
Abstract
Aim:
The aim of this study was to investigate the association between killer cell immunoglobulin-like receptor (KIR) gene polymorphisms and unexplained recurrent pregnancy loss (URPL).
Materials and Methods:
This study included 70 URPL patients with a history of two or more miscarriages and 70 healthy multiparous women as a control group. KIR genotyping was performed in all subjects for the KIRs 2DL1-4 and 2DS1-5 genes using polymerase chain reaction with sequence-specific primers.
Results:
There was a significant relationship between the KIR genotypes and URPL. We demonstrated that the KIR 2DL1, 2DL2, 2DL3, 2DL4, 2DS1, 2DS2, 2DS4, and 2DS5 polymorphisms are associated with URPL. The 2DS3 genotype was not detected in either the case or control group. Gene-gene interactions for all genes were statistically significant. The KIR Bx genotype was found primarily in the case group, and at a higher frequency when compared with the control group. There was a significant relationship between the URPL cases and Bx haplotypes.
Conclusion:
We demonstrated that the KIR 2DL1, 2DL2, 2DL3, 2DL4, 2DS1, 2DS2, 2DS4, and 2DS5 polymorphisms are associated with URPL. The 2DS3 genotype of the KIR gene, however, was not detected in either the case or control group. The observations reported herein on KIR genotyping offer a new avenue for innovations in biomarker research concerning URPL and other complex obstetrics diseases.
Introduction
R
Evidence-based treatments such as surgical correction of uterine anomalies or aspirin and heparin for antiphospholipid syndrome have provided improved results for some couples with RPL. However, almost half of the RPL cases remain unexplained, and are treated empirically with progesterone supplementation, anticoagulation, and/or immunomodulatory drugs (Pandey et al., 2005; Rai and Regan, 2006; Beaman et al., 2012; Sugiura-Ogasawara et al., 2014; Garrido-Gimenez and Alijotas-Reig, 2015). A genetic predisposition may cause unexplained recurrent pregnancy loss (URPL), and it has been reported in several studies that this increases the risk of pregnancy loss for the siblings of URPL patients. Several candidate RPL genes have been identified. Most of these play a role in the immune response, coagulation, metabolism, or angiogenesis (El Hachem et al., 2017).
There are controversial issues regarding assisted reproduction (ART), the most prevalent being the role of the immune system in RPL and recurrent implantation failure. This controversy stems in part from the fact that the majority of previously published studies on the immune system and reproduction were designed to discover peripheral blood markers and offer rapid solutions through immunomodulation (Alecsandru and Garcia-Velasco, 2015).
Natural killer (NK) cells play a basic role in the innate immune response; this is due to their ability to secrete cytokines and kill target cells without prior sensitization. Due to their cytotoxic nature, NK cells must have the ability to recognize normal self-tissue to prevent self-destruction. Besides their role in host defense, NK cells are thought to play a critical role in pregnancy by accumulating at the maternal-fetal interface (Riley and Yokoyama, 2008). There is likely an immunological origin of RPL etiology. One hypothesis for recurrent miscarriages with an immunological origin is an improper transplantation response, which leads to an immune rejection and miscarriage of the fetus due to allogeneic antibodies in the mother that cross through placenta (Beaman et al., 2012). A new concept has arisen, which suggests that the uterine immune system uses NK cell allorecognition to regulate placentation and control the maternofetal interface (La Roccaa et al., 2014; Alecsandru and Garcia-Velasco, 2015). Killer cell immunoglobulin-like receptors (KIRs) are molecules found on NK cells that regulate their function.
