
Abstract
Objective:
Asthma is the most common chronic pulmonary disease in China and is characterized by airway inflammation and episodic airflow obstruction. The aim of this meta-analysis was to evaluate the relation of two transforming growth factor-β1 (TGF-β1) polymorphisms with asthma risk in Chinese population.
Methods:
PubMed, Springer, EMBASE, MEDLINE, CNKI (China National Knowledge Infrastructure), and Wanfang databases were used to search and retrieve relevant eligible case-control studies published through December 2017. The odds ratios (OR) and 95% confidence intervals (CI) were used to evaluate the effect.
Results:
A total of 2040 asthma patients and 1952 controls from 12 studies were analyzed. Two polymorphic sites of TGF-β1 gene were identified: −509C/T and +869T/C. We found that the −509C/T polymorphism was associated with increased asthma risk under the heterozygous model (CT vs. CC: OR = 1.40, 95% CI = 1.03-1.90, p = 0.03) and the dominant model (TT+CT vs. CC: OR = 1.41, 95% CI = 1.05-1.90, p = 0.02). Subgroup analyses by age suggested that −509C/T variant was associated with childhood asthma. Analysis of disease severity indicated that this variant was associated with both mild-to-moderate asthma and severe asthma. However, the +869T/C polymorphism was not associated with asthma susceptibility in subgroup analysis by age or disease severity.
Conclusions:
This study demonstrated that the −509C/T polymorphism of the TGF-β1 gene might be a risk factor for asthma in the Chinese population, especially in Chinese children. Further large-scale case-control studies are still required.
Introduction
A
In China, about 30 million people have been affected by asthma, and a higher mortality has been reported in Chinese patients (Chen et al., 2013). Moreover, the incidence of asthma in China has dramatically increased 40% in the past 5 years, and prevalence in some cities reaches about 11% (Xu and Hsu, 2016). Besides, the prevalence of asthma obviously varies among different regions and populations in China: the prevalence of childhood asthma are widely varied, ranging from 1.1% in Lhasa to 11.0% in Hong Kong (Yangzong et al., 2012), and the prevalence of adult asthma in local area is reported as 0.7-3.8% (Song et al., 2014). Comparing with Global Initiative for Asthma (GINA) guidelines, despite the situation of asthma control been improved in China, there is still a considerable gap (Su et al., 2014).
For example, about 20% of Chinese pediatric asthma patients and half of the adult asthma patients had uncontrolled asthma (Zhong et al., 2016). Although the GINA recommends a stepwise therapeutic management strategy for asthma patients, evidences have suggested that the available therapeutic strategies are inadequate in ∼20% of patients with severe asthma, and an increase in incidence of asthma cases is associated with the treatment (Dilokthornsakul et al., 2016). Hence, identification of several new biomarkers to predict asthma occurrence and guide the therapeutic strategy is urgent.
Asthma is a heterogeneous disease (Weiss, 2001), and genome-wide association studies have determined a strong genetic basis and identified several genetic loci associated with the susceptibility in patients (Vahedi et al., 2014). Transforming growth factor-β (TGF-β) gene is located in human chromosome 19q13.1-13.3. TGF-β, as a multifunctional cytokine, is a classical growth and differentiation factor in TGF-β family, and plays important roles in inflammatory immune responses (Sanjabi et al., 2017). It is involved in the regulation of various cell behaviors, including regulation of immune system, cell growth, cell proliferation and differentiation, wound healing, apoptosis, and pathology (Morikawa et al., 2016). The TGF-β family includes three isoforms containing TGF-β1, TGF-β2, and TGF-β3. These cytokines show similar biological activity but have distinct expression patterns (Travis and Sheppard, 2014).
TGF-β1 reveals both proinflammatory and anti-inflammatory activities. High levels of TGF-β1 are associated with many fibrotic diseases, which is also used to characterize the regions of fibrosis/remodeling in all tissues (Borthwick and Wynn, 2015). In asthma patients, increased TGF-β1 expression and signaling has been detected in the airway cells, indicating the potential role of TGF-β1 in asthma development (Howell and McAnulty, 2006). Some single nucleotide polymorphisms (SNPs) in exons, introns, and promoter regions have been reported in TGF-β1 gene. The most studied variants were −509C/T (rs1800469), +869T/C (rs1982073, a Leucine to Proline substitution at amino acid position of 10), and +915G/C (rs1800471, an Arginine to Proline substitution at amino acid position of 25). TGF-β1 polymorphisms are related with increased TGF-β1 levels (Costa et al., 2013), and are associated with severity of asthma, the underlying airway inflammation and airway remodeling (Ierodiakonou et al., 2013).
The role of TGF-β1 polymorphisms in asthma risk in different populations has been studied; however, the results remain inconclusive. Salam et al. showed that children with the −509TT genotype had a 1.8-fold increased risk of early persistent asthma in California (Salam et al., 2007), where de Faria et al. (2008) suggested that no association existed between the −509C/T polymorphism and children with severe asthma in Brazil. In addition, ethnicity and demographic and environmental factors might be responsible for the diverse variations of worldwide prevalence (Anandan et al., 2010), and a series of studies have shown that genetic polymorphism might be one of the possible reasons for these differences (Wei and Deng, 2012). Therefore, this meta-analysis was performed to re-evaluate all the published case-control studies and obtain relatively reliable results regarding the association of TGF-β1 genetic polymorphisms with asthma susceptibility in the Chinese population.
