
Abstract
Background and Aims:
Interleukin-10 (IL-10) plays a vital part in the pathophysiology of vascular inflammation. Several studies have investigated the potential association between the IL-10-1082A/G polymorphism and the risk of ischemic stroke where the inflammatory process is involved, but the conclusions have been inconsistent.
Methods:
Three hundred eighty-six ischemic stroke patients and 386 healthy controls were recruited in the study. Genotyping was conducted by using the polymerase chain reaction-ligation detection reaction method. A meta-analysis was then performed by pooling our data with previous published studies.
Results:
In our case-control study, a lack of association was revealed between IL-10-1082A/G and ischemic stroke (p > 0.05). When combined with previous studies, however, a significant relationship between IL-10-1082A/G and ischemic stroke risk was found (G vs. A: OR = 0.73, 95% CI = 0.60-0.88, p < 0.01; GG vs. AA: OR = 0.61, 95% CI = 0.49-0.76, p < 0.01; GG+AG vs. AA: OR = 0.70, 95% CI = 0.54-0.91, p < 0.01; GG vs. AG+AA: OR = 0.68, 95% CI = 0.52-0.89, p < 0.01), as well as in subgroup analyses. Sensitivity analysis and publication bias assessment supported the reliability of the results from the meta-analysis.
Conclusions:
Evidence from a case-control study to an updated meta-analysis suggests that the IL-10-1082A/G polymorphism is associated with ischemic stroke susceptibility.
Introduction
S
Interleukin-10 (IL-10) is an immunomodulatory cytokine that is mainly secreted by activated monocytes, lymphocytes, and macrophages (de Vries, 1995). Several experimental studies have reported that IL-10 can inhibit the production of pro-inflammatory mediators as well as the activation of macrophages, which may protect endothelial cells and slow the progression of vascular inflammation and thrombosis (Caligiuri et al., 2003; Yin et al., 2013; Han and Boisvert, 2015). Moreover, a clinical study revealed that patients with vulnerable atherosclerotic plaques had significantly reduced serum IL-10 levels (George et al., 2012). Human IL-10 gene is located on chromosome 1q31-q32 and consists of 5 exons and 4 introns that span over 4800 bp (Niu et al., 2015). A polymorphic G allele at the −1082 position of the IL-10 gene promoter region has been shown to affect the mRNA expression of IL-10 (Kingo et al., 2005). The serum IL-10 levels from individuals with the GG or GA genotypes were statistically higher than those from individuals with the AA genotype (Lesiak et al., 2014).
The potential association of IL-10-1082A/G with IS risk has been gradually investigated by several studies on different ethnic populations. Unfortunately, the conclusions have not come to an agreement. Some studies found an association between IL-10-1082A/G and IS susceptibility (Munshi et al., 2010; He et al., 2015). Nevertheless, these results have not been verified in other studies (Jin et al., 2011; Marousi et al., 2011). To address this issue, we first evaluated the association of IL-10-1082A/G with IS risk in a new case-control study, and we then performed a comprehensive meta-analysis to derive a more reliable and precise result.
Materials and Methods
Study participants
This study recruited 386 IS patients and 386 controls from the Chinese Han population in Liaoning Province. Eligible cases were those patients who were diagnosed as IS for the first time according to neurological examination and radiological imaging. The patients were recruited consecutively in the First Hospital of China Medical University. The controls without IS and other neurological diseases were enrolled from the physical examination department of the Shenyang Red Cross Hospital, and they were matched with age and sex. This study was approved by both hospitals' ethics committees, and in agreement with the Helsinki Declaration. Also, written informed consent was obtained from all participants.
Genotyping
Genomic DNA was extracted by using standard procedures from peripheral blood leukocytes. Genotyping was conducted by the polymerase chain reaction-ligation detection reaction (PCR-LDR) method. The primer sequences for PCR: Forward: CAGGATTCCATGGAGGCTGGA; Reverse: CCCTGTGGAAGGGGAAGGTG. PCR amplification was conducted in a total volume of 10 μL, which contained 0.3 mM dNTP, 3.0 mM Mg2+, 1× GC buffer I, 1 U HotStarTaq polymerase, 1 μL genomic DNA, and 1 μL of each of the primers. The PCRs were cycled as follows: 95°C for 2 min, followed by 11 cycles of 94°C for 20 s, 65°C (decreased 0.5°C per cycle) for 40 s, 72°C for 1.5 min, and then 24 cycles of 94°C for 20 s, 59°C for 30 s, and 72°C for 1.5 min, and a final extension at 72°C for 2 min. The probe sequences for LDR: RC: TCTCTCGGGTCAATTCGTCCTTCAAGACAACACTACTAAGGCT TCTTTGGTAG; RP: GGGGAAGTAGGGATAGGTAAGAGGATTTTTTTTTTTT TTTTTTTTT; RT: TGTTCGTGGGCCGGATTAGTCAAGACAACACTACTAAG GCTTCTTTGGCAA. The LDRs were conducted in a final volume of 10 μL, containing 2 μL PCR product, 0.4 μL 3′ ligase primer mixture, 0.4 μL 5′ ligase primer mixture, 0.25 μL Taq DNA ligase, 1 μL 10× ligase reaction buffer, and 6 μL double-distilled H2O. The LDR cycling program was set as follows: 38 cycles of 94°C for 60 s and 56°C for 4 min, and it was kept at 4°C. After the reaction, the LDR product was sequenced by using the ABI3730XL sequencer.