The KIR locus contains remarkable haplotypic diversity among populations and a highly homologous gene family with A and B (which has more diverse repertoire of activating KIR genes) haplotypes, and maps to chromosome 19q13.4 within the leukocyte receptor complex. There are one or two immunoreceptor tyrosine inhibitory motifs in the cytoplasmic tail of KIRs; and they are able to recruit inhibitory phosphatases through their SH2 domains. The signal transduction cascade results in the inhibition of cytotoxic granule release and reduced NK cell cytotoxicity (Khakoo and Carrington, 2006; Middleton and Gonzelez, 2012; Alijotas-Reig et al., 2014; Manser et al., 2015; Dambaeva et al., 2016).
KIR ligands are members of the MHC class I alleles, and are mostly HLA-C alleles. The signaling balance between inhibitory and activation receptors determines the final result in any NK cell. Inhibitory signals generally suppress activating signals; which is how NK cells avoid killing self cells. When both the activating and inhibitory KIRs connect to their respective ligands, the inhibitory signal predominates, and the NK cell tolerates the target cell. Increased NK cell inhibition may result in an inadequate trophoblast invasion into the uterine spiral arteries. Specific combinations of maternal KIR genotypes and phenotypes and parental HLA-C genotypes are more common in women with RPL (Beaman et al., 2012). Therefore, the aim of this study was to determine if there is a correlation between specific KIR gene polymorphisms and URPL.
Materials and Methods
This study was conducted on URPL patients and healthy controls (from 2016 to 2017) who attended the Department of Obstetrics and Gynecology at the Mersin University Faculty of Medicine Hospital, Turkey. All genetic analyses were performed by the Department of Medical Biology and Genetics, Mersin University Faculty of Medicine Hospital, Turkey.
Cases and controls
The URPL patients included 70 women with a history of two or more miscarriages undergoing extended evaluation. They were assessed for chromosomal, anatomical, metabolic, hormonal, infectious, autoimmune, and thrombophilic etiologies, which were used as exclusion criteria. In the URPL patient group, the mean subject age was 29.04 years, with an average of 3.275 abortions (min = 2, max = 8, SD = 1.4841). Primary RPL subjects (n = 42, 60%) had an average of 3.195 abortions (SD = 1.5687), and secondary RPL subjects (n = 28, 40%) had an average of 3.393 abortions (SD = 1.3700). The control group consisted of 70 healthy multiparous women who had at least two healthy children with no history of miscarriages, and were of Turkish ethnogeographic origin. The mean age of control subjects was 30.88 years. All of the women in both groups were given all pertinent information about the study and gave their informed consent before participation. Ethical committee approval of the study was received from the Ethics Committee of Mersin University, Clinical Research. This study assessed appropriate female cases who were taken from a population study for the determination of KIR genes.
DNA extraction
A blood sample (5 mL) was drawn from each participant. Venous blood samples were aggregated in tubes containing ethylenediaminetetraacetic acid (EDTA). DNA was extracted from whole blood by Miller's salting out procedure.
KIR genotyping
KIR genotyping was performed using polymerase chain reaction with sequence-specific primers (PCR/SSP) in all of the recruited subjects for the following KIRs: 2DL1, 2DL2, 2DL3, 2DL4, 2DS1, 2DS2, 2DS3, 2DS4, and 2DS5. All reactions had an internal positive control composed of an extra pair of primers, specific for nonpolymorphic sequences of the growth hormone gene (GH1 gene) (Table 1). The control primers were used at a final concentration of 0.2 μM. The PCR system without DNA was used as a negative PCR control.
Primer Sequences Used for Amplification of Killer Cell Immunoglobulin-Like Receptor Genes
F, forward; PCR, polymerase chain reaction; R, reverse.