Materials and Methods
Screening of relevant studies
An overall references search was performed in the online database of PubMed, Springer, MEDLINE, EMBASE, CNKI (China National Knowledge Infrastructure database), and Wanfang to retrieve relevant articles published updated to December 2017. The MeSH terms were: “asthma or asthmatic,” “cytokines,” “transforming growth factor-β1 or TGF-β1,” “Chinese population,” “polymorphism or variant,” and all the possible combinations. The corresponding Chinese terms (language) were applied for searching in Chinese databases. The references in the retrieved articles were manually screened. The search for relevant studies concerning Chinese population was carefully carried out. If there are similar studies that are performed by same authors at different times, we only choose the recent studies.
Standards for inclusion and exclusion
The inclusion standards contain: (1) case-control studies evaluating the association between TGF-β1 polymorphisms and asthma risk in the Chinese population; (2) the definition of asthma patients is in compliance with the guidelines of the American Thoracic Society: two or more episodes of shortness of breath, tachypnea and wheezing during the past years, reversibility of the wheezing and dyspnea either spontaneously or by bronchodilator treatment; (3) controls should be ethnic-matched individuals with no respiratory clinical signs or history of asthma-related diseases; and (4) genotype information in patients and controls are able to be obtained. The exclusion standards are: (1) having no control group; (2) conference reports or review reports without fully available information; (3) data cannot be obtained; and (4) with repeated information and data.
Data extraction
According to the information and descriptions supplied by each selected trial, two authors independently estimated the quality of the extracted case-control studies. Any discordance was solved by careful discussion with other authors. The following detailed information was extracted from the selected articles: first author, publication year, mean age, sample size, genotype distributions in cases and controls, genotyping methods, and the Hardy-Weinberg equilibrium (HWE) in controls.
Statistical analysis
Statistical analysis was carried out by Review Manager Software (version 5.3). The overall relation of TGF-β1 polymorphisms with asthma risk among Chinese population was calculated by odds ratios (ORs) and 95% confidence interval (CI). The significance of the pooled ORs was analyzed by the Z test; for all analyses, p < 0.05 was defined as significant. For each SNP, the allelic model, homozygous model, heterozygous model, dominant model, and recessive model were examined to evaluate its effect. The between-study heterogeneity was defined through I2 test and the Q-statistic test. The fixed effect was used when p value was more than 0.10 for the Q-test and I2 was less than 50% for the I2 test; otherwise, the random-effects model was chosen. To assess whether our results were obviously affected by any individual study, a sensitivity analysis was further performed by systematically omitting each study and recalculating the significance of the results. The evidence of publication bias was determined by visual funnel plot inspection.
Results
Main characteristics of eligible studies
We obtained 132 available articles after searching the online databases based on the MeSH terms. According to the inclusion and exclusion standards, a total of 12 articles containing 2040 asthma patients and 1952 controls were finally screened out. As shown in Figure 1, the flow chart showed the selection process of the case-control studies. Five articles (Mak et al., 2006; Lv et al., 2009; Yang et al., 2011; Chiang et al., 2013; Li et al., 2014) were written in English and others (Lu et al., 2004; Xia et al., 2006; Liu, 2008; Zhang, 2008; Dai et al., 2010; FENG et al., 2012; Zhang et al., 2013) were in Chinese. Seven were conducted in Chinese children and five were conducted in Chinese adults. Ten were conducted in Mainland China, one was carried out in Hong Kong, and one was in Taiwan. The sample size ranged from 90 to 670. Three polymorphic sites, −509C/T, +869T/C, and +915G/C of TGF-β1 gene were identified. The SNPs were measured in two genotyping methods, polymerase chain reaction-restriction fragment length polymorphism and MassArray SNP genotyping system. For +869T/C polymorphism, distribution of genotypes in controls was all consistent with HWE (p > 0.05); for −509C/T polymorphism, three studies significantly deviated from HWE (p < 0.05) (Lv et al., 2009; Dai et al., 2010; Chiang et al., 2013). For +915G/C polymorphism, there were only two relevant studies concerning the effect of this genetic polymorphism in asthma risk. Results from such small samples might influence its reliability. Hence, we did not conduct the statistical analysis for this genetic polymorphism. The main characteristics of the included case-control studies are shown in Table 1.
