
Abstract
Objective:
Perindopril is an angiotensin-converting enzyme (ACE) inhibitor that is commonly used in the treatment of Chinese Han patients with acute myocardial infarction (AMI). However, there have been few studies on whether polymorphisms of the ACE gene affect the efficacy of perindopril or the prognosis of AMI patients. The purpose of this study was to analyze the relationship among the ACE rs121912703 (C>T), rs767880620 (C>A), and rs397514689 (C>T) gene polymorphisms and the prognosis of AMI patients and the clinical efficacy of perindopril in the treatment of AMI.
Methods:
The ACE genotypes at the rs121912703, rs767880620, and rs397514689 loci in 225 AMI patients treated with perindopril were determined by polymerase chain reaction/Sanger sequencing. Differences in cardiac structure, functional indicators, hemodynamic parameters, and related laboratory indicators were detected before and after treatment.
Results:
After administration of perindopril, improved ventricular remodeling in AMI patients with wild-type ACE was better than in patients with the ACE rs121912703, rs767880620, and rs397514689 minor variant alleles. The patients harboring wild-type ACE had lower systolic blood pressure and diastolic blood pressure than the patients harboring the minor variant alleles (p < 0.01). The contents of serum ACE and Ang II (angiotensin II) in AMI patients carrying the wild-type ACE alleles were lower than those of patients harboring any of the minor variant alleles (p < 0.01). The 3-year survival time of AMI patients carrying the wild-type ACE alleles was markedly greater compared with AMI patients carrying the mutant genes (p < 0.01).
Conclusion:
Mutations at the ACE rs121912703, rs767880620, and rs397514689 loci affect the efficacy of perindopril on ventricular remodeling and hemodynamics in Chinese Han AMI patients. The 3-year survival of AMI patients harboring the variant alleles is less than that of the patients harboring the wild-type gene.
Introduction
Acute myocardial infarction (AMI) is myocardial cell ischemia and hypoxia necrosis caused by interruption of blood supply to the coronary arteries. Its clinical features are acute circulatory dysfunction, heart failure, chest pain, and arrhythmia (Culic et al., 2003; Van de Werf et al., 2009; Steg et al., 2012). In recent years, with the development of medical technology, an increasing number of AMI patients have shown increased survival rates after revascularization (Dzavik et al., 2003; Kalarus et al., 2007). After revascularization in patients with AMI, ventricular remodeling leads to enlargement of the ventricles, decreased cardiac function, and poor prognosis.
Angiotensin-converting enzyme inhibitor (ACEI) can effectively improve ventricular remodeling in AMI patients during convalescence. Clinically, it is suggested that ACEI drugs should be used in AMI patients after vascular remodeling, but this is not applicable to patients with contraindications (Mathews et al., 2015). Perindopril is a third-generation ACEI drug.
The renin-angiotensin-aldosterone system (RAAS) plays a crucial role in blood pressure regulation and water and salt metabolism. Angiotensin-converting enzyme (ACE) is one of the key enzymes of the RAAS, and its main physiological function in vivo is to convert angiotensin I (Ang I) into the effector peptide angiotensin II (Ang II) (Liu et al., 2002). The main role of ACEI drugs is to inhibit the conversion of Ang I into Ang II by inhibiting ACE (McMurray et al., 2014; Lee et al., 2016). The expression of ACE is controlled by the ACE gene. We speculated that single nucleotide polymorphisms (SNPs) of the ACE gene might influence the efficacy of ACEI drugs. To evaluate this hypothesis, we selected several pathogenic and possibly damaging SNP loci using the Ensembl system rs121912703, rs767880620, and rs397514689. AMI patients were followed up for 3 years to study the effect of these SNPs on the prognostic survival of AMI patients treated with perindopril.