The PCRs were performed in a 50 μL volume with 100 ng DNA, 100 μM dNTPs, 20 pmol of each primer, 1 mM MgCl2, 1× PCR buffer with (NH4)SO4 (Fermentas, Vilnius, Lithuania), 0.2% (w/v) bovine serum albumin, and 1 U Taq polymerase (Fermentas). Thermocycling was performed on an automated Thermal Cycler (Techne Genius, Duxford, United Kingdom). The PCR conditions for 2DL1, 2DL2, 2DL3, and 2DL4 were as follows: 2 min at 96°C for the initial denaturation; 35 cycles of 45 s at 96°C for the denaturation, 1 min at 58°C for annealing, 2 min at 72°C for the extension; and 7 min at 72°C for the final extension. The PCR conditions for 2DS1, 2DS2, 2DS3, 2DS4, and 2DS5 were as follows: 2 min at 96°C for the initial denaturation; 35 cycles of 45 s at 96°C for the denaturation, 1 min at 60°C for the annealing, 2 min at 72°C for the extension; and 7 min at 72°C for final extension. Samples were stored at 4°C.
The PCR products, along with ∼3 μL Thermo Fisher Scientific 100 bp DNA ladder that was used as a molecular weight marker, were subjected to electrophoresis on 1.5% agarose (FMC BioProducts, Rockland, ME) gels containing 0.5 μg/mL ethidium bromide. The voltage was maintained at 100 V for 20-30 min. Gels were visualized under UV light using a gel electrophoresis visualizing system (Vilber Lourmat, Marne La Vallée, France). PCR/SSP amplification of the KIR 2DL1, 2DL2, 2DL3, and 2DL4 polymorphisms is shown in Figure 1, and amplification of the KIR 2DS1, 2DS2, 2DS3, 2DS4, and 2DS5 polymorphisms is shown in Figure 2.
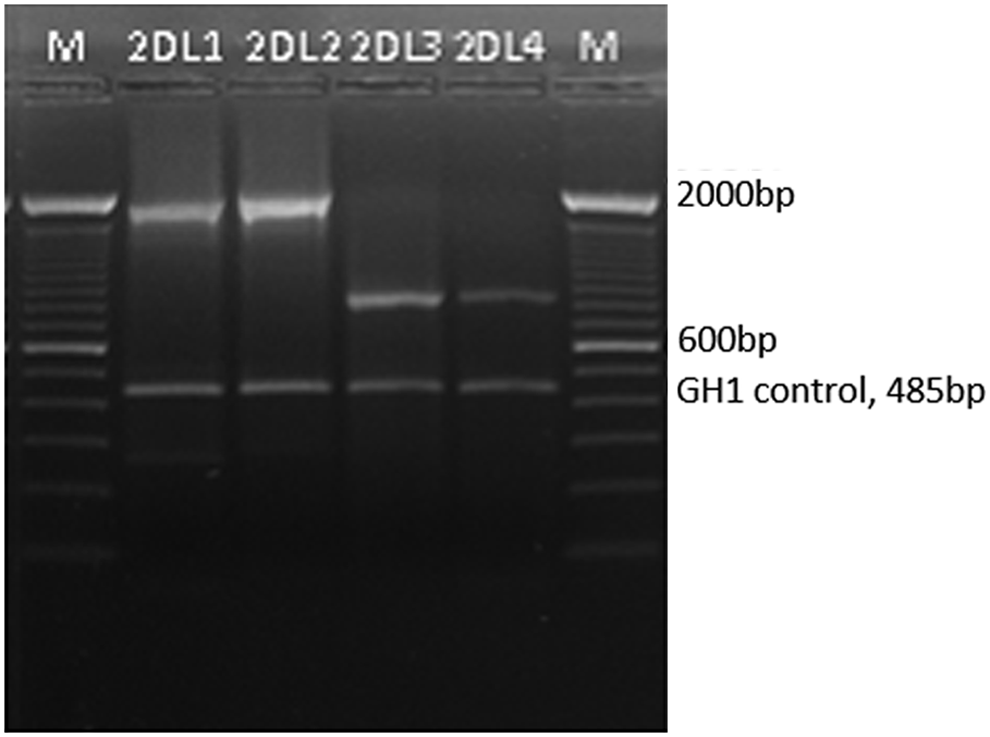
PCR/SSP amplification of KIR 2DL1, 2DL2, 2DL3, and 2DL4 (1750, 1800, 798, and 695 bp). The GH1 served as a positive marker of PCR (485 bp). M: 100-2000 bp marker. KIR, killer cell immunoglobulin-like receptor; PCR/SSP, polymerase chain reaction with sequence-specific primers.
