
Abstract
Background and Aims:
The relationship between the promoter polymorphism (−308G/A) of the tumor necrosis factor-alpha (TNF-α) gene and the susceptibility to asthma has been tested in several studies. However, the results have been inconsistent. Therefore, we performed an updated meta-analysis to evaluate the relationship between this promoter polymorphism of the TNF-α gene and the risk of asthma.
Methods:
Fifty case-control studies were included in this meta-analysis which provided 17,937 controls and 9961 asthma patients. The pooled p-value, odds ratio (OR), and 95% confidence interval (95% CI) were used to investigate the strength of the association of this polymorphism of the TNF-α gene with the risk of asthma. The meta-analysis was carried out by Comprehensive Meta-Analysis software.
Results:
The results of our meta-analysis revealed that the TNF-α polymorphism (−308, G/A) was strongly associated with the risk of asthma (p < 0.05 in the allelic, dominant, and recessive models, respectively). In further analyses, based on age group and ethnicity, we observed this association for all subpopulations examined (p < 0.05 in allelic, dominant, and recessive models, respectively).
Conclusion:
This large-scale meta-analysis supports a strong association between the TNF-α gene promoter polymorphism (−308G/A) and the development to asthma in both children and adults.
Introduction
Asthma is a common chronic lower respiratory disease. It is characterized by chronic airway inflammation associated with variable airflow obstruction and airway hyperresponsiveness. Previous studies revealed that tumor necrosis factor-α (TNF-α) is implicated in pathogenesis of asthma. TNF-α gene encodes a multifunctional proinflammatory cytokine that is versatile and very popular (Kim et al., 2017a). TNF was derived from the ability to control endotoxin-induced tumor necrosis gene (Carswell et al., 1975). It is mainly produced in macrophage cell but it is also widely expressed in granulocytes, fibroblasts, epithelial cells, and so on (Spriggs et al., 1992; Li et al., 2018). It is also involved in inflammation, even “master regulator” of proinflammatory cytokine production (Maini et al., 1995; Michlewska et al., 2009), regulation of apoptosis in macrophage (Takada et al., 2007), differentiation (Witsell and Schook, 1992), and so on. Like this, TNF has a variety of functions so that it is associated with various diseases related to these functions. As TNF-α mediates survival of macrophage, it plays an important role in sepsis (Conte et al., 2006). A macrophage-derived TNF-α downregulates macrophage scavenger receptor gene expression and is related to the development of atherosclerosis (Hsu et al., 1996). Because TNF-α is associated with and involved in a variety of pathways, mutations in the gene are also associated with the development of various diseases. TNF-α polymorphism is associated with dengue (Santos et al., 2017), cancer including gastric cancer and hepatocellular cancer (Wang et al., 2016a), systemic lupus erythematosus (Yang et al., 2017), immune thrombocytopenia (Zhang et al., 2017), ischemic stroke (Song and Cheng, 2017), and others. Thus, it is natural that there are many studies on this.
Asthma cannot escape the touch of TNF-α. Asthma is a complex disease and has diverse causes. Not only environmental factors such as indoor allergen (Ahluwalia and Matsui, 2011), socioeconomic and ethnic disparities (Gold and Wright, 2005), and drug use including acetaminophen (Henderson and Shaheen, 2013) or antibiotics (Murk et al., 2011a) but also genetic factors such as promoter polymorphisms in the chromosome 5 gene cluster (Rosenwasser et al., 1995), polymorphism of ADAM33 (Van Eerdewegh et al., 2002), KCNS3 (Hao et al., 2005), HNMT gene (Preuss et al., 1998), and so on could be the cause of asthma. Some genetic variants could cause asthma when they interact with other environmental factors, gene polymorphisms, or specific diseases (Martinez, 2007). Among them, quantitative locus analysis of airway hyperresponsiveness in mice revealed that one of the locus contained TNF-α (De Sanctis et al., 1995). In addition, there have been many studies on the polymorphism of TNF-α and the occurrence of asthma. TNF-α polymorphism has been reported to be a genetic risk factor for the development of asthma in the UK/Irish child (Winchester et al., 2000).
The aim of this study is to evaluate the relationship between promoter polymorphism (−308G/A) of TNF-α gene and the development of asthma in updated meta-analysis.