Patient Selection and Clinical Evaluation and Methods
Patient selection and clinical evaluation
From January 2013 to February 2015, 225 AMI patients (aged from 42 to 81 years, with an average age of [57.5 ± 7.9] years, BMI [25.7 ± 1.6] kg/m2, 123 males [58.0%], and 89 females [42.0%]) admitted to Yuhuangding Hospital Affiliated with Qingdao University were selected as research subjects. Thirty-nine patients had smoked at least 100 cigarettes in the past (at least 5 packs, 20 cigarettes per pack), and 52 patients drank more than 50 mL per week. The diagnostic criteria for AMI were based on the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Ryan et al., 1996). All patients involved in the study signed informed consent, and the study was approved by the Medical Ethics Committee of Yuhuangding Hospital Affiliated with Qingdao University. Inclusion criteria were as follows: compliance with diagnostic criteria of AMI in this study; admission within 6 h after onset; and successful establishment of recanalization within 12 h after admission. Exclusion criteria were as follows: admission after morbidity 6 h; Killip classification ≥III at admission; severe liver and kidney dysfunction; perindopril allergy history; and arrhythmia.
Methods
After admission, all patients were monitored for heart rate (HR), blood pressure, respiration, and blood oxygen. Meanwhile, symptomatic treatment such as analgesia, dilation of coronary arteries, antiplatelet, and anticoagulation was performed during emergency percutaneous coronary intervention. Perindopril (commodity name: Yastar; Servier Pharmaceutical Co., Ltd., Tianjin; specification 4 mg) was administered to all patients when vascular recanalization (thrombolysis in myocardial infarction flow grade is up to 2∼3) and blood pressure were stable. The initial dosage was 2 mg/qd, which was increased by 2 mg/qd every 1-2 weeks depending on the patient's condition. The course of treatment was 6 months. At the same time, all patients underwent routine secondary prevention after surgery, including aspirin plus clopidogrel dual antiplatelet therapy, β-receptor blockers to prevent arrhythmia, statins to regulate blood lipids, and to control diet and exercise.
Outcome measures
(1) Differences in the cardiac structure and function of all AMI patients were observed before and 6 months after treatment, and color Doppler ultrasonic electrocardiography (The ACUSON S2000 full digital Doppler ultrasound diagnostic system of Siemens Co., Ltd., China) was performed in the patients with stable hemodynamics. The recorded indicators included left ventricular end systolic diameter (LVESD), left ventricular end diastolic diameter (LVEDD), interventricular septum diameter (IVSD), left ventricular posterior wall diameter (LVPWD), IVSD, left ventricular ejection fraction (LVEF), and cardiac output (CO). (2) An HBP-1300 electronic sphygmomanometer was used to measure the hemodynamic parameters of all AMI patients, including systolic blood pressure (SBP), diastolic blood pressure (DBP), and HR. (3) Fasting venous blood (5 mL) was collected from each AMI patient, 2 mL of which was anticoagulated with EDTA for genomic DNA extraction, and the other 3 mL was used to detect fasting blood glucose (FPG), total cholesterol (TC), triacylglycerol (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), alanine transaminase (ALT), serum creatinine (Scr), aspartate aminotransferase (AST), and blood and urea nitrogen (BUN) using a 7020 fully automatic biochemical analyzer. (4) Adverse reactions of the patients were recorded. (5) All patients were followed up for 3 years by telephone or home visit.
Genotyping
Genomic DNA was extracted from the blood of patients using a QIAamp DNA Blood Mini Kit (Qiagen 51104, German). Polymerase chain reaction (PCR) amplification primers were designed basing on the ACE sequence in the NCBI Single Nucleotide Database (https://www.ncbi.nlm.nih.gov/snp). The primer sets used were as follows: rs121912703 Fw: 5′-CAG TAC AAC TGG ACG CCG A-3′ and Rv: 5′-GAG GGG GTT AAG ACC CAA GGC-3′; rs767880620 Fw: 5′-TCA CCC TGT TCC TGC ATA GA-3′ and Rv: 5′-GTT GGT CGT GGG TGA GAC C-3′; and rs397514689 Fw: 5′-TCA CCC TGT TCC TGC ATA GA-3′ and Rv: 5′-GTT GGT CGT GGG TGA GAC C-3′. Operate in strict accordance with the kit instructions. A PCR Amplification Kit (Cat# SK2491-50; Biotech Engineering Co., Ltd., Shanghai) was used to perform PCR amplification of the ACE rs121912703, rs767880620, and rs397514689 loci from genomic DNA. The PCR amplification products were purified using a DNA Purification Kit (Cat# D0033; Beyotime, China), and the DNA sequence of the target fragment was determined using Sanger sequencing. The genotype frequencies of different groups of ACE rs121912703, rs767880620, and rs397514689 loci are shown in Table 1.
