus AA) were not available.
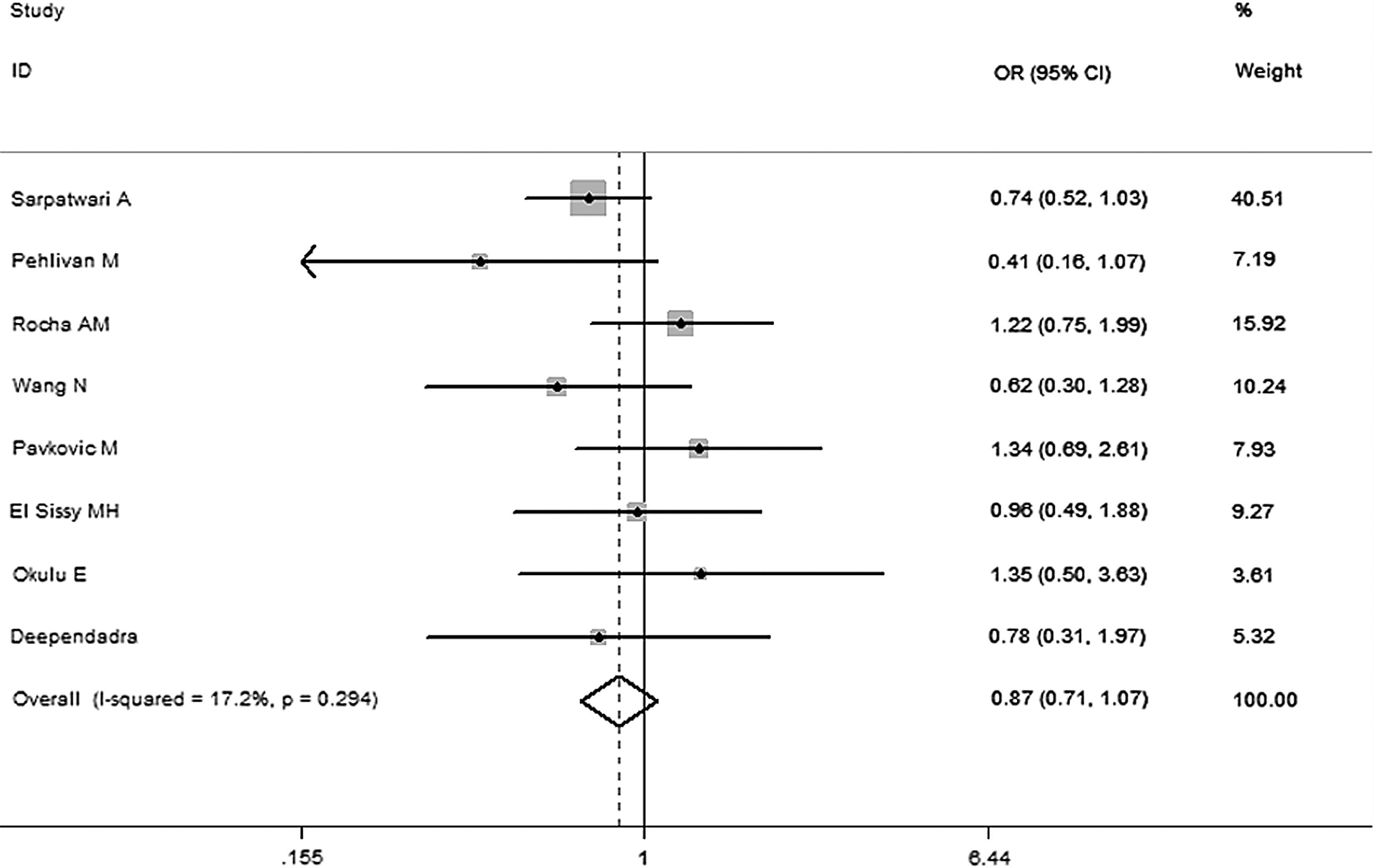
Forest plots for TNF-α -308G/A polymorphism and ITP risk in genetic model (AG vs. GG). ITP, immune thrombocytopenia; TNF-α, tumor necrosis factor-alpha.