Statistical analysis
Hardy-Weinberg equilibrium (HWE) analysis was assessed by the χ2 test for genotypes in the case-control group. Differences of allele and genotype distribution between cases and controls were analyzed by using the χ2 test. The association of IL-10-1082A/G polymorphism with IS was estimated by odds ratios (ORs) and 95% confidence intervals (CIs) from logistic regression analysis after adjusting for traditional risk factors. A value of p < 0.05 was considered statistically significant. All statistical analyses were performed with SPSS17.0 software.
Meta-analysis
To further investigate the association of IL-10-1082A/G with IS risk, a meta-analysis combining published literature and our current study was performed. We searched literature from Pubmed, Embase, Chinese WanFang database, and China National Knowledge Infrastructure (CNKI) till August 31, 2016. The following terms were used in the search strategies: interleukin 10/interleukin-10/IL 10/IL-10 and cerebral infarction/stroke/brain infarction/cerebral ischemia and genotype/polymorphism/variant/allele.
The included studies should meet the following criteria: (1) case-control design; (2) genotype frequencies in the control group consistent with HWE; and (3) availability of allele or genotype frequency for calculating ORs and 95% CIs. To assess the quality of eligible studies, a series of predetermined criteria, which were derived by Thakkinstian et al. (2005), were structured, with scores from 0 to 15. The studies with scores of ≥10 or <10 were considered high- and low-quality studies, respectively (Qin et al., 2013; Lu et al., 2014). The following information was collected: first author, year of publication, ethnicity, genotyping method, quality score of studies, characteristics, and genotype distribution of cases and controls.
Heterogeneity among studies was assessed with I2 statistic, and I2 greater than 50% indicates significant heterogeneity. If there was heterogeneity in the studies, a pooled OR was calculated by the random effect model; otherwise, a fixed effect model was adopted. Subgroup analyses were conducted involving ethnicity, the genotyping method, source of controls, sample size, case-control matched status, and study quality. Sensitivity analysis was conducted to examine the effect of individual studies on pooled results and the stability of results. Publication bias was assessed by the funnel plot and Egger's regression test. A value of p < 0.05 was considered statistically significant. Data were analyzed with Stata 12.0.
Results
Our current case-control study
Three hundred eighty-six IS patients and 386 controls were included in our case-control study. The characteristics of the patients and controls are shown in Table 1. No significant difference existed in age (p = 0.83), gender (p = 0.88), or body mass index (p = 0.20) between IS patients and controls. However, the prevalence of traditional risk factors (hypertension, diabetes, hyperlipidemia, and smoking) was significantly higher in IS patients (p < 0.01).
BMI, body mass index.
The allele and genotype frequencies of IL-10-1082A/G in patients and controls are listed in Table 2. The genotype distribution in both patients and control subjects was satisfied with HWE (p = 0.56 for patients, p = 0.50 for controls). As shown in Table 2, no significant difference existed in allele and genotype distribution between patients and controls. Furthermore, logistic regression analysis was performed to assess the relationship of IL-10-1082A/G with IS risk. It showed no association under any genetic model after adjusting for the confounding factors (AG vs. AA: OR = 0.96, 95% CI = 0.66-1.41, p = 0.84; GG vs. AA: OR = 1.73, 95% CI = 0.40-7.56, p = 0.47; GG+AG vs. AA: OR = 1.00, 95% CI = 0.69-1.45, p = 0.98; GG vs. AG+AA: OR = 1.75, 95% CI = 0.40-7.61, p = 0.46; Table 2).
CI, confidence interval; OR, odds ratio.
Meta-analysis
The primary literature search generated 137 potential studies, among which 11 studies met the inclusion criteria (Zhang et al., 2007; Munshi et al., 2010; Jin et al., 2011; Marousi et al., 2011; Tuttolomondo et al., 2012; He et al., 2015; Jiang et al., 2015; Ozkan et al., 2015; Kumar et al., 2016a; Li et al., 2016). The study selection process is detailed in Figure 1. The characteristics and genotype distribution of studies are listed in Table 3.