The Genotype Frequencies of Different Groups of Angiotensin-Converting Enzyme rs121912703, rs767880620, and rs397514689 Loci
Those people who had smoked at least 100 cigarettes in the past (at least 5 packs, 20 cigarettes per pack).
Weekly alcohol consumption more than 50 mL.
BMI, body mass index.
Statistical analysis
Statistical analysis of the data was performed using SPSS20.0, and the survival curves of progression-free survival and overall survival were determined using the Kaplan-Meier method and Log-rank test. The t-test was used for comparative analysis of clinical indicators of AMI patients harboring mutant and wild-type genes. p < 0.05 indicates that the difference was statistically significant.
Results
Baseline data
The baseline data of 225 AMI patients selected in this study are shown in Table 2.
Baseline Data of Acute Myocardial Infarction Patients
Differences in heart structure, function, and hemodynamic parameters before and after treatment
LVESD, LVEDD, LVPWD, CO, HR, SBP, DBP, FPG, TC, TG, and LDL-C in AMI patients were distinctly lower after treatment than before treatment (<0.01). LVEF, CO, SBP, DBP, ALT, Scr, AST, and BUN increased markedly after treatment (p < 0.01). There was no difference in IVSD and HDL-C before and after treatment (p > 0.05) (Table 3).
Changes in Cardiac Structure, Function, Hemodynamics, and Related Laboratory Indicators Before and After Treatment (n = 225, ±s)
ALT, alanine transaminase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; CO, cardiac output; DBP, diastolic blood pressure; FPG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; HR, heart rate; IVSD, interventricular septum diameter; LDL-C, low-density lipoprotein cholesterol; LVEDD, left ventricular end diastolic diameter; LVEF, left ventricular ejection fraction; LVESD, left ventricular end systolic diameter; LVPWD, left ventricular posterior wall diameter; SBP, systolic blood pressure; Scr, serum creatinine; TC, total cholesterol; TG, triacylglycerol.
Effects of SNPs of ACE on cardiac structure and function
The effects of ACE gene rs121912703, rs767880620, and rs397514689 SNPs on cardiac structure and function are shown in Tables 4-6. The results of independent sample t-tests showed that after treatment, the LVESD, LVEDD, IVSD, LVPWD, FPG, TC, TG, and LDL-C of AMI patients with wild-type ACE and mutations in ACE at the rs121912703, rs767880620, and rs397514689 loci markedly decreased, and LVEF, CO, ALT, Scr, AST, and BUN increased (p < 0.01). Among AMI patients with different genotypes, before and after treatment with perindopril, LVESD, LVEDD, IVSD, LVPWD, FPG, TC, TG, and LDL-C were lower in AMI patients with wild-type ACE than in those with mutant ACE genes, and ALT, Scr, LVEF, CO, AST, and BUN of patients harboring wild-type ACE were higher than those of patients harboring mutant genes (p < 0.01). There was no significant difference in IVSD and HDL-C between AMI patients with wild-type and mutant genes (p > 0.05).