Subgroup analysis
Three subgroups were stratified on the basis of ethnicity, mean age, and the type of ITP. There were no statistically significant differences in age and ITP type between cases and controls. However, ethnicity analysis revealed a significant association between them in the dominant model (AA+AG versus GG in Caucasians) (OR = 1.35, 95% CI 1.07-1.71, I2 = 33.40%, PH = 0.173), but not in Asians (OR = 0.81, 95% CI: 0.46-1.43, I2 = 31.60%, PH = 0.227) (Fig. 3).
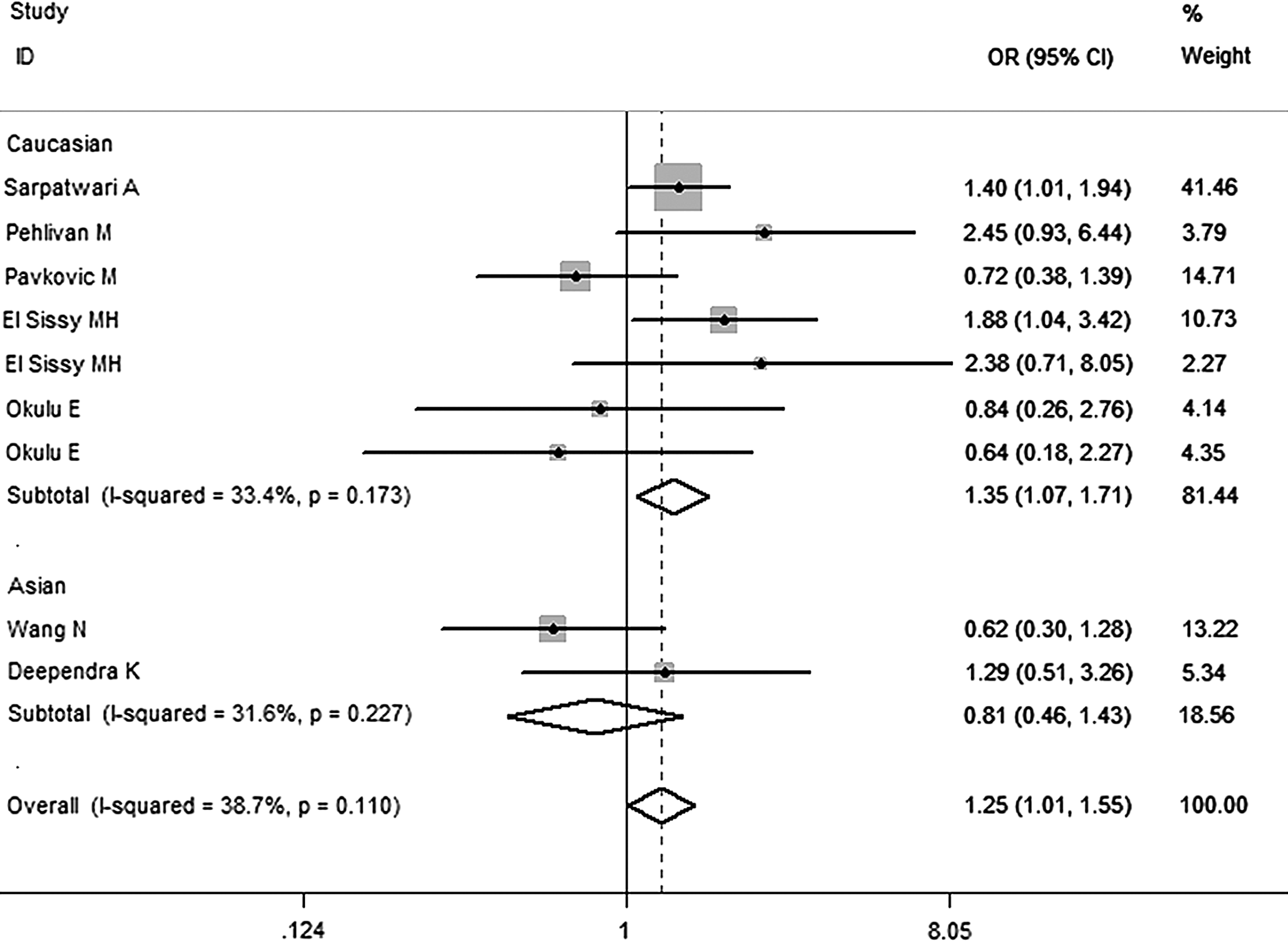
Meta-analysis for the association between ITP risk and the TNF-α -308A/G polymorphism (dominant model: AA+AG vs. GG).