Materials and Methods
Search strategy
We performed a comprehensive electronic search including PUBMED, EMBASE, scholar of google, and Korean databases was performed until April 1, 2016 to search eligible studies. We used the following keywords to find eligible studies: “tumor necrosis factor,” “TNF-alpha”, or “TNF-A,” AND “polymorphism,” “polymorphisms,” or “variant” AND “rs1800629,” or”−308” AND “acute rejection,” “asthma,” or “meta analysis.” The previous meta-analysis studies about TNF-α (−308G/A) and asthma were considered as reference. Additional studies were identified by a hand search of the references of original studies.
Study selection
Published articles were recruited in our updated meta-analysis if they met the inclusion criteria: (i) evaluation of the association between the TNF-α polymorphism (−308G/A) and asthma; (ii) study was designed using the case-control study or cohort studies; (iii) contained sufficient distribution of TNF-α polymorphism (−308G/A) in the asthma group and the control group for the estimation of an odds ratio (OR), 95% confidence interval (CI), and p-value. Studies that deviated from Hardy-Weinberg equilibrium (HWE) in the control group were excluded.
Data extraction
The investigators extracted data and reached consensus on all of the data. We extracted data from the selected articles including the first author's name, year of publication, population of subject, number of cases and controls, and genotype frequency of TNF-α polymorphism (−308G/A).
Statistical analysis
HWE in control subjects was assessed by chi-squared test. The pooled p-value, OR, and 95% CI were used to assess association between susceptibility to asthma and TNF-α polymorphism (−308G/A). And we calculated the heterogeneity among studies. The heterogeneity test was referred for the null hypothesis that all studies evaluated the same effect. The chi-square-based Q test and I2 test were applied. When p-value of the Q test was less than 0.05 or I2 statistic was >50%, we considered significant heterogeneity. If there was significant heterogeneity, the random-effects Mantel-Haenszel method was adopted to evaluate the point estimates and 95% CI. Otherwise, the fixed-effects Mantel-Haenszel method was adopted.
For meta-analysis of TNF-α polymorphism (−308G/A), the pooled ORs, 95% CI, and p-value were calculated using combination of genotype. We first estimated the risk of the A/A genotype and A/G genotype for asthma compared with the G/G genotype as dominant model, respectively, and then evaluated the risk of “A allele versus G allele,” “A/A genotype+A/G genotype versus G/G genotype,” and “A/A genotype versus A/G genotype+G/G genotype” on risk of asthma, assuming dominant and recessive effects of the variant A allele, respectively (Seok et al., 2014; Park and Kim, 2015; Kang et al., 2016, 2017; Kim et al., 2017b). The p < 0.05 was regarded as statistically significant association with asthma. Meta-analysis was performed using the comprehensive meta-analysis software (Biostat, Englewood, NJ).
Results
Table 1 shows the main characteristics of selected studies included in our updated meta-analysis. Briefly, we performed updated meta-analysis with fifty articles (Moffatt and Cookson, 1997; Albuquerque et al., 1998; Chagani et al., 1999; Tan et al., 1999; Louis et al., 2000; Winchester et al., 2000; Hakonarson et al., 2001; Witte et al., 2002; Buckova et al., 2002; El Bahlawan et al., 2003; Gao et al., 2003; Zhifang et al., 2003; Guo and Zhou, 2004; Beghe et al., 2004; Liu et al., 2004; Zhai and Li, 2004; Shin et al., 2004; Sandford et al., 2004; Wang et al., 2004; Bilolikar et al., 2005; Zhao et al., 2005; Gupta et al., 2005; Kim et al., 2006, 2008; Schubert et al., 2006; Sharma et al., 2006; Tolgyesi et al., 2006; Hong et al., 2007; Kamali-Sarvestani et al., 2007; Mak et al., 2007; Kumar et al., 2008; Kurotani et al., 2008; Trajkov et al., 2008; Wang et al., 2009; Mahdaviani et al., 2009; Aytekin et al., 2009; Castro-Giner et al., 2009; Daley et al., 2009; Jimenez-Morales et al., 2009; Michel et al., 2010; Cui and Wang, 2010; Jiffri and Elhawary, 2011; Murk et al., 2011b; Jia et al., 2012; Chiang et al., 2013; Shaker et al., 2013; Ying et al., 2013; Dhaouadia et al., 2011; Despotovic et al., 2015; Yang et al., 2015; Zheng et al. 2012). After pooling all data, these 50 articles included 17,937 asthma patients and 9961 control subjects.