The Influence of Single Nucleotide Polymorphism of Angiotensin-Converting Enzyme rs121912703 on Cardiac Structure and Function and Other Related Indicators (±s)
The Influence of the Angiotensin-Converting Enzyme rs767880620 Single Nucleotide Polymorphism on Cardiac Structure and Function and Other Related Indicators (±s)
The Influence of the Angiotensin-Converting Enzyme rs397514689 Single Nucleotide Polymorphism on Cardiac Structure and Function and Other Related Indicators (±s)
The influence of ACE SNPs on HR and blood pressure
The genotype frequencies of ACE gene rs121912703, rs767880620, and rs397514689 were in accordance with Hardy-Weinberg equilibrium (p > 0.05). The effect of ACE rs121912703, rs767880620, and rs397514689 SNPs on HR and blood pressure is shown in Figure 1. Before perindopril administration, the HR of AMI patients with wild-type ACE was lower compared with AMI patients with ACE rs121912703, rs767880620, and rs397514689 mutations, and the SBP and DBP in the patients harboring the wild-type gene were higher than those in patients harboring the mutant genes (p < 0.01). After perindopril administration, the HR, SBP, and DBP of all patients with AMI decreased (p < 0.01). After perindopril administration, the SBP and DBP of AMI patients with wild-type ACE were lower compared with the patients with ACE mutations at the rs121912703, rs767880620, and rs397514689 loci (p < 0.05).
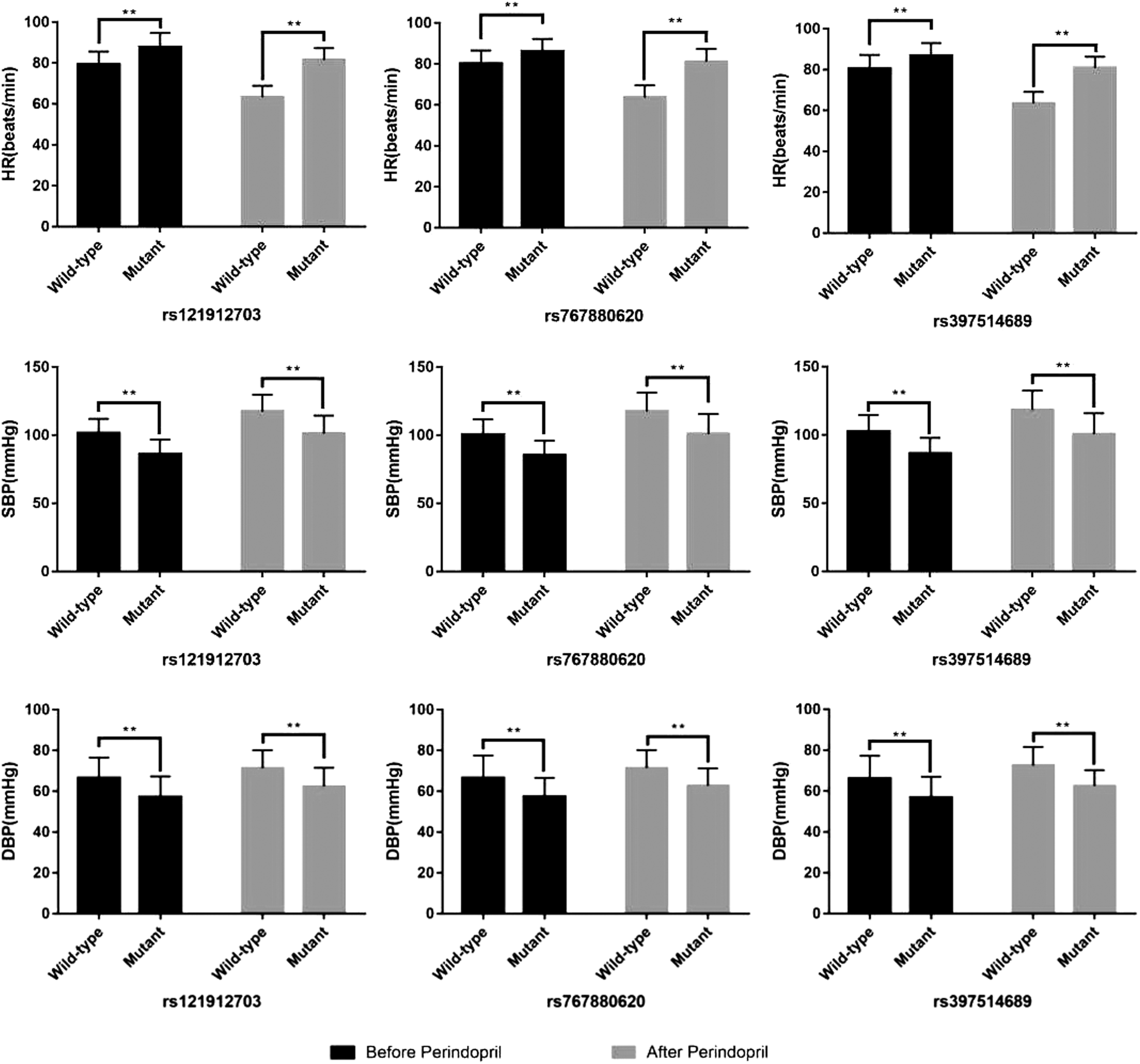
The association of the ACE gene rs121912703, rs767880620, and rs397514689 SNPs with HR and blood pressure. **p < 0.01. ACE, angiotensin-converting enzyme; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SNPs, single nucleotide polymorphisms.