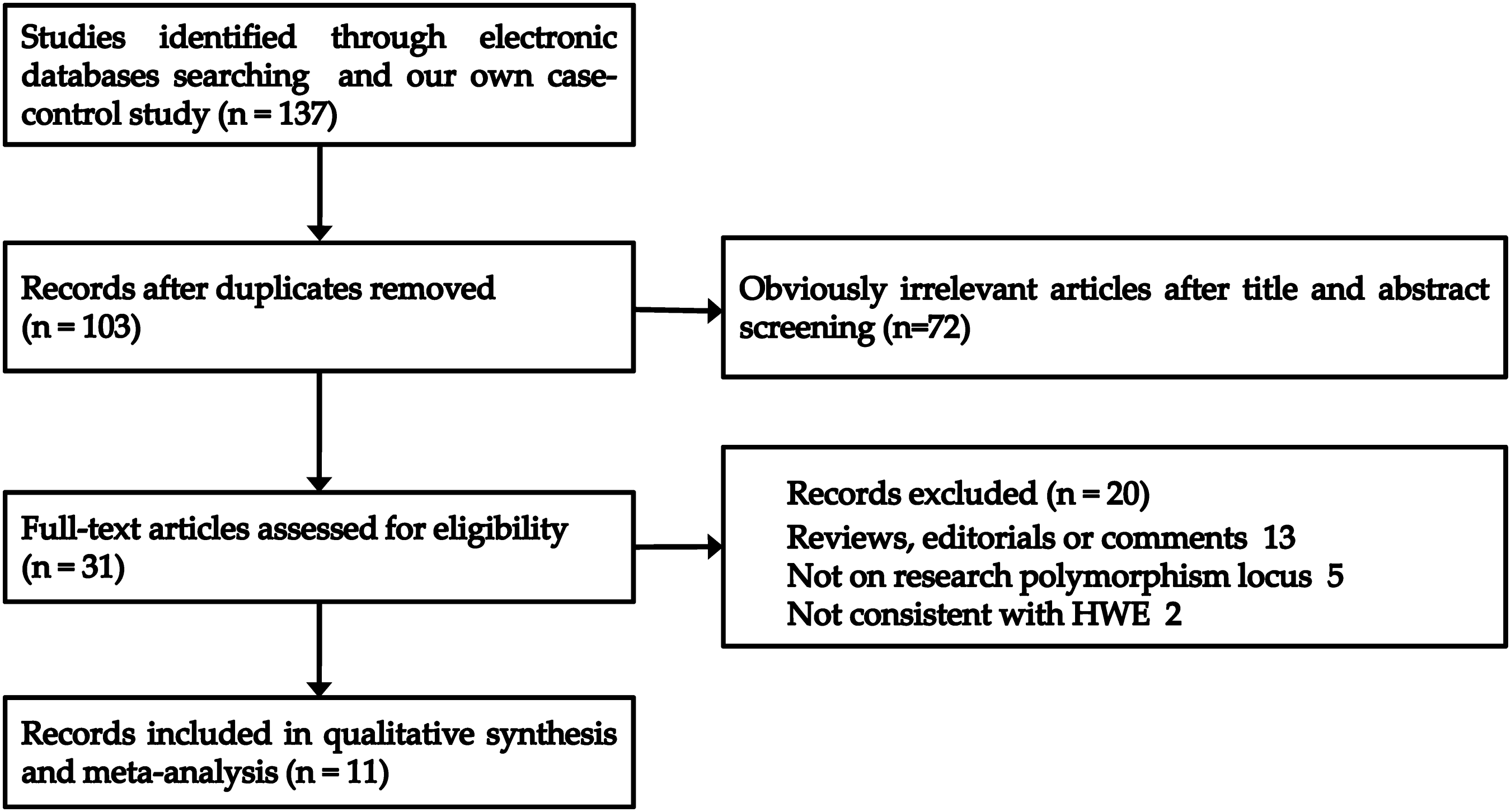
Flow diagram of the study selection process.
ARMS, amplification refractory mutation system; HWE, Hardy-Weinberg equilibrium; PCR-LDR, polymerase chain reaction-ligation detection reaction; RFLP, restriction fragment length polymorphism.
The relationship of IL-10-1082A/G with IS risk was analyzed in 11 original studies, including 2568 patients and 2280 controls. As shown in Figure 2-5, the pooled analysis indicated the significant association between IL-10-1082A/G and IS under four genetic models (G vs. A: OR = 0.73, 95% CI = 0.60-0.88, p < 0.01; GG vs. AA: OR = 0.61, 95% CI = 0.49-0.76, p < 0.01; GG+AG vs. AA: OR = 0.70, 95% CI = 0.54-0.91, p < 0.01; GG vs. AG+AA: OR = 0.68, 95% CI = 0.52-0.89, p < 0.01; Table 4). In the subgroup analysis by