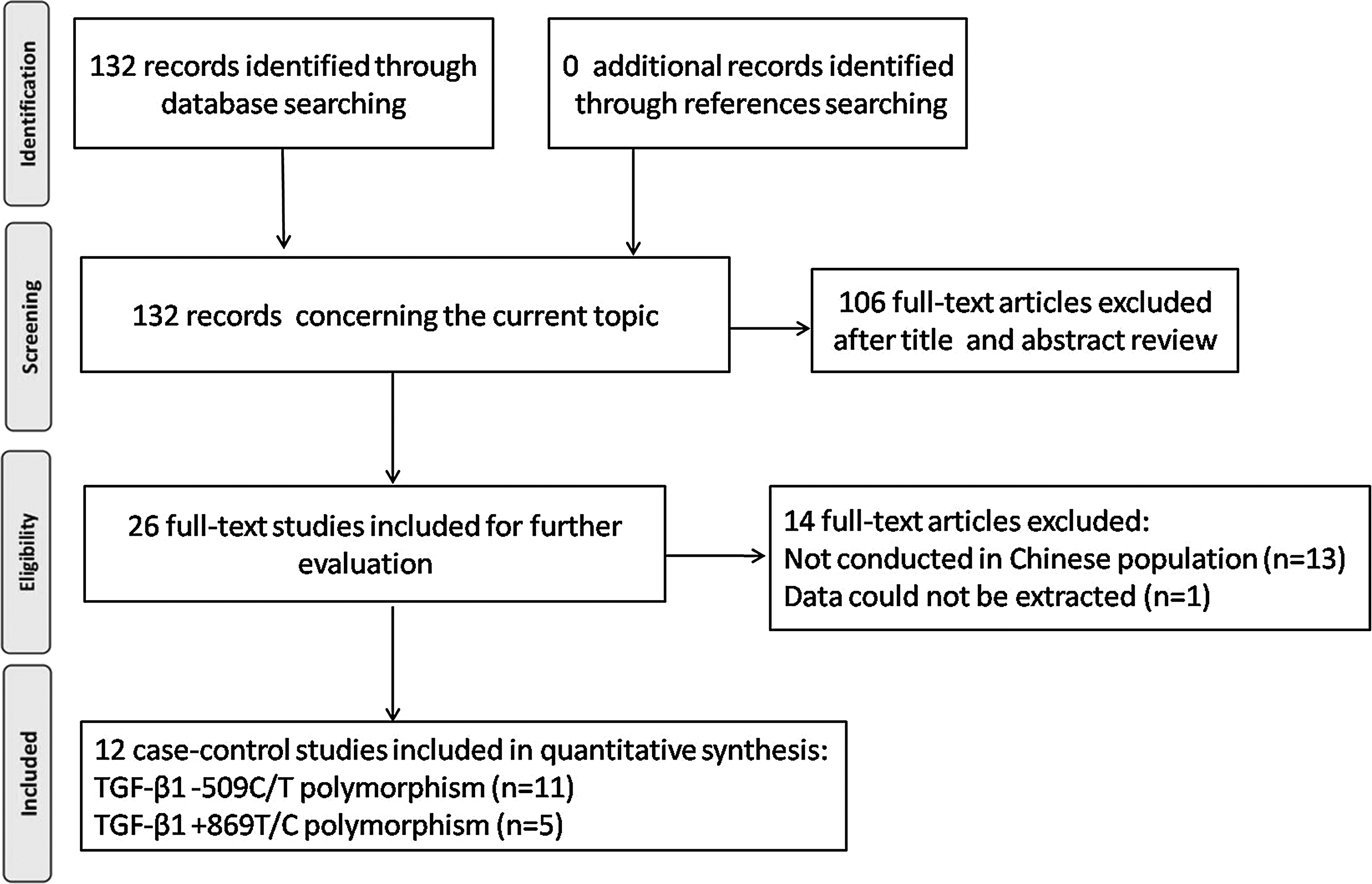
Flow diagram of selection process of the case-control studies.
HWE, Hardy-Weinberg equilibrium; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; —, no data available; SNP, single nucleotide polymorphisms.
Association of TGF-β1 − 509C/T polymorphism with asthma susceptibility in Chinese population
Table 2 listed the summary of TGF-β1 − 509C/T and +869T/C polymorphisms in asthma susceptibility in Chinese population. Eleven articles (six were conducted in children and five were in adults) containing 1933 asthma patients and 1842 controls were used to evaluate the association between −509C/T variant and asthma risk. As shown in Figure 2, compared with the controls, −509C/T polymorphism of TGF-β1 gene was significantly associated with increased asthma development under the heterozygous model (CT vs. CC: OR = 1.40, 95% CI = 1.03-1.90, p = 0.03) and dominant model (TT+CT vs. CC: OR = 1.41, 95% CI = 1.05-1.90, p = 0.02) in the random-effects model. This means that there is a 1.40-fold and 1.41-fold increase of asthma incidence in CT genotype and TT+CT genotype than that in the wild-type CC, respectively. The possible reason for the presence of between-study heterogeneity in the comparisons might be the difference of genetic distribution between individuals. Therefore, the random-effects model was employed to solve this problem. But this significant association was not detected in other genetic models (T vs. C: OR = 1.14, 95% CI = 0.94-1.40, p = 0.19; TT vs. CC: OR = 1.36, 95% CI = 0.93-2.00, p = 0.12; TT vs. CT+CC: OR = 1.02, 95% CI = 0.71-1.46, p = 0.94).