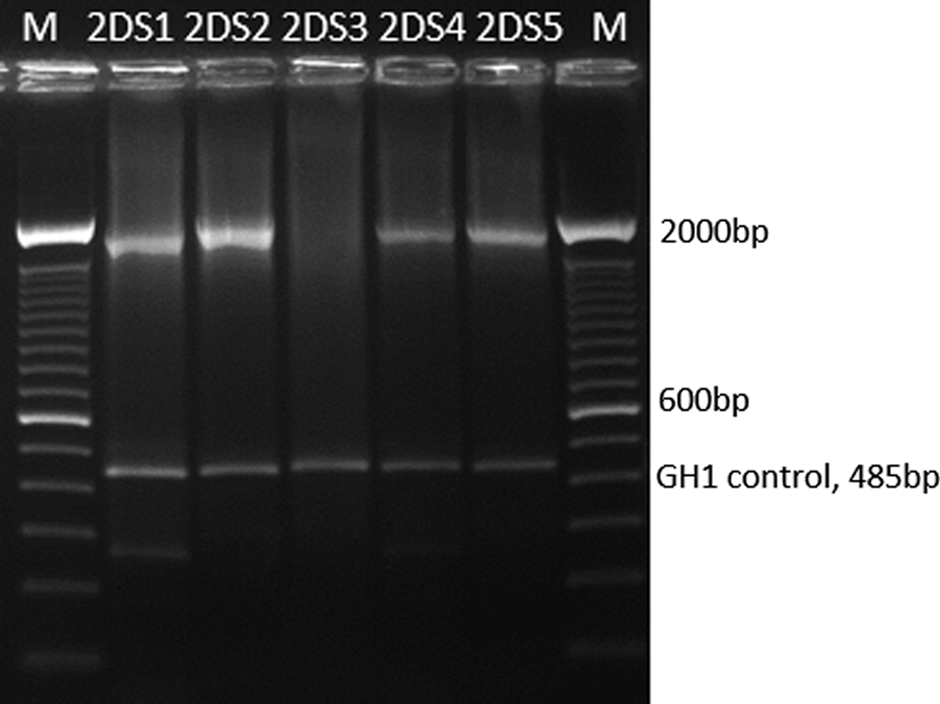
PCR/SSP amplification of KIR 2DS1, 2DS2, 2DS3, 2DS4, and 2DS5 (1800, 1750, 1800, 1800, and 1950 bp). 2DS3 was not detected. The GH1 served as a positive marker of PCR (485 bp). M: 100-2000 bp marker.
Prediction of group A and group B KIR haplotypes
If any of the genes, 2DL2, 2DL5, 3DS1, 2DS1, 2DS2, 2DS3, and 2DS5, were present, the genotype was accepted as B. When none of these were present, the genotype was accepted as AA. We did not attempt to make a distinction between the AB and BB genotypes, thus these groups were collectively called Bx (www.allelfrequencies.net).
Statistical analysis
The relationship between positivity in genes and disease was calculated by the chi-squared or likelihood ratio test. Odds ratios were calculated for significant relationships with a confidence interval (95% CI). Categorical variables were expressed as frequencies and percentages. Gene-gene interactions were calculated. For significant interactions, genes were separated into positive and negative based on the risk of disease, and then odds ratios (95% CI) were calculated for each interaction. The Mann-Whitney U test was used for comparison of the two groups. The statistical analyses were performed using MedCalc version 11.5.0. A p-value <0.05 was considered statistically significant.