Sensitivity analysis
Sensitivity analysis was conducted to assess the effect of each study by omitting a single study at a time. After excluding the study deviation from HWE (Foster et al., 2001; Satoh et al., 2004), the results of the meta-analysis were stable.
Publication bias
Begg's funnel plot and Egger's regression test were selected to evaluate publication bias in our study. The funnel plot showed almost symmetrical (Fig. 4), and p-value of Egger's test (p = 0.92) was larger than 0.05. These results indicated that no potential publication bias was observed in our study.
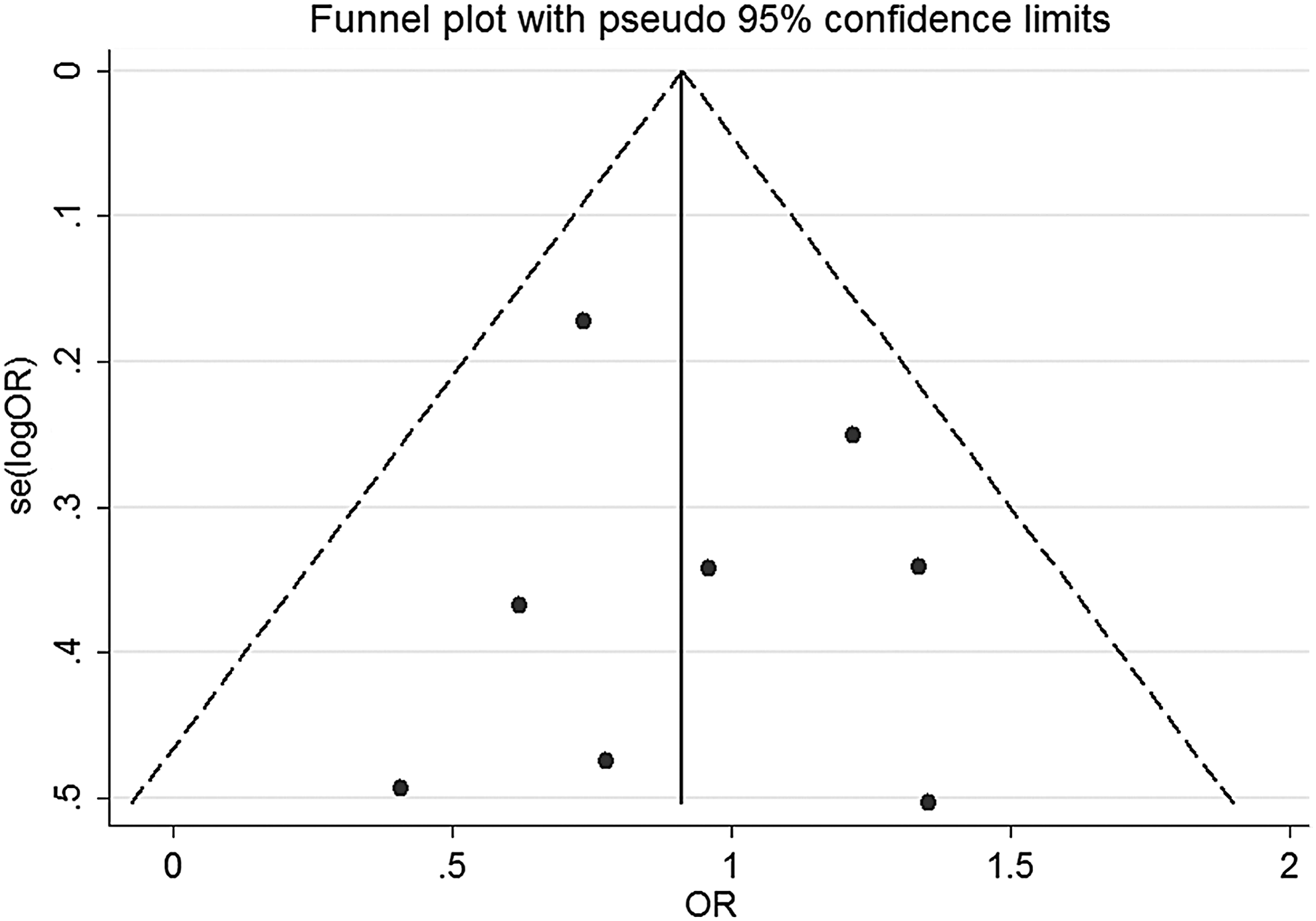
Funnel plots for TNF-α -308G/A polymorphism and ITP risk (AG vs. GG).