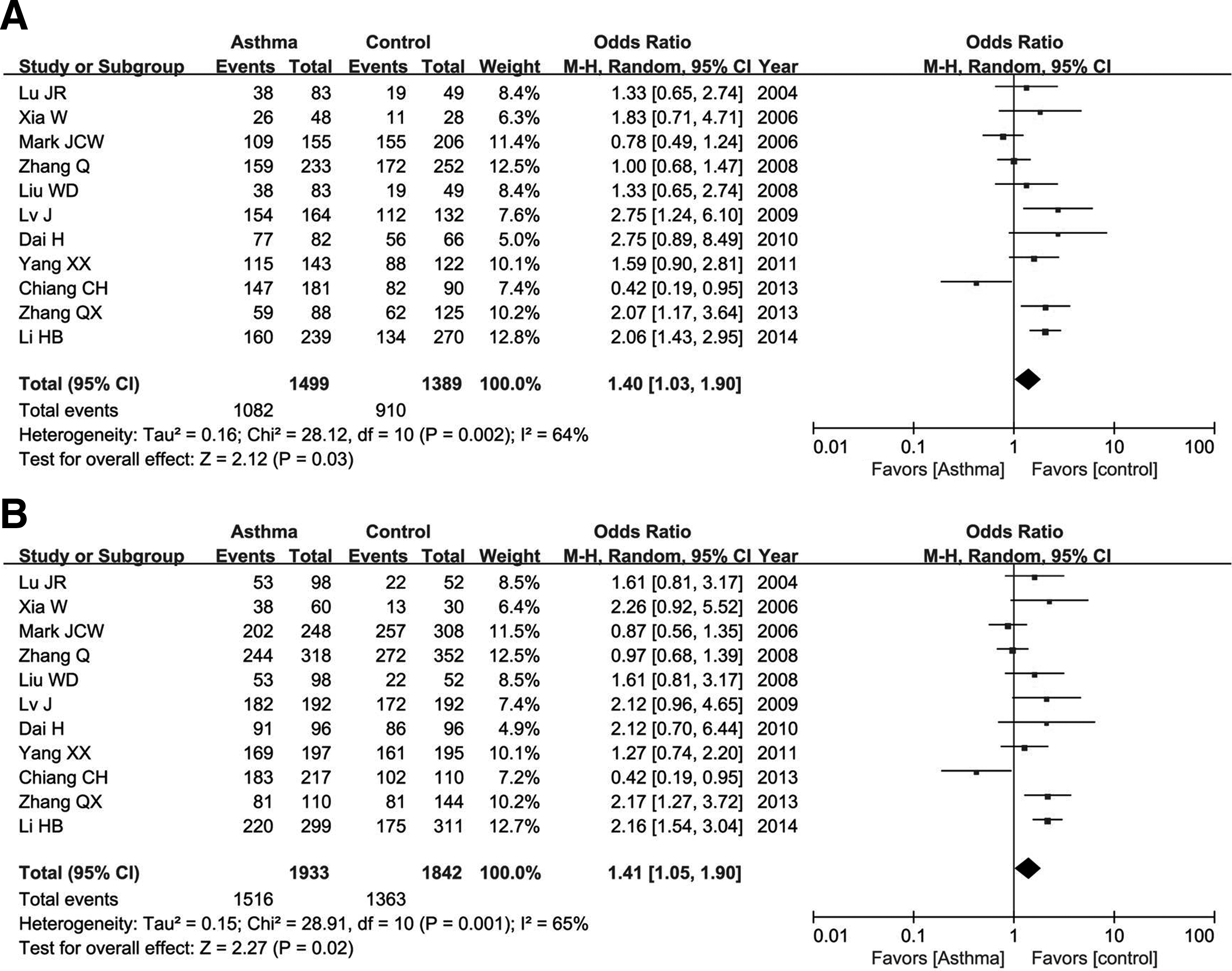
Meta-analysis of TGF-β1 − 509C/T polymorphism and asthma susceptibility in Chinese populations under the heterozygous model
The OR is the main way to quantify how strongly the presence or absence of property A is associated with the presence or absence of property B in a given population. The CI is a type of interval estimate (of a population parameter) that is computed from the observed data. The p value is the probability for a given statistical model that, when the null hypothesis is true, the statistical summary would be the same as or of greater magnitude than the actual observed results.
95% CI, 95% confidence interval; F, fixed-effects model; n, number of included studies; OR, odds ratio; ph, p value of between-study heterogeneity; R, random-effects model.
Subgroup analysis by age revealed that a significant association existed between −509C/T polymorphism and childhood asthma risk in Chinese population under the homozygous model (TT vs. CC: OR = 2.13, 95% CI = 1.53-2.96, p < 0.00001), heterozygous model (CT vs. CC: OR = 1.94, 95% CI = 1.53-2.48, p < 0.00001), and dominant model (TT+CT vs. CC: OR = 2.02, 95% CI = 1.60-2.54, p < 0.00001) in the fixed-effects model (Fig. 3). However, this genetic variant had no association with asthma risk in Chinese adults.
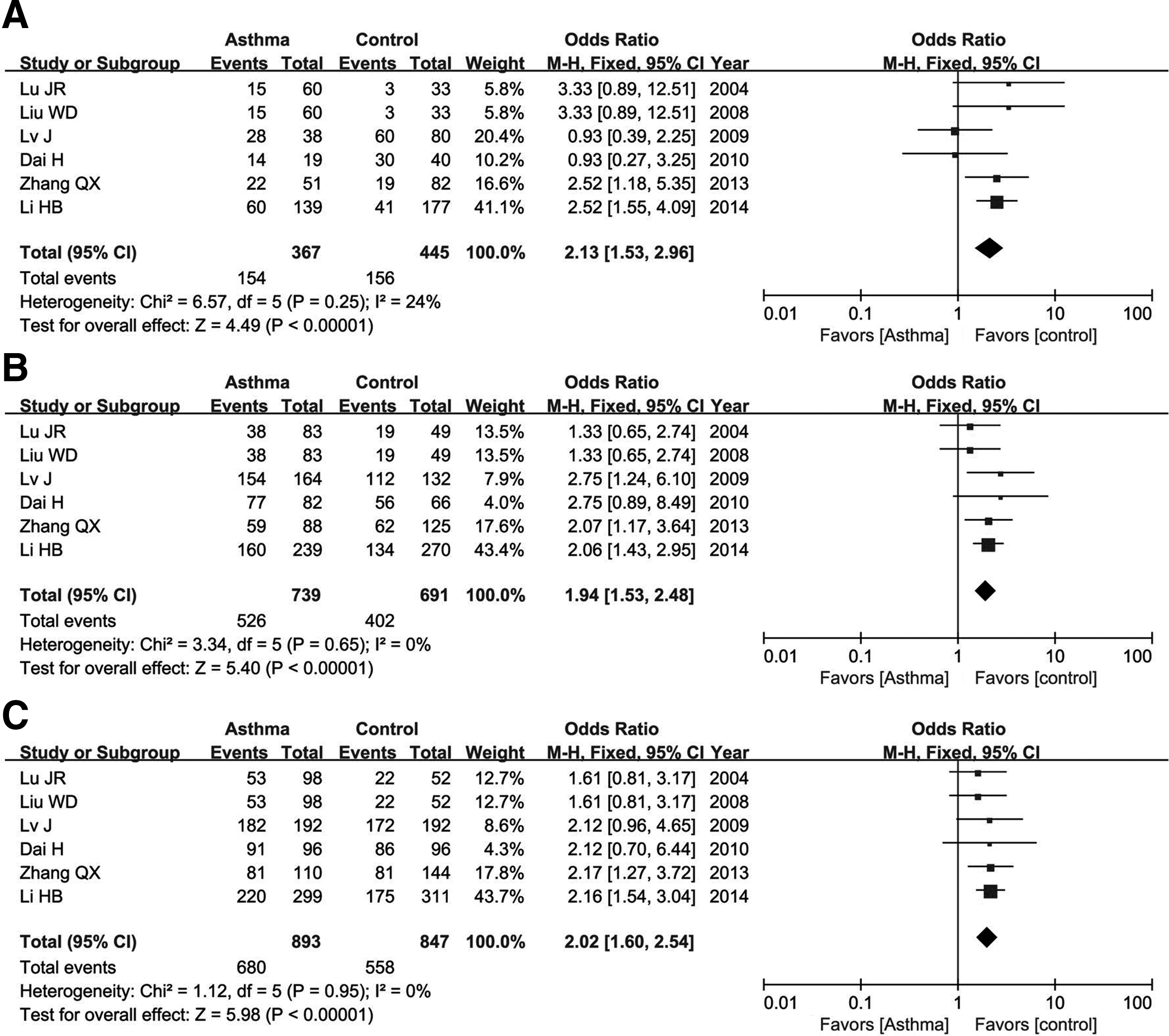
Meta-analysis of TGF-β1 − 509C/T variant and childhood asthma risk under the homozygous model
When eliminating the studies of which the genetic distributions in the controls were deviated from the HWE, we found that the −509C/T polymorphism was highly associated with asthma risk under the allelic model (T vs. C: OR = 1.31, 95% CI = 1.05-1.65, p = 0.02), homozygous model (TT vs. CC: OR = 1.66, 95% CI = 1.07-2.55, p = 0.02), heterozygous model (CT vs. CC: OR = 1.40, 95% CI = 1.05-1.86, p = 0.02), and dominant model (TT+CT vs. CC: OR = 1.47, 95% CI = 1.09-1.98, p = 0.01). Furthermore, subgroup analysis by age showed that −509C/T polymorphism had an association