Characteristics of Eligible Studies Included in the Meta-Analysis
Among these 50 studies, any studies did not show an error in the HWE in the control group (p > 0.05, data not shown). To estimate risk evaluation in all asthma cases and control, we tested the heterogeneity in each model, respectively (dominant, recessive, and allele model). The results of the heterogeneity test for meta-analysis are shown in Tables 2 and 3, Figures 1-3. If the result of the Q test was p < 0.05 or the I2 statistic was >50%, the random-effects method was adopted. Otherwise, the fixed-effects method was applied. In allele analysis (A allele vs. G allele) between TNF-α polymorphism (−308G/A) and susceptibility to asthma, the minor A allele showed strong association with asthma (all population, OR = 1.344, 95% CI = 1.207-1.497, p < 0.0001; Asian population, OR = 1.342, 95% CI = 1.099-1.639, p = 0.004; Caucasian population, OR = 1.350, 95% CI = 1.187-1.536, p < 0.0001 in random model, respectively) (Table 2 and Fig. 1). In dominant model (A/A genotype+A/G genotype vs. G/G genotype), A/A genotype+A/G genotype presented association with asthma (all population, OR = 1.407, 95% CI = 1.246-1.590, p < 0.0001; Asian population, OR = 1.351, 95% CI = 1.088-1.677, p = 0.007; Caucasian population, OR = 1.452, 95% CI = 1.242-1.698, p < 0.0001 in random model, respectively) (Table 2 and Fig. 2). In recessive model (A/A genotype vs. A/G genotype+G/G genotype), A/A genotype also showed the association with asthma (all population, OR = 1.420, 95% CI = 1.157-1.743, p = 0.0008; Asian population, OR = 1.596, 95% CI = 1.058-2.408, p = 0.026; Caucasian population, OR = 1.425, 95% CI = 1.109-1.830, p = 0.0006 in fixed model, respectively) (Table 2 and Fig. 3).
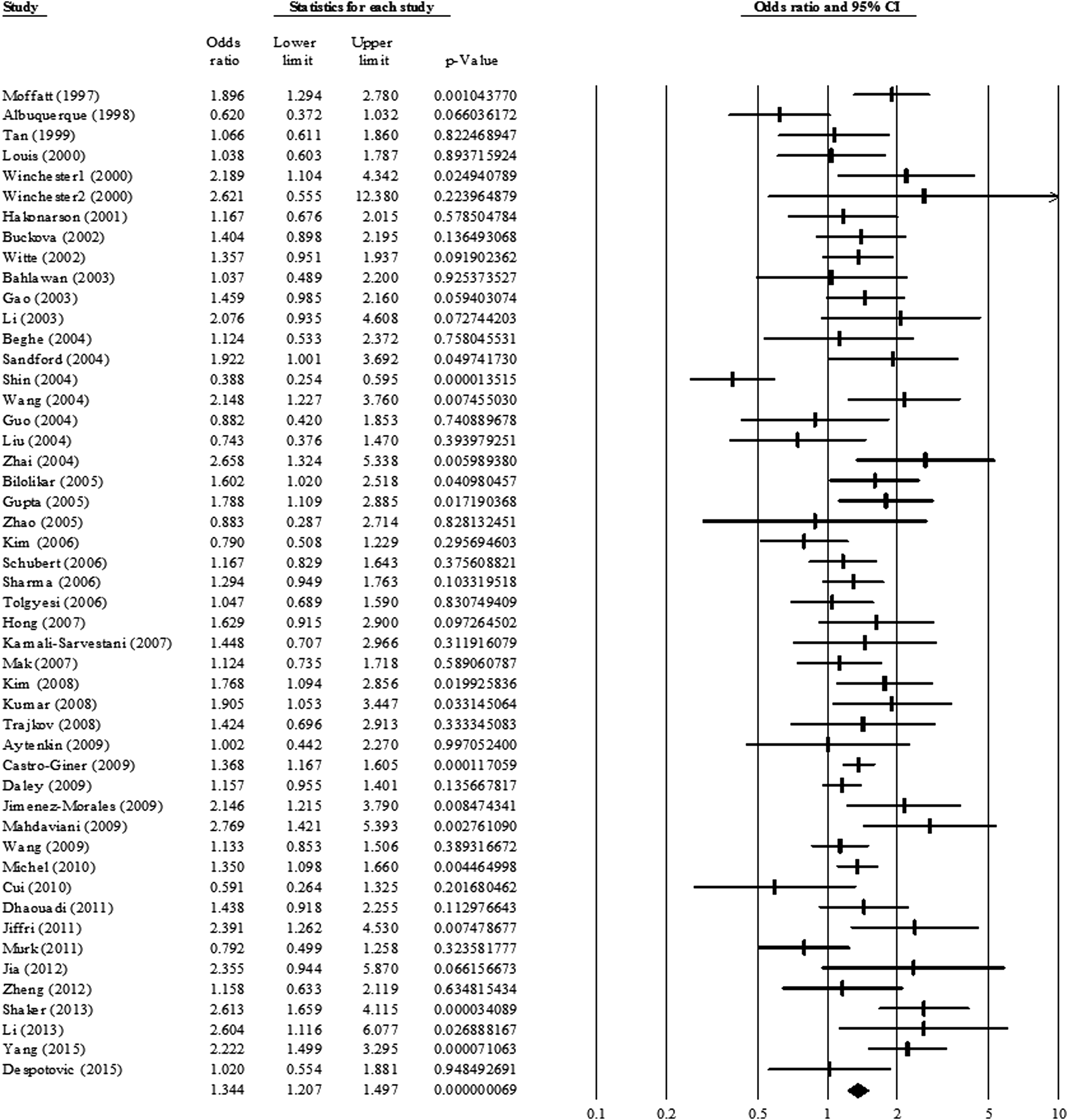
Odds ratio and 95% CI of individual and pooled data for TNF-α polymorphism (−308G/A) and susceptibility to asthma in allele model. CI, confidence interval; TNF-α, tumor necrosis factor-alpha.
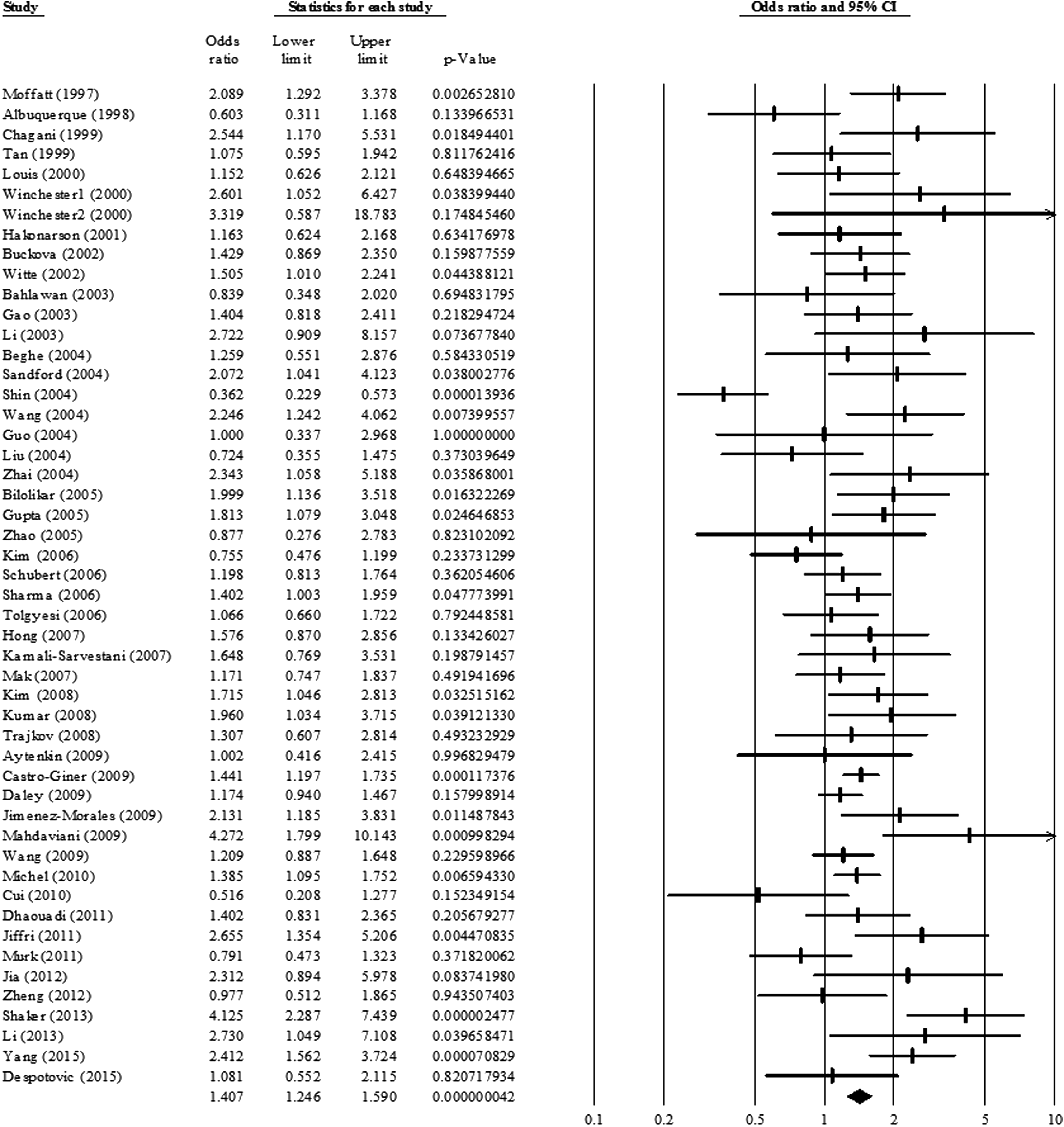
Odds ratio and 95% CI of individual and pooled data for TNF-α polymorphism (−308G/A) and susceptibility to asthma in dominant model.