Discussion
The present meta-analysis of eight high-quality case-control studies, including 947 patients and 1911 controls, revealed that TNF-α -308G/A under the dominant model (AA+AG versus GG) might significantly increase ITP risk in Caucasians, however, no statistical significant association was observed in overall and Asian populations, revealing that allele A carrier (AA+AG) of rs1800629 might increase predisposition to ITP in Caucasians.
The following reasons may explain our findings. Owing to differences in ethnic genetic backgrounds in Asians and Caucasians, frequency of the A allele is conspicuously higher in the Caucasian population than in the Asian population (Table 1). Moreover, only two studies, including a total of 295 patients and 306 controls, were conducted in the Asian population, and the relative small sample sizes of cases and controls might limit the power to reach a more reliable result. Besides, TNF-α -308G/A polymorphism was reported to affect gene transcription by increasing TNF-α production and regulating cell proliferation and differentiation, leading to potentially exacerbate the outcomes of ITP (Qidwai and Khan, 2011).
In addition, we should emphasize the importance of the heterogeneity and publication bias, which could affect the results of meta-analysis (Sterne and Egger, 2001). Supplementary Figure S3 shows that the study with low quality implemented by Foster et al. (2001) could cause publication bias. Table 1 presents that the data detected by Satoh et al. (2004) and Foster et al. (2001) were not in agreement with HWE. Once the two studies were excluded, the funnel plot showed almost symmetrical, suggesting deviation of allelic distribution from HWE might influence publication bias. Moreover, there was statistically significant heterogeneity between them in the dominant genetic model (Table 2). After the ethnicity analysis, the heterogeneity could effectively decrease, indicating that the ethnicity analysis, to some extent, may be used to explore the source of heterogeneity. Interestingly, analysis of frequency of A allele revealed that the prevalence of A allele was considerably lower in Asians than in Caucasians among cases and healthy controls (Table 1), suggesting that the rarity of the A allele hardly exhibits polymorphism in Asians. Therefore, the distributional difference of the A allele may contribute to the probability of false results.
Data for p < 0.05.
F, fixed effects models; R, random effects model.
Our meta-analysis is the first assessment of the relationship between TNF-α -308G/A and risk of ITP. However, some limitations of this meta-analysis should be addressed. First of all, the number of studies and sample size included in this meta-analysis are relatively small. In addition, some eligible negative studies may not be published. Consequently, some potential publication bias may occur inevitably in our results. Finally, owing to insufficient data, we could not carry out the analysis of gene-environment interaction in this meta-analysis.
In conclusion, TNF-α -308G/A polymorphism may play a role in development of ITP, and allele A carrier (AA+AG) of the locus was a possible susceptible factor for Caucasians. Considering the limitations of the current study, a larger sample size in Asians and a potential target for therapeutic intervention in ITP are warranted to further validate the results.
Footnotes
Acknowledgment
This report was supported by the National Natural Science Foundation of China (No. 81271912 and No. 81360083).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.