ethnicity, similar results were revealed in the Asian population under all five genetic models. Significant associations with IS risk were also found under five genetic models in the population-based control group and the PCR-RFLP group, as well as under three genetic models in the age- and sex-matched group. Subsequent analyses accounted for sample size and quality of included studies; some significantly decreased risks were also observed in large sample-size subgroups and high-quality studies (Table 4).
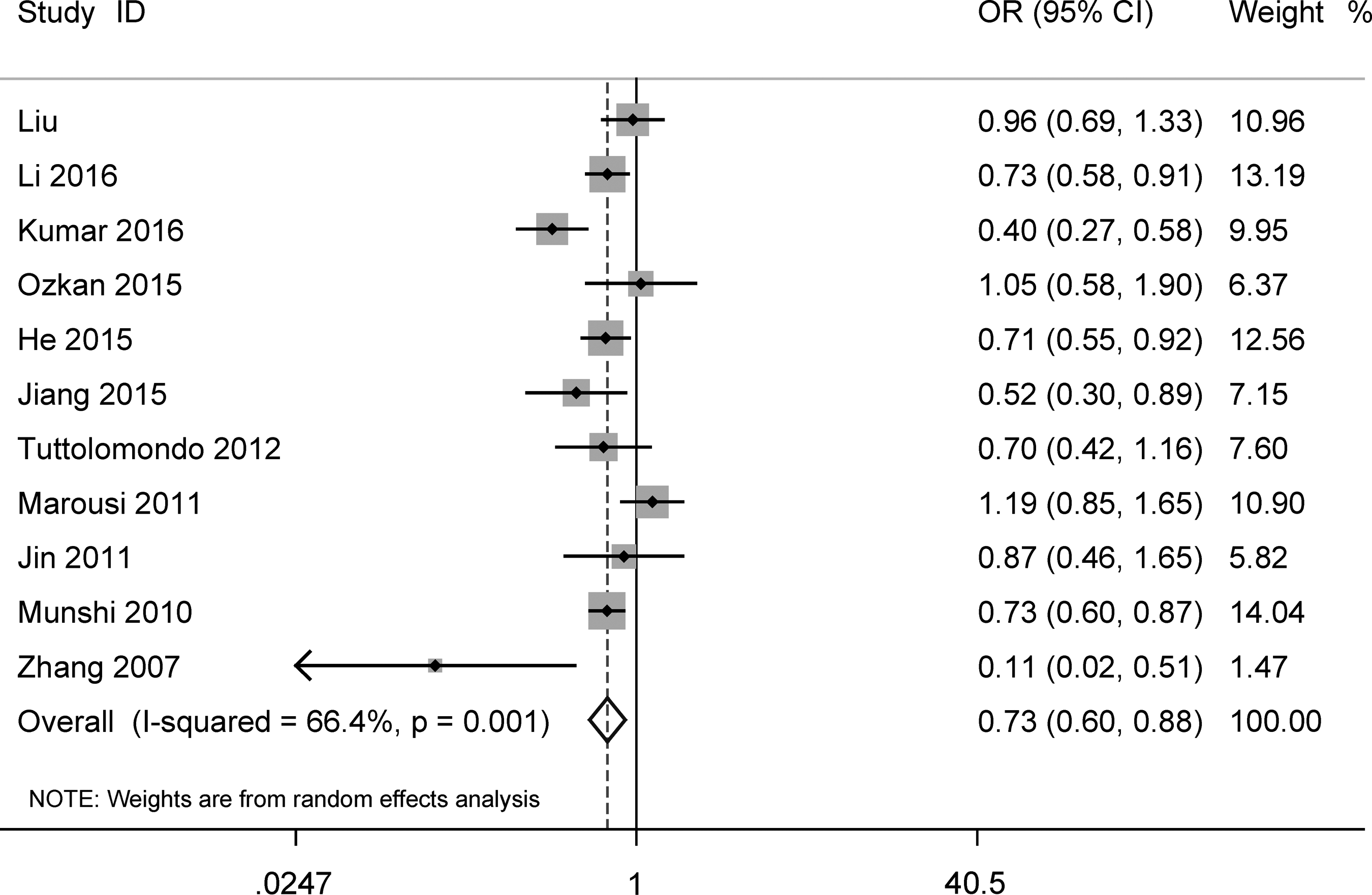
Forest plot for IL-10-1082A/G polymorphism and ischemic stroke risk under allele model (G vs. A).
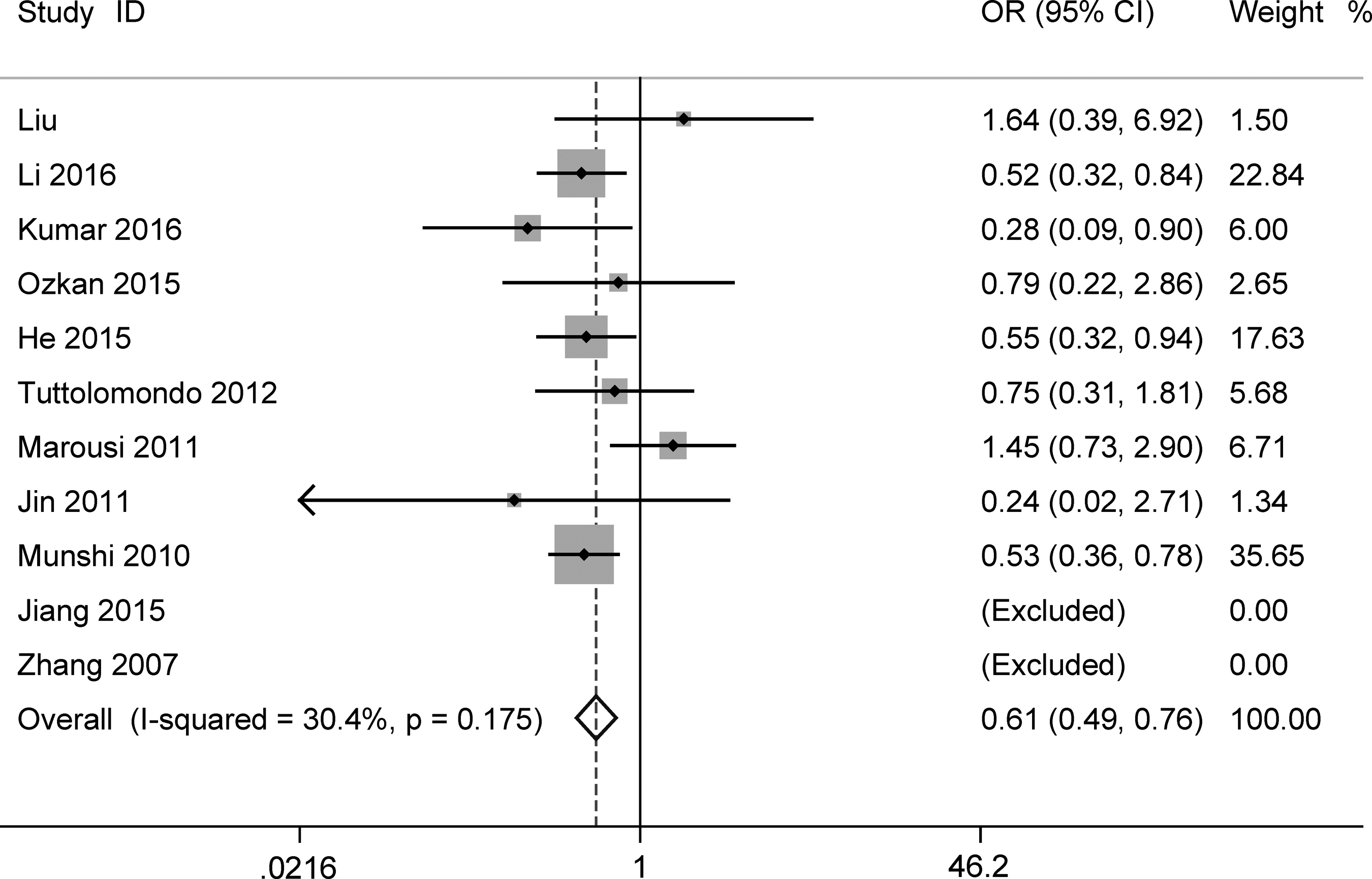
Forest plot for IL-10-1082A/G polymorphism and ischemic stroke risk under homozygote model (GG vs. AA).