Results
Using gene-specific PCR amplifications, we analyzed the presence/absence of nine KIR genes in the case and control groups. There was a significant relationship between the 2DL1, 2DL2, 2DL3, and 2DL4 polymorphisms and URPL (p < 0.001). The positivity rate of the 2DL1, 2DL2, 2DL3, and 2DL4 polymorphisms in the case group was higher than the positivity rate in the control group (7.07, 51.56, 24.00, and 8.00 times higher, respectively). There was a significant relationship between the 2DS1, 2DS2, 2DS4, and 2DS5 polymorphisms and disease (p < 0.001). The positivity rate of the 2DS1, 2DS2, 2DS4, and 2DS5 polymorphisms in the case group was higher than the positivity rate in the control group (21.78 times and p = 0.035, 30.13 times and p = 0.019, 53.39 times and p = 0.006, and 24.47 times and p = 0.028, respectively). 2DS3 was not detected in either the case or control group (Table 2).
Frequency of Each Killer Cell Immunoglobulin-Like Receptor Gene in Unexplained Recurrent Pregnancy Loss Case and Controls (2DS3 Was Not Detected in Both the Case and the Control Group)
CI, confidence interval; KIR, killer cell immunoglobulin-like receptor; OR, odds ratio.
Gene-gene interactions for all genes were statistically significant (p < 0.001 and 95% CI). Considering these interactions, positivity for the KIR genes observed in the case group is a risk factor for the disease (data not presented). The KIR Bx genotype was detected in the majority of the case group. When compared with the control population, a significant increase in the KIR Bx genotype frequency was identified in the case group, and a significant relationship was found between URPL cases and Bx haplotypes (Fig. 3). The distribution of KIR genotypes in the case and control groups is shown in Tables 3 and 4, respectively.

The distribution of KIR genotypes of URPL case and control group. URPL, unexplained recurrent pregnancy loss.
Distribution of Killer Cell Immunoglobulin-Like Receptor Genotypes in Case Group
The gray color shadings indicate gene presence and the white rectangles indicate gene absence.
Distribution of Killer Cell Immunoglobulin-Like Receptor Genotypes in Control Group
The gray shadings indicate gene presence and the white rectangles indicate gene absence.
There is no statistically significant relationship between KIR polymorphisms and the primary/secondary pregnancy loss group (Table 5). There was no statistically significant difference in the number of pregnancy losses between the 2DL1, 2DL2, 2DL3, 2DL4, 2DS1, 2DS2, 2DS4, 2DS5 polymorphisms presence/absence (p > 0.05).
URPL, unexplained recurrent pregnancy loss.
Discussion
Because the etiology is usually not known and evidence-based diagnostic and treatment strategies are limited, URPL is seen as an important and devastating medical problem in reproductive medicine. Couples with RPL need to know the reason this disease occurs and what the risk of a recurrence is. Genetic, endocrine, anatomical, immunological, thrombophilic, and environmental factors are the common etiological categories of URPL (Garrido-Gimenez and Alijotas-Reig, 2015). While a patient is evaluated, the doctor should take into consideration the disease classification, identify the nature of previous pregnancy losses, and delineate all possible risk factors.
For a successful pregnancy to occur, even if the maternal genetic, immunological, and anatomical factors are favorable, they must work together with the paternal and embryologic milieu as well. During the autoimmune rejection process of gestation, deregulation of the expressions of proinflammatory cells generates cytotoxicity, which can lead to miscarriages. The most prominent effectors of this pathology are NK cells, whose cytotoxic expressions are controlled by the KIR genes. Genotyping the KIRs, measuring their expression levels, and revealing their relationship with HLA-C appear to be a cornerstone for fetal and placental growth (Beaman et al., 2014; Perce-da-Silva et al., 2015; Comins-Boo et al., 2016; Quan and Yang, 2017).