with an increased risk of childhood asthma under each genetic model in the fixed-effects model (T vs. C: OR = 1.66, 95% CI = 1.40-1.97, p < 0.00001; TT vs. CC: OR = 2.66, 95% CI = 1.83-3.86, p < 0.00001; CT vs. CC: OR = 1.84, 95% CI = 1.42-2.38, p < 0.00001; TT+CT vs. CC: OR = 2.00, 95% CI = 1.57-2.35, p < 0.00001; TT vs. CT+CC: OR = 1.82, 95% CI = 1.30-2.54, p = 0.0005). However, under the similar situation, this genetic variant was not associated with asthma in Chinese adults (p > 0.05).
Association of TGF-β1 + 869T/C polymorphism with asthma susceptibility in Chinese population
One thousand seventy-two asthma patients and 1207 controls from five articles (three were regarding asthma in children and two were regarding adults) were analyzed for +869T/C polymorphism of TGF-β1. The results showed that the C allele of this site had no significant association with asthma risk when compared with the T allele in the fixed-effects model (C vs. T: OR = 0.99, 95% CI = 0.88-1.11, p = 0.81). This insignificant association was also found in other genetic comparison models (CC vs. TT: OR = 0.96, 95% CI = 0.75-1.21, p = 0.71; TC vs. TT: OR = 0.98, 95% CI = 0.80-1.19, p = 0.81; CC+TC vs. TT: OR = 0.97, 95% CI = 0.80-1.16, p = 0.73; CC vs. TC+TT: OR = 0.96, 95% CI = 0.71-1.30, p = 0.81). Subgroup analysis by age indicated that no significant association existed between +869T/C polymorphism of TGF-β1 gene and asthma susceptibility in Chinese children under any genetic models (C vs. T: OR = 0.88, 95% CI = 0.74-1.05, p = 0.14; CC vs. TT: OR = 0.74, 95% CI = 0.52-1.07, p = 0.11; TC vs. TT: OR = 0.95, 95% CI = 0.73-1.24, p = 0.70; CC+TC vs. TT: OR = 0.89, 95% CI = 0.69-1.15, p = 0.37; CC vs. TC+TT: OR = 0.77, 95% CI = 0.55-1.07, p = 0.12) or in adults (C vs. T: OR = 1.10, 95% CI = 0.84-1.43, p = 0.50; CC vs. TT: OR = 1.17, 95% CI = 0.73-1.86, p = 0.51; TC vs. TT: OR = 1.01, 95% CI = 0.75-1.35, p = 0.95; CC+TC vs. TT: OR = 1.07, 95% CI = 0.81-1.40, p = 0.64; CC vs. TC+TT: OR = 1.17, 95% CI = 0.74-1.83, p = 0.51).