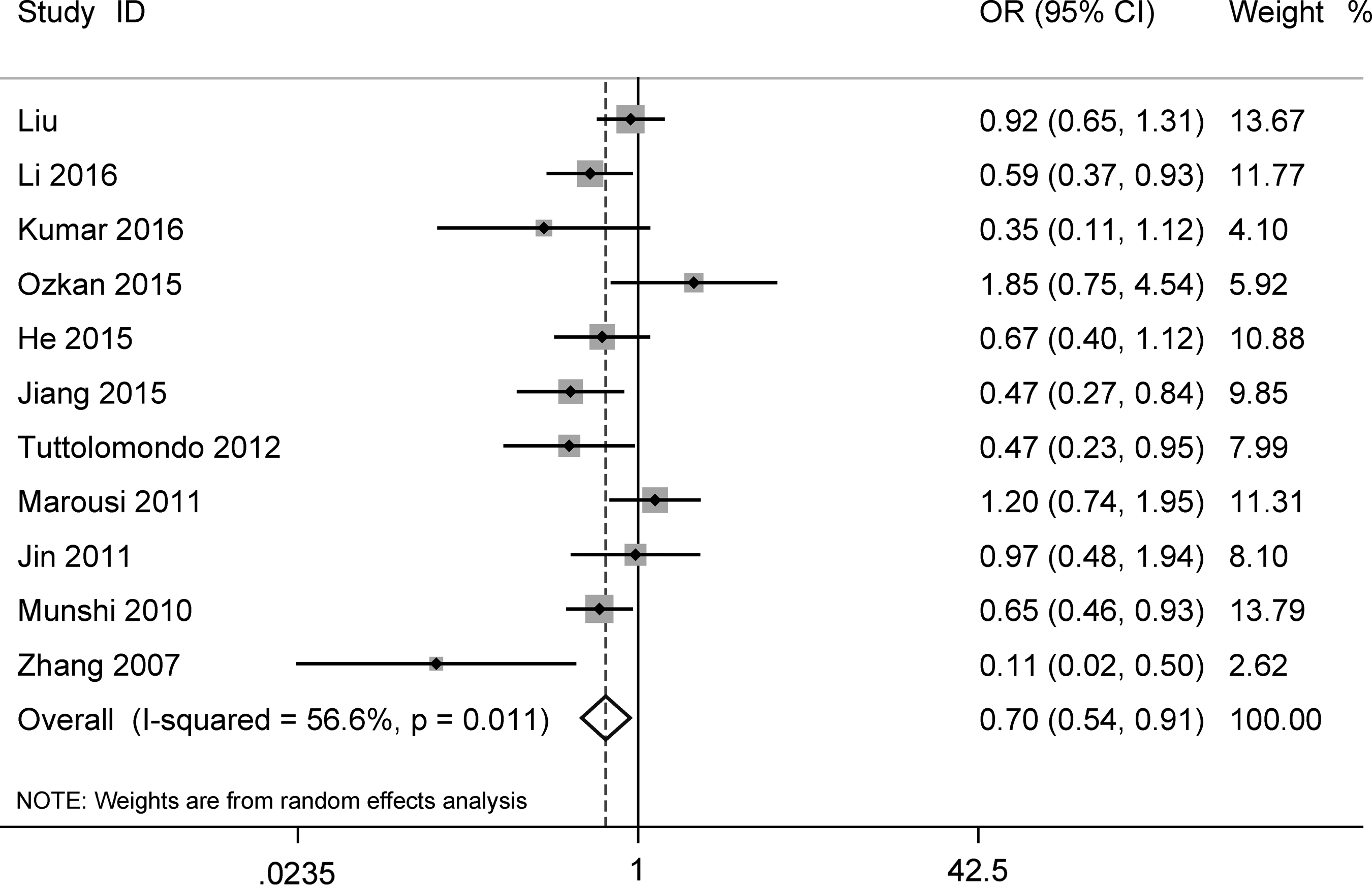
Forest plot for IL-10-1082A/G polymorphism and ischemic stroke risk under dominant model (GG+AG vs. AA).