In this study, we evaluated nine KIR genes thought to be associated with URPL. We found that eight of them were associated with an increased risk of URPL (2DL1, 2DL2, 2DL3, 2DL4, 2DS1, 2DS2, 2DS4, and 2DS5) and belong to the B haplotype, which is an activator haplotype. We did not detect 2DS3 in either case or control groups. We focused on the immune rejection phenomenon, in which KIR molecules thought to play one of the major roles, on maternal NK cells interacting with HLA-C ligands of trophoblast cells.
Our results show that the number of activating KIR genes was statistically higher in patients with unexplained RPL when compared with control subjects. These findings were in agreement with the studies of Wang et al. (2007), Faridi et al. (2009), Vargas et al. (2009), and Ozturk et al. (2012), who found that women with activating KIR genes have a threefold higher probability of developing RPL. It is hypothesized that the number of activating KIR genes per genotype may influence URPL susceptibility through a gene dosage effect, which may tend toward an undesirable autoimmune pathogenesis, possibly caused by an imbalance between activating and inhibitory KIRs. Fifteen (21.42%) of 70 patients have the same genetic makeup of inhibitory KIRs that include 2DL2, 2DL3, and 2DL4.
The Bx genotype occurred at a significantly higher rate in our patient group when compared with controls (85.8%). Thus, it is likely that possessing a Bx genotype promotes the etiopathogenesis of URPL. In contrast to our results, Flores et al. (2007) found that the KIR AA genotype was higher in the study subjects when compared with the controls.
The findings in this study in the evaluation of KIR genotypes in URPL risk may contribute to the interaction of the genes in the inhibitory and activatory KIR repertoire in which gene content varies between haplotypes. However, studies on the absence or presence of KIR genotypes have conflicting results among different populations. To solve this discrepancy, more data and studies are required, which look at interallelic combination of KIRs, diversity at the level of the locus, and their expression patterns (Dambaeva et al., 2016).
Therefore, creating a frequency database of KIR genes for every population will have important effects on determining the disorders, including URPL, with immunological origin. Such data, together with the HLA ligands, which are functionally linked to KIRs, will lead to enormous levels of genetic variation among individuals and between populations with different ethnic groups. The stochastic association of these genes may trigger not only the URPL outcomes but also pre-eclampsia, intrauterine fetal growth restriction, and in vitro fertilization failure (Jamil and Khakoo, 2011; Alecsandru et al., 2014; Chercıu et al., 2016; Sugioka et al., 2016).
In this study we found that both inhibitory and activatory KIR gene polymorphisms were higher in URPL women compared with controls. The highly polymorphic nature of the KIR gene family can explain these results. With 15 genes (www.ebi.ac.uk/ipd/kir) containing 907 alleles and split into 2 haplotypic groups, the degree of variation within the gene family among individuals and ethnic groups is very high, and can explain multiple heterogeneous outcomes and phenotypes. Although all of the KIR genes are localized to chromosome 19q13.4, they are separately expressed, and each has unique interaction motifs (Hiby et al., 2008; Falco et al., 2013). Moreover, the degree of recombination in this region is high; Europeans alone have dozens of gene-content haplotypes. This genomic region is rich in transposons, which likely provide the primary mechanism for recurrent meiotic recombination event. Therefore, more detailed gene analysis techniques (receptor expression, gene and genotype distribution, and the relationship with KIR ligands such as HLA-C) would help with the understanding of KIR-related URPL (Roe et al., 2017).
Finally it is important to consider not only the role of the KIR gene family by itself in the regulation of NK cells but also their interactions with the HLA proteins as it is likely the complex interplay of both activating and inhibitory KIR proteins with their cognate HLA counterparts that predicts/determines URPL.
Footnotes
Acknowledgments
The authors of this article thank the patient and control group women for their participation in the study. They also thank Prof. Dr. İ.Ömer Barlas and the Mersin University Department of Gynecology and Obstetrics for their valuable contributions and collaboration.
Author Disclosure Statement
No competing financial interests exist.