Association of TGF-β1 − 509C/T and +869T/C polymorphisms with different severities of asthma
According to the disease severity, asthmatic subjects could be classified into mild-to-moderate asthma and severe asthma. Concerning TGF-β1 − 509C/T polymorphism, there were 6 articles, including 551 mild-to-moderate asthma patients and 309 severe asthma patients. Our statistical analysis showed that −509C/T polymorphism significantly increased the severe asthma risk under each genetic model in the fixed-effects model when compared with the controls (T vs. C: OR = 1.82, 95% CI = 1.50-2.22, p < 0.00001; TT vs. CC: OR = 3.33, 95% CI = 2.18-5.08, p < 0.00001; CT vs. CC: OR = 2.05, 95% CI = 1.48-2.83, p < 0.00001; TT+CT vs. CC: OR = 2.36, 95% CI = 1.74-3.20, p < 0.00001; TT vs. CT+CC: OR = 1.98, 95% CI = 1.41-2.79, p < 0.0001) (Fig. 4). In patients with mild-to-moderate asthma, only T allele and TT genotype of TGF-β1 − 509C/T polymorphism were associated with asthma risk (T vs. C: OR = 1.36, 95% CI = 1.16-1.59, p = 0.0001; TT vs. CC: OR = 1.64, 95% CI = 1.18-2.28, p = 0.003; TT vs. CT+CC: OR = 1.51, 95% CI = 1.15-1.99, p = 0.003) (Fig. 5).
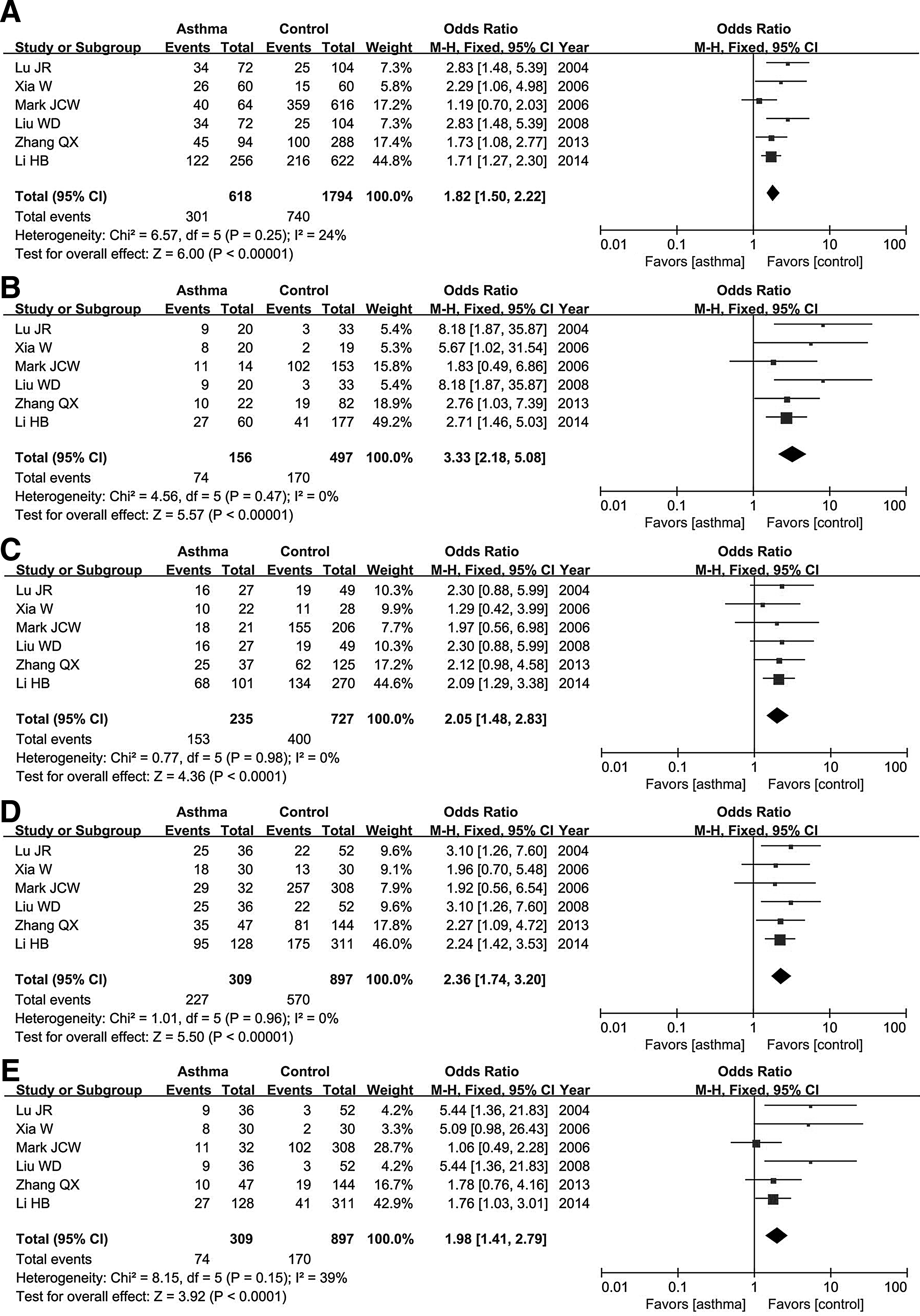
Association of TGF-β1 − 509C/T polymorphism in severe asthma risk under the allelic model

Association of TGF-β1 − 509C/T polymorphism in mild-to-moderate asthma risk under the allelic model
As for TGF-β1 + 869T/C polymorphism, three articles contained 398 patients with mild-to-moderate asthma and 205 patients with severe asthma. The results showed that +869T/C polymorphism had no association with the mild-to-moderate asthma or the severe asthma (p > 0.05, Table 2).