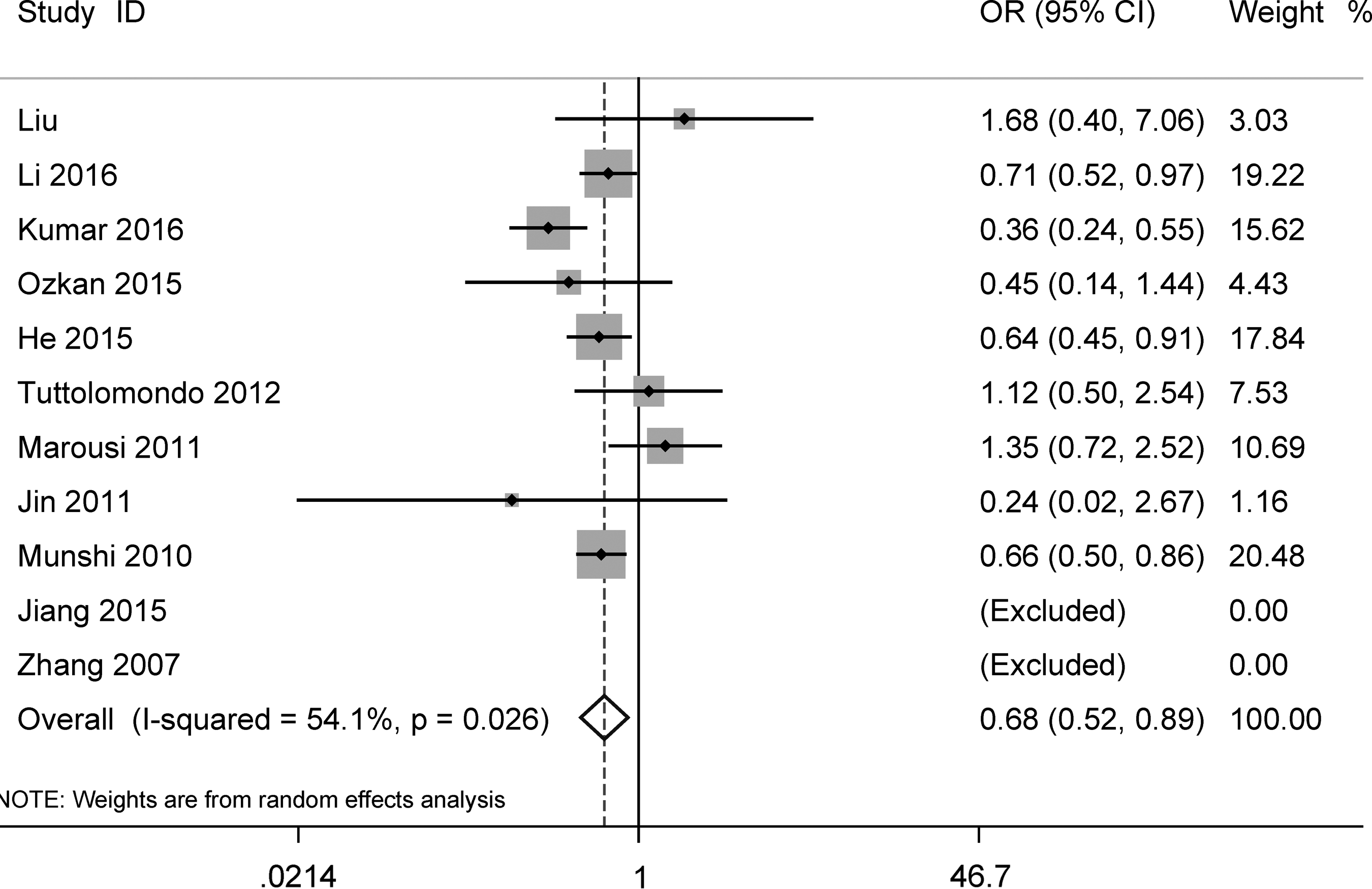
Forest plot for IL-10-1082A/G polymorphism and ischemic stroke risk under recessive model (GG vs. AG+AA).
Number of studies.
Test for heterogeneity.
Sensitivity studies were conducted to assess the effect of individual studies on pooled results. No single study significantly altered the overall ORs, which indicated the robustness of the current results (Fig. 6). As shown in Figure 7, the visual inspection of the funnel plot failed to detect significant bias. Furthermore, in Egger's regression test, there was no statistical publication bias detected (allelic model: p = 0.497, heterozygote model: p = 0.426, homozygote model: p = 0.643, dominant model: p = 0.305, recessive model: p = 0.687, respectively).