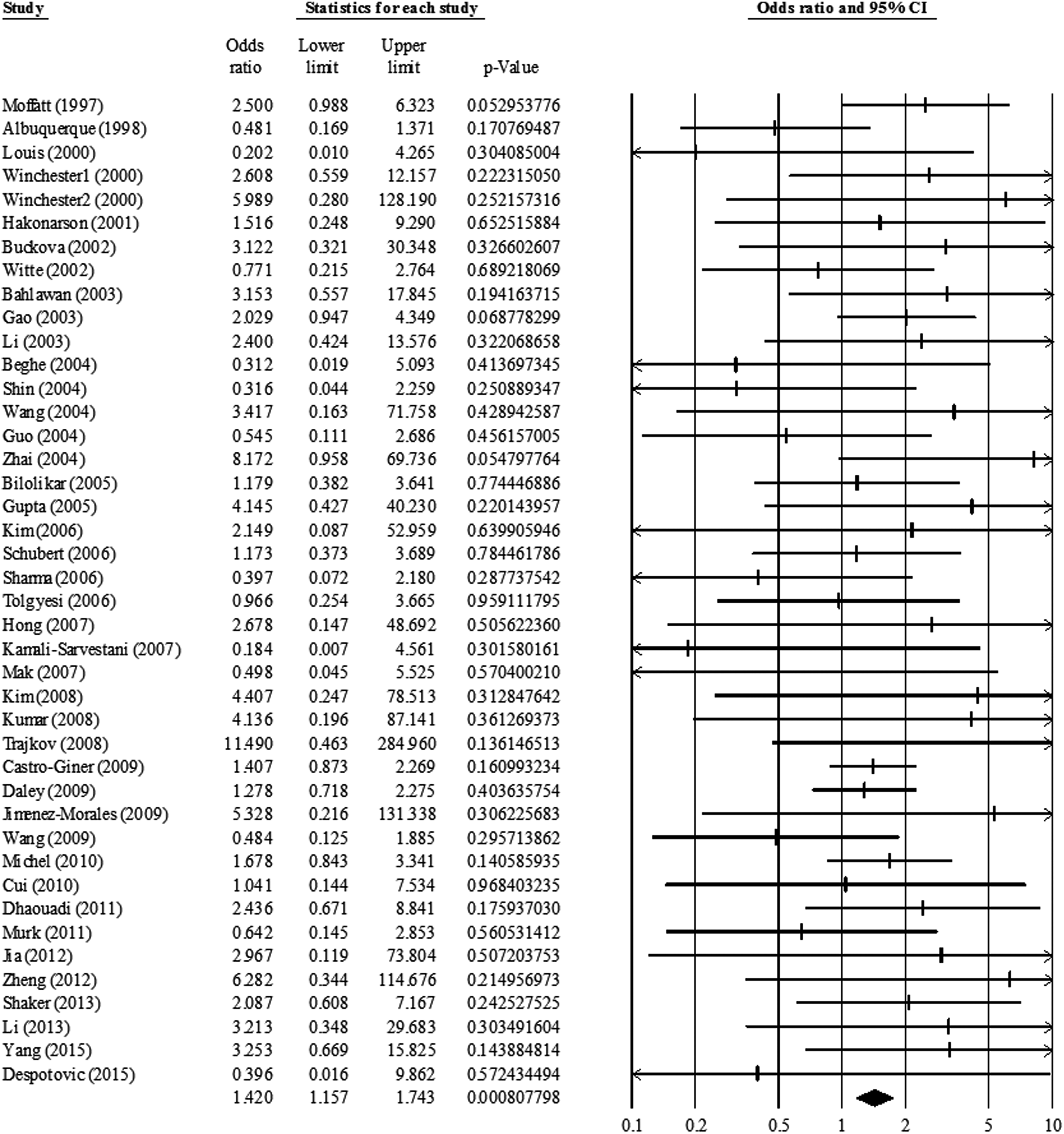
Odds ratio and 95% CI of individual and pooled data for TNF-α polymorphism (−308G/A) and susceptibility to asthma in recessive model.