Association of TGF-β1 − 509C/T, +869T/C polymorphisms with serum levels of TGF-β1 (ng/mL) in asthma patients
Four articles reported the effect of −509C/T and +869T/C variants in serum levels of TGF-β1 in asthma patients. However, the available data could only be extracted from two articles, containing 157 asthma patients. Our results showed that these two genetic polymorphisms had no association with serum level of TGF-β1 in asthma patients in the random-effects model (TT+CT vs. CC: OR = 5.71, 95% CI = −3.59-15.01, p = 0.23 for −509C/T variant; CC+TC vs. TT: OR = −2.21, 95% CI = −9.07-4.64, p = 0.53 for +869T/C variant).
Sensitivity analysis and publication bias
We conducted a sensitivity analysis to estimate if our results were substantially affected by the presence of any individual study. Each included study was deleted at every turn and the significance of the results was recalculated. Our results suggested that the pooled ORs were not significantly influenced. The funnel plot was applied to evaluate the publication bias, and the shape of the funnel plot was symmetrical, further indicating that no publication bias existed in this meta-analysis (Fig. 6).
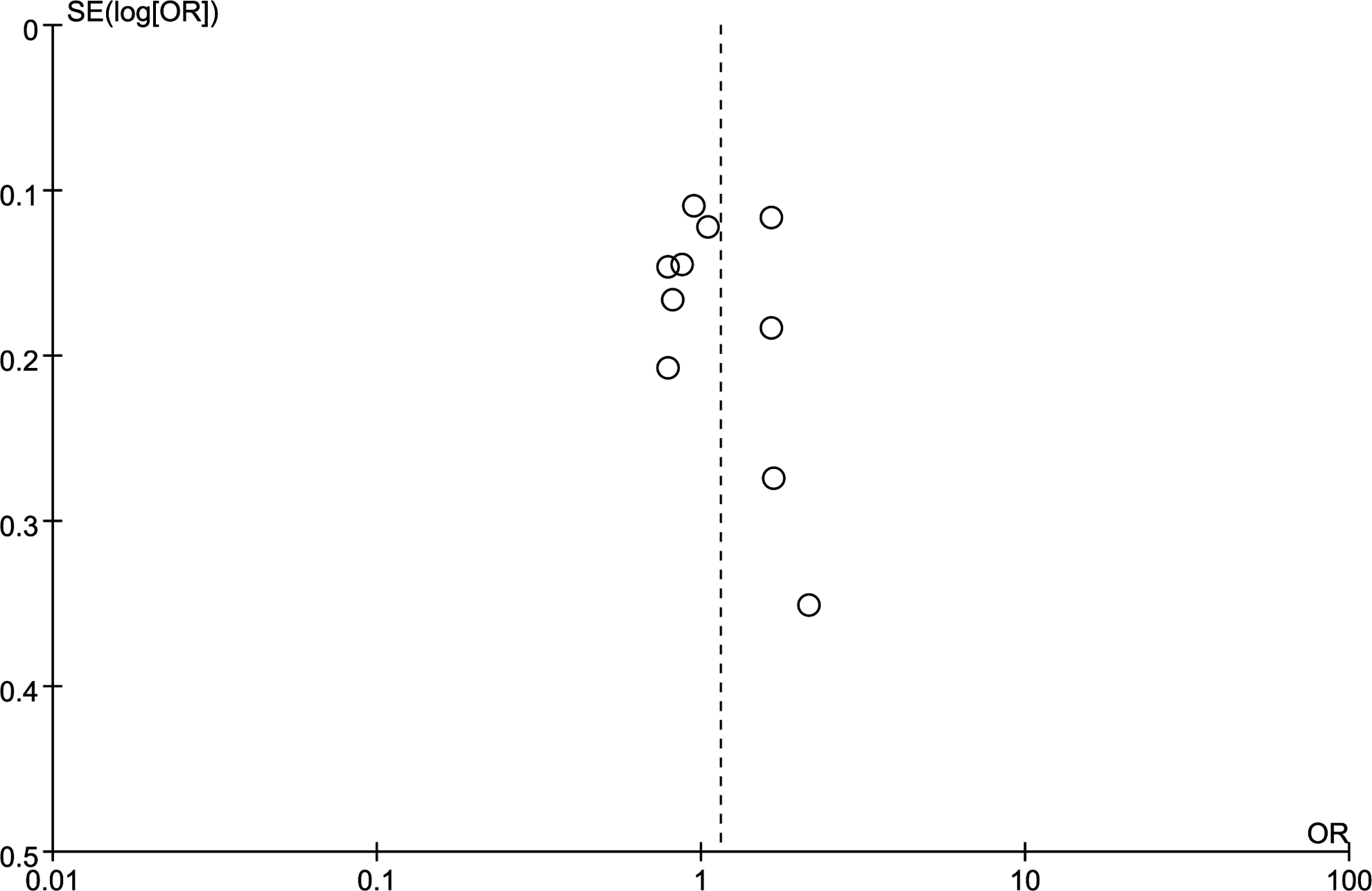
Funnel plot of association between TGF-β1 − 509C/T polymorphism and asthma risk in total populations under the allelic model.