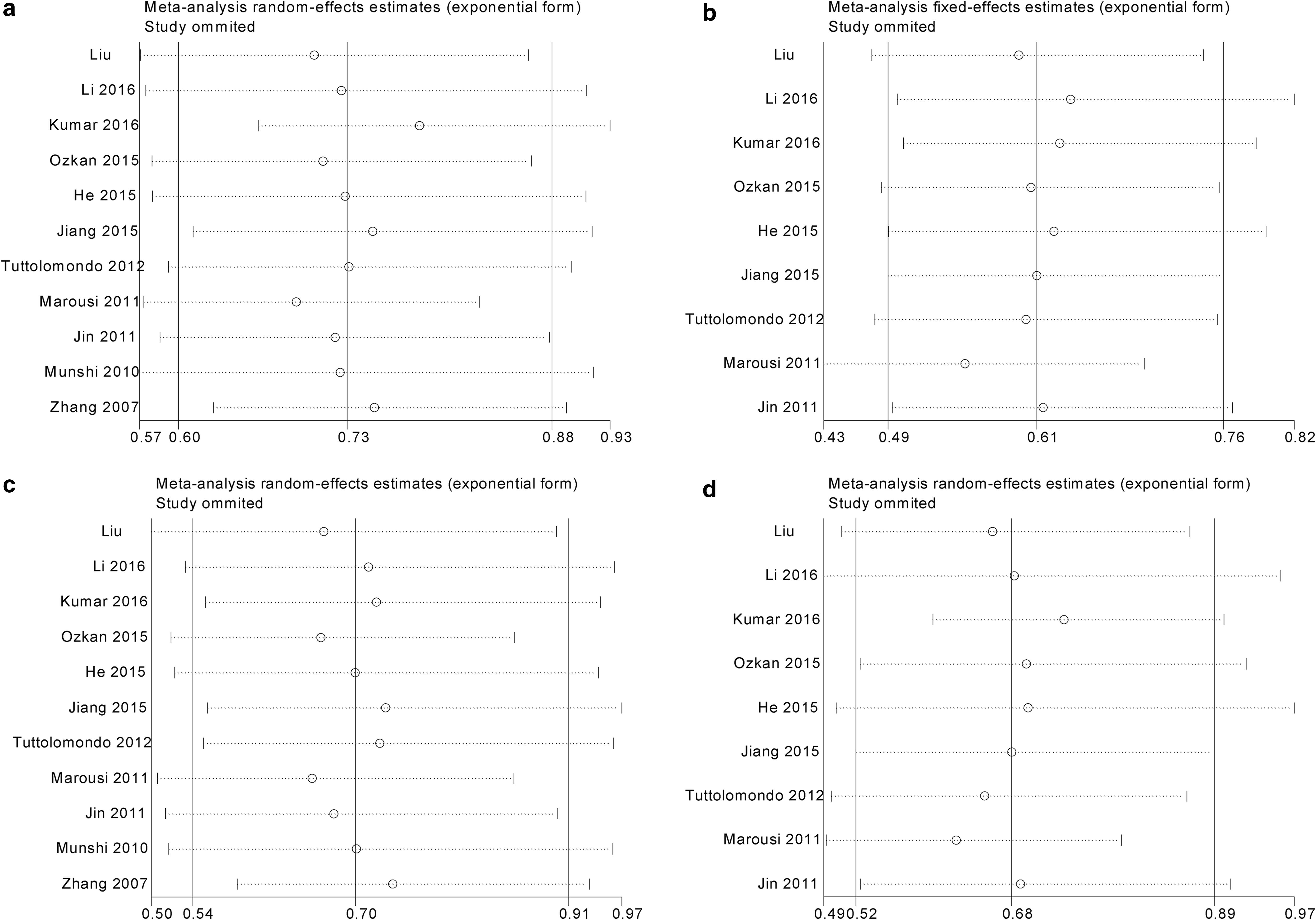
Sensitivity analysis for IL-10-1082A/G polymorphism and ischemic stroke risk.
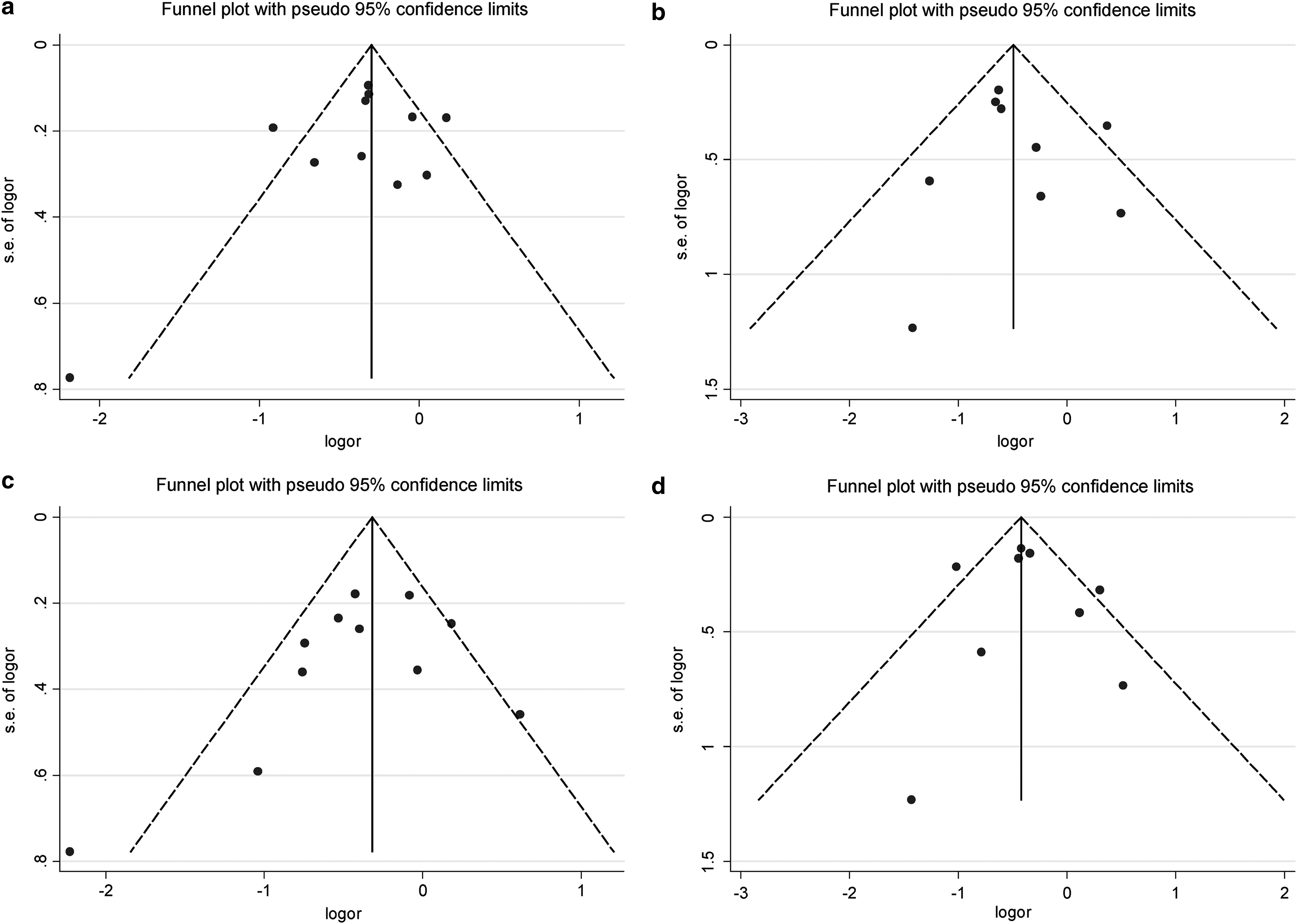
Funnel plots for IL-10-1082A/G polymorphism and ischemic stroke risk.