The influence of ACE SNPs on the expression of serum ACE and Ang II
The association of ACE gene rs121912703, rs767880620, and rs397514689 SNPs with serum ACE and Ang II expression levels is shown in Figure 2. Before perindopril administration, the levels of serum ACE and Ang II in AMI patients with wild-type ACE were distinctly lower than those in AMI patients with mutations at the rs121912703, rs767880620, and rs397514689 loci (p < 0.01). After treatment with perindopril, the levels of ACE and Ang II were distinctly lower than the levels before treatment in AMI patients with wild-type ACE and in patients with ACE gene rs121912703, rs767880620, and rs397514689 mutations, and the contents of serum ACE and Ang II in AMI patients with wild-type ACE were distinctly lower than those in patients with mutant genes (p < 0.01).
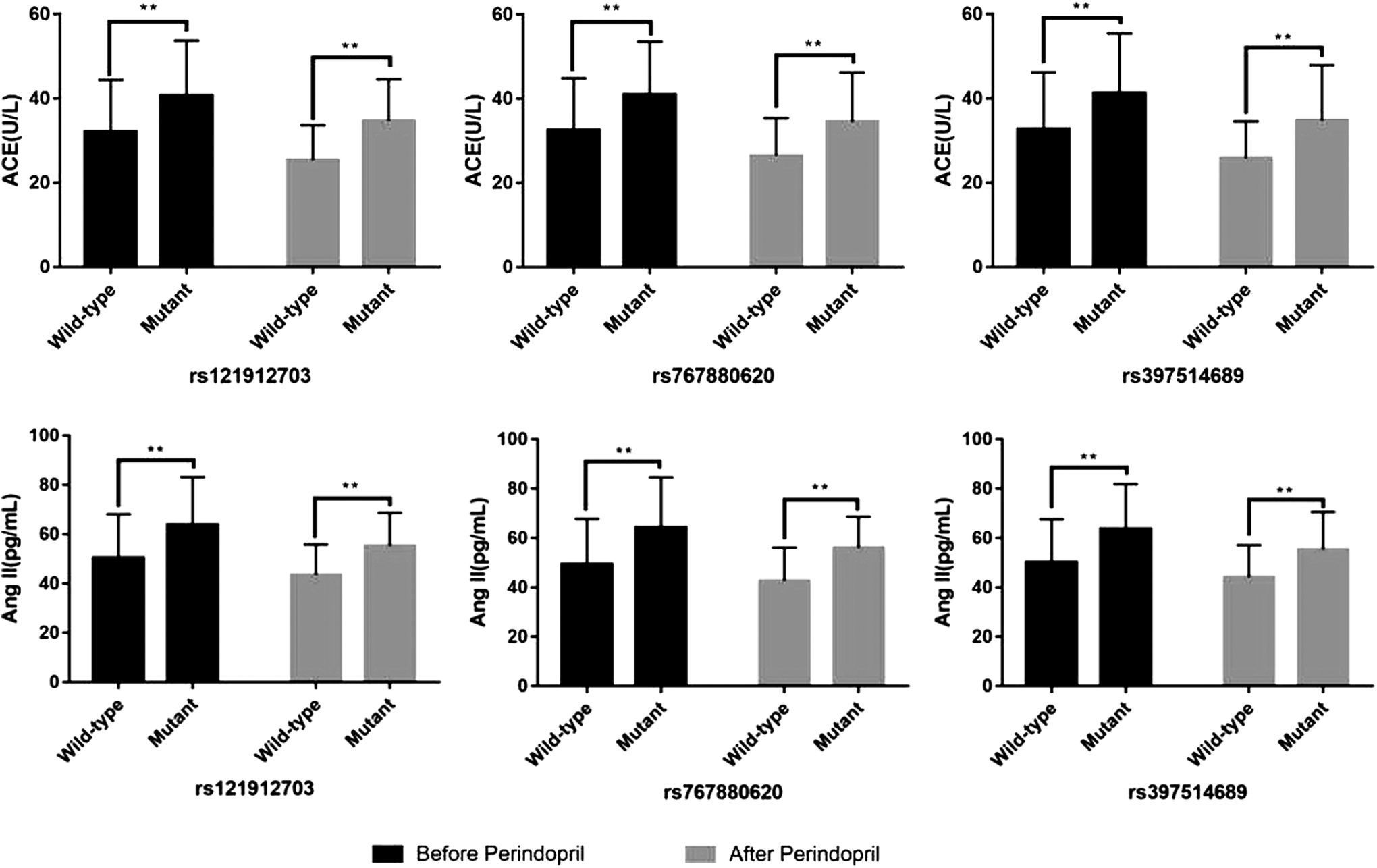
The influence of ACE SNPs on the expression of serum ACE and Ang II. **p < 0.01. Ang II, angiotensin II.
Adverse reaction