Discussion
This meta-analysis totally included 12 case-control studies. The results suggested that the TGF-β1 − 509C/T polymorphism was associated with increased asthma risk under the heterozygous model and dominant model. Subgroup analysis by age revealed that −509C/T polymorphism was highly associated with the asthma risk in Chinese children under the homozygous model, heterozygous model, and dominant model, but this genetic polymorphism had no association with adult asthma. Subgroup analysis by asthma disease severity showed that −509C/T polymorphism was associated with both the mild-to-moderate asthma and severe asthma. However, +869T/C polymorphism had no association with asthma susceptibility in subgroup analysis by age or disease severity. Our results were not consistent with previous meta-analysis carried out by Li et al., which only included three case-control studies and believed that TGF-β1 − 509C/T had no association with asthma risk in Chinese population (Li et al., 2010).
Asthma imposes significant impacts on individuals, families, and societies. Its prevalence ranges from 1% to 18% of the population in different countries (FitzGerald et al., 2015), causing a significant health burden (Croisant, 2014). Even so, the preventive strategies and treatments for asthma are not well employed and established (Chen and Lin, 2008). Only a few of asthma patients get appropriate and better treatment. Poverty and inadequate medical resources have contributed to the consistent prevalence of this disease in China especially in the underdeveloped regions. Therefore, the potential effective approach to prevent the prevalence of asthma might modify the risk factors of asthma.
Increasing studies have shown that asthma is a familial and hereditary disorder in the pathogenesis of which genetic and environmental factors play significant roles (von Mutius, 2009). Genetic predisposition is considered as one of the crucial determinants to asthma susceptibility (March et al., 2011), and 35-80% of the variation in asthma risk is attributable to the genetic variation (Gerasimova et al., 2013). However, most asthma genes are not replicable across populations, which is possibly due to the difference in genetic risk alleles among different populations, and differences in the epidemiology of these genes (Chen et al., 2016). Lack of replication might reflect the genetic heterogeneity underlying the asthma phenotype. Previous studies have found the differences in allele frequencies of asthma genes and haplotype structures of asthma loci between Chinese population and other populations (Leung et al., 2014). In addition, environmental factors are clearly important in the pathogenesis of asthma, and genes affected by environment are often included in genetic studies (Akhabir and Sandford, 2011).
TGF-β1, as a multifunctional cytokine, plays significant regulative roles in several biological processes, including cell growth, development, transformation, fibrosis, tissue repair, and inflammatory responses (Blobe et al., 2000). Altered TGF-β1 expression might influence a wide variety of normal cellular and disease processes (Shah et al., 2006). In asthma patients, the levels of TGF-β1 in the airways of asthmatics are obviously higher than that in the normal subjects. Polymorphisms in the TGF-β1 gene are deemed to be associated with functional implications: some polymorphisms affect TGF-β1 expression; some interfere with transcriptional regulation by affecting the binding of transcription factors binding, whereas others interfere with protein production (Martelossi Cebinelli et al., 2016). Some of these polymorphisms may affect asthma phenotypes, thus functioning as susceptibility biomarkers. The −509C/T polymorphism site is located in TGF-β1 gene promoter region, and might alter TGF-β1 promoter-reporter activity and influence the interaction of the promoter region with the transcription factor Yin Yang 1, which finally lead to varied circulating concentrations of TGF-β1 in plasma (Silverman et al., 2004). Several studies have found that TGF-β1 − 509C/T polymorphism had significant association with increased serum levels of TGF-β1 in asthma patients (Nagpal et al., 2005). This genetic polymorphic site is also deemed as a factor that is associated with increased asthma risk (Yao et al., 2016). Moreover, the −509T variant on haplotype 1 is the most informative marker of the TGF-β1 that is correlated with the asthma severity (Pulleyn et al., 2001). These results indicate that −509C/T polymorphism may enhance TGF-β1 gene transcription and it might be a potential factor that can be used in asthma diagnosis.
The +869T/C polymorphism site of TGF-β1 is located in the signal peptide coding region, which is thought to target the newly synthesized protein to the endoplasmic reticulum (Buckova et al., 2001). This variant may influence the functions of the signaling peptide of TGF-β1, most likely having influences on the intracellular trafficking or exporting efficiency of cellular proteins. The +869T/C polymorphism may play an important regulative role in TGF-β1 mRNA expression (Mak et al., 2006). The T allele has been demonstrated to be associated with decreased expression of TGF-β1, whereas the C allele has shown a 2.8-fold higher secretion of TGF-β1 than the T allele (Dunning et al., 2003). The allele 869T may result in the lower cellular protein exporting efficiency and lead to the reduction of protein production. The C allele is also associated with the high serum concentrations of TGF-β1 (Yokota et al., 2000). Studies have shown that +869T/C polymorphism might be involved in the modulation of asthma severity (de Faria et al., 2008), indicating that this variant might influence asthma susceptibility and development.
Although we have carefully evaluated the association of TGF-β1 with asthma risk, several limitations remain presented in this meta-analysis. First, the number of included studies was still relatively less. Second, the between-study heterogeneity was high in some genetic comparison models, which might influence the results. Third, all the included studies were performed in Chinese populations, whereas other ethnicities should be further considered. Fourth, the genetic distributions of the controls and cases in three included studies were deviated from the HWE. The mutation features for this certain genetic polymorphism might be the possible cause. Although deviations from HWE in control subjects may bias the estimates of genetic effects in meta-analysis, our results showed that elimination of these studies from analysis did not significantly influence the overall results. Lastly, asthma is highly associated with the complicated gene-gene and gene-environment interactions, hence the interaction of gene-gene and gene-environment should be considered.
In conclusions, our results suggest that −509C/T polymorphism of TGF-β1 gene might be a risk factor in Chinese asthma patients, especially in children. Future well-designed case-control studies with more participants are still needed to further estimate the association between TGF-β1 genetic polymorphism and asthma risk in Chinese population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.