Discussion
To evaluate the potential association of the IL-10-1082A/G polymorphism with IS risk, we conducted a new case-control study and a comprehensive meta-analysis including 4848 subjects.
In our case-control study, we observed that the allele and genotype frequencies of IL-10-1082A/G were not associated with IS risk, which was consistent with the Greek population, as reported by Marousi et al. (2011). However, the significant association between IL-10-1082A/G and IS has been found in the Italian population (Tuttolomondo et al., 2012). Even in the Asian population, several studies have indicated the positive or null relationship of IL-10-1082A/G with IS, and the results remain controversial (Zhang et al., 2007; Munshi et al., 2010; Jin et al., 2011; He et al., 2015; Jiang et al., 2015; Kumar et al., 2016a; Li et al., 2016). The following reasons can explain the difference among research findings. First, and most significantly, the relatively small sample sizes of included studies might lead to false positive or negative results. Second, the inconsistent results could result from different genotype frequencies among enrolled subjects, especially in different ethnic groups.
By expanding the sample size, meta-analysis has the ability to detect small genetic effects in association studies. Therefore, we conducted this comprehensive analysis of 11 studies to derive a more convincing estimation. In our meta-analysis and subsequent subgroup analyses, we found some significant associations of IL-10-1082A/G with IS risk. Although the number of included studies was limited, we believe that our findings could be helpful to clarify the association. First, by performing sensitivity analysis, we found that no single study was completely responsible for the pooled result. Second, no apparent publication bias was detected by the funnel plot or Egger's regression test. Third, we performed a more comprehensive subgroup analysis. In the analysis based on ethnic diversity, we revealed a decreased risk for IL-10-1082A/G in the Asian population. Meanwhile, significant decreased risks were also observed in large sample-size studies, age- and sex-matched studies, as well as high-quality studies.
In 2014, Jin et al. (2014) performed a similar meta-analysis, including three studies in Chinese, two in Indians, and two in Caucasians. They found no significant association between IL-10-1082A/G and IS susceptibility. Subsequently, in 2016, Kumar et al. (2016b) conducted another meta-analysis, including three studies in Indians and two in Caucasians, and revealed a similar result. However, our meta-analysis demonstrated the significant association of IL-10-1082A/G with IS in four genetic models. The discrepancy between our findings and two previous meta-analyses may be due to the following reasons. Our meta-analysis had a larger sample size: We added our own study and three recent studies, including 1023 IS patients and 1029 controls, which were not part of the previous meta-analyses (He et al., 2015; Ozkan et al., 2015; Li et al., 2016). Meanwhile, we deleted two studies with a low quality, whose controls' genotype frequencies deviated from HWE (Sultana et al., 2011; Tong et al., 2016).
Till date, this is the largest and latest meta-analysis that has focused on the association of IL-10-1082A/G polymorphism with IS risk. However, several limitations need to be taken into account: First, the heterogeneity among studies existed in four genetic models: G vs. A, AG vs. AA, GG+AG vs. AA, and GG vs. AG+AA. We performed subgroup analyses to explore the source of heterogeneity, which often came from study design difference, measurement error, and ethnicity diversity (Thompson, 1994). However, none of subgroup analyses eliminated the heterogeneity effectively, which suggested that all the factors mentioned earlier should be considered. Second, most of the subjects in our meta-analysis were Asians, which limited the general application of our results to other ethnic populations. Third, different genetic polymorphisms can predispose to different subtypes of IS (Holliday et al., 2012). So far, only two studies exploring the association of IL-10-1082A/G with IS subtypes have been conducted (Munshi et al., 2010; Kumar et al., 2016a). Data were insufficient to analyze the influence of IL-10-1082A/G on IS subtypes.
Conclusions
In conclusion, our study indicates that the IL-10-1082A/G polymorphism is associated with IS susceptibility, with stronger evidence compared with the previous meta-analyses and case-control studies. Given some shortcomings in our case-control study and meta-analysis, future well-designed studies with larger sample sizes focusing on more ethnic groups are necessary to confirm our findings.
Footnotes
Acknowledgment
This work was supported by grants from the National Natural Science Foundation of China (Grant No. 81400950, 81501006).
Author Disclosure Statement
No competing financial interests exist.