Seven cases of renal dysfunction and 14 cases of gastrointestinal adverse reactions occurred in this study, and the incidence of adverse reactions was 9.33%.
The effect of ACE SNPs on the prognosis of AMI patients after perindopril administration
The correlation among ACE rs121912703, rs767880620, and rs397514689 SNPs and the prognosis of AMI patients after perindopril administration is shown in Figure 3. After 3 years of follow-up, the association between ACE gene polymorphisms and survival of AMI patients was analyzed, and multivariate logistic regression was used to correct factors such as age, gender, smoking, drinking, body mass index (BMI), and Killip classification. The results showed that the 3-year survival of AMI patients with wild-type ACE was distinctly longer compared with AMI patients with mutations at rs121912703, rs767880620, and rs397514689 (p < 0.01).
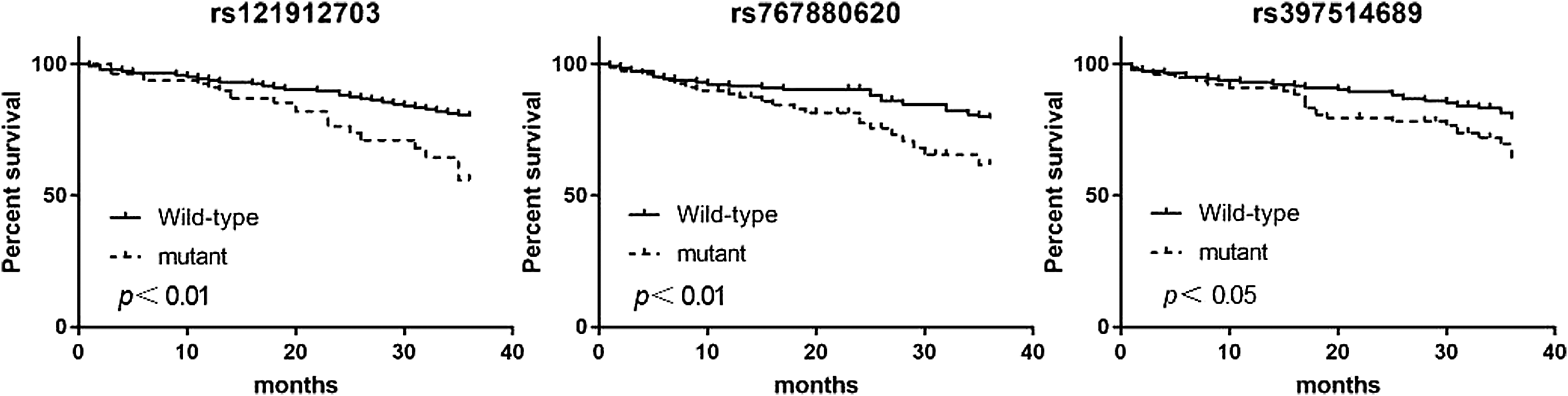
The influence of ACE SNPs on the prognosis of AMI patients. AMI, acute myocardial infarction.
Discussion
Studies have shown that the activation of the RAAS plays an important role in the process of ventricular remodeling in the pathogenesis of AMI (Huang and Leenen, 2009; Bahramali et al., 2017). ACEI drugs or Ang II receptor antagonists can effectively block the effects of angiotensin, reduce vascular resistance in AMI patients, inhibit the secretion of aldosterone, and improve the function of ventricular diastole in patients, thus preventing ventricular remodeling (Geshi et al., 2001).
Perindopril as a third-generation ACEI drug can significantly improve ventricular remodeling in patients with AMI. Double blind, placebo-controlled, multicenter clinical trials demonstrate that perindopril can reduce cardiovascular morbidity and mortality in patients with stable coronary heart disease (Brugts et al., 2009). The results of this study showed that after treatment LVESD, LVEDD, and LVPWD were significantly lower in patients with AMI, indicating that after treatment with perindopril, the heart chamber size was reduced, the ventricular wall was thinner than before treatment, and the LVEF and CO were significantly increased, indicating that perindopril effectively inhibited ventricular remodeling in patients with AMI and improved ventricular function, which are consistent with the results of Zhang et al. (2018). ACEI mainly acts through Ang II and bradykinin to improve myocardial remodeling. On the one hand, ACEI acts on the RASS system to convert the Ang I to Ang II and reduce the level of Ang II in vivo; on the other hand, ACEI acts on kininase II to inhibit the degradation of bradykinin through the bradykinin-prostaglandin-nitric oxide pathway (Volpe et al., 2016). The hemodynamic parameters of AMI patients after treatment showed that SBP and DBP decreased distinctively after treatment, which was consistent with the results of Thomson and Greenacre (2007). In a study of hypertensive patients, it was found that when perindopril was used alone, the blood pressure of the patient was well controlled regardless of their size.
The expression of ACE, the target of perindopril, is regulated by ACE genes. Genetic factors play an important role in the treatment of ACEI. The understanding of the gene spectrum of the benefits of ACEI treatment can optimize treatment methods and improve patient outcomes (Brugts et al., 2010). Whether ACE polymorphisms affect the interaction between perindopril and ACE is one of the hot topics in clinical research. The genetic study of cardiovascular pharmacogenetics of ACEI drugs in patients with coronary heart disease is still in its infancy. The genetic characteristics of the benefits associated with the treatment of perindopril were evaluated according to the genetic determinants of treatment benefit and blood pressure response (Brugts et al., 2012). Ajala et al. (2012) showed that an indel in the Alu sequence in the 16th intron of the ACE gene affects the content of Ang II in the blood, resulting in unstable clinical efficacy of perindopril. Iqbal et al. (2004) showed that in exon of Chromosome 17, a G2350A gene polymorphism has a distinct effect on plasma ACE concentrations. To study the effect of ACE gene polymorphisms on perindopril treatment, we selected three SNPs in the ACE gene: rs121912703, rs767880620, and rs397514689. Rs121912703 is located on chromosome 17, rs121912703 and rs397514689 are predicted to be pathogenic on the Ensembl system, and the probability that rs767880620 is damaging was predicted by the system to be 0.983. Since all three SNPs belong to the variation of protein coding sequence, there is no evidence to support how to reflect the 3D structure of the protein and whether it affects the interaction with other molecules. We inferred that these three SNPs site polymorphisms in the amino acid sequence of ACE protein and further affect the structure of ACE protein. To verify the inference, this study analyzed the correlation between the efficacy of ACEI drugs and the polymorphisms of these three SNP loci in the treatment of AMI.
The results showed that the improvement of ventricular remodeling of AMI patients with wild-type ACE after treatment with perindopril was distinctly better compared with patients with mutations at rs121912703, rs767880620, and rs397514689 when treated at the same dose. Comparison of hemodynamic parameters showed that after treatment with perindopril, the SBP and DBP of AMI patients with wild-type ACE were lower compared with patients harboring mutant genes (p < 0.05), while there is no significant change in HR of patients harboring mutant genes (p > 0.05), indicating that perindopril has no obvious effect on HR in patients, and the decrease of HR after treatment is mainly due to the effect of β-blockers. Although the SNP and DBP of the mutant patients were reduced after treatment, the SBP and DBP were still at abnormally high levels compared with the wild-type patients, indicating that the abnormally high level of ACE after ACE mutation requires more doses of perindopril to achieve the same clinical effect. We also found that the contents of serum ACE and Ang II in AMI patients with wild-type ACE were distinctly lower than those in patients harboring mutant genes (p < 0.05). We speculated that the ACE SNPs at rs121912703, rs767880620, and rs397514689 may have affected the expression of ACE. Higher expression of ACE in the patients harboring mutant genes resulted in a higher conversion of Ang I to Ang II, eventually leading to a decrease in heart function and heart failure. This stimulated the proliferation of myocardium and vascular smooth muscle cells, which promoted retention, oxidation, and engulfment of LDL by macrophages, thereby promoting the development of atherosclerosis (Schulman et al., 2006; Shafi, 2013).
In addition, this study also analyzed the impact of ACE gene polymorphisms on the prognosis of AMI patients administered perindopril. After 3 years of follow-up, the 3-year survival of AMI patients with wild-type ACE was distinctly longer compared with AMI patients with ACE mutations at rs121912703, rs767880620, and rs397514689 (p < 0.01). From this result, it can be seen that the ACE SNPs affected the survival of patients with AMI treated with perindopril. The specific manifestation is that the sensitivity of AMI patients harboring mutant genes to perindopril is not as high as that of patients harboring the wild-type gene, and patients with these mutations may require larger doses of perindopril. It is necessary to evaluate ACE SNPs at rs121912703, rs767880620, and rs397514689 in AMI patients before treatment with perindopril. According to the test results, we can better guide clinical medication. Patients with AMI who harbor ACE mutations may need more or higher doses of perindopril for treatment. In addition, the incidence of adverse reactions in this study was only 9.33%, and there was no notable correlation between ACE gene polymorphisms and adverse effects of perindopril.
This study also has some weaknesses. First, the selection of the ACE gene polymorphism sites was based on predicted results from the Ensembl database, but there is no relevant research to confirm that these SNPs have functional effects. However, as an exploratory study, this can be understood and accepted. In addition, the sample size was also relatively small. To reduce the influence of the error on the analysis results of the related indicators, it is necessary to increase the sample size of this research. Finally, we need to further study the effects of SNPs at these three loci of the ACE gene on perindopril dose to support our conclusions.
Conclusion
Patients with ACE rs121912703, rs767880620, and rs397514689 mutations showed less improvement of ventricular remodeling and hemodynamics than patients harboring the wild-type gene after treatment with the same dose of perindopril. The 3-year survival of AMI patients harboring the mutant genes was shorter compared with AMI patients harboring wild-type ACE, which may be related to the high expression of ACE and the high content of serum Ang II in the patients harboring the mutant genes.
Footnotes
Acknowledgment
This work was supported by grants from Yuhuangding Hospital Affiliated to Qingdao University.
Data Availability Statement
All data generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors' Contributions
T.D. participated in the study design, data collection, and analysis of data and drafted the article. H.L. participated in data collection and analysis of data. Y.Y.L. carried out the study design and the analysis and interpretation of data and revised the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.