Overall Analysis Between Tumor Necrosis Factor-Alpha Polymorphism (−308G/A) and Susceptibility to Asthma
Bold numbers are indicants of significant association with risk of asthma.
95% CI, 95% confidence interval; OR, odds ratio.
Overall Analysis Between Tumor Necrosis Factor-Alpha Polymorphism (−308G/A) and Susceptibility to Asthma in Age Group
Bold numbers are indicants of significant association with risk of asthma.
According to age group in asthma, we performed the updated meta-analysis. Table 3 presents the overall analysis with TNF-α polymorphism (−308G/A) and susceptibility to asthma in children/adults. The A allele in allele model significantly increased susceptibility to asthma both in children and adults in Asian and Caucasian population (p < 0.05 in each group) (Table 3). These results obtained from these genetic models suggested that TNF-α polymorphism (−308G/A) was significantly associated with a strong risk of asthma both in children and adults in Asian and Caucasian population.
Discussion
This meta-analysis was carried out to comprehensively interpret the previous studies. Previously there were two meta-analysis articles (Huang et al., 2014; Yang et al., 2014). However, they not only missed several previous existing published articles but also included articles out of the HWE. In addition, three more reports have been published since 2014. Thus, this meta-analysis removed all incorrect articles, added nonincluded articles, and reevaluated overall.
This meta-analysis included a total of 50 articles and showed statistical significance between TNF-α polymorphism and the development of asthma. Table 2 shows a clear relationship between TNF-α polymorphism and the development of asthma in allele and dominant, recessive model, and all races. The symptoms of childhood asthma and adult asthma are similar, and similar treatments are used. But there is a difference between the two. Adult asthma is caused by many causes such as mainly allergies, infection, hormonal factors, and so on and has worse prognosis and poorer response to treatment (de Nijs et al., 2013). Therefore, additional meta-analysis was carried out by dividing each of them. Table 3 shows that allele model was significant in all races in both childhood asthma and adult asthma. In the dominant model, there was no statistical significance in Asian adult asthma. Also, there was no statistical significance in recessive model except for Asian adult asthma. Childhood asthma was not significant in the recessive model. These results may be due to differences of mechanism in childhood asthma and adult asthma.
We found the relationship between asthma and TNF-α polymorphism and confirmed the difference between childhood asthma and adult asthma in this article. Currently, socioeconomic costs associated with asthma are increasing. Asthma has a significant impact on medical resource use and related costs in the Asia-Pacific region (Wang et al., 2016b). Early diagnosis, prevention, and timely and effective treatment of asthma could reduce illness and health care costs and improve quality of life and be clinically and economically beneficial.
In this meta-analysis, a statistically significant relationship between asthma and TNF-α polymorphism was confirmed. However, there is an unsatisfactory point. First of all, there are only Asian and Caucasian ethnic race. There was a lack of research on various other races and could not be examined. And the interaction with other factors also plays an important role in the onset of asthma. Simple one gene could not be an asthma gene and environment elements cannot be ignored. But it is regrettable that environmental factors or other genetic factors could not be considered. If environmental factors are considered and reenforced in more races and more samples, more accurate results will be obtained.
Footnotes
Acknowledgment
This study was supported by a grant from the Traditional Korean Medicine R&D Project, Ministry of Health & Welfare, Republic of Korea (HI15C0171).
Authors' Contributions
J.Y.B confirmed the topic of this article. Y.R.H., D.H., J.C., and J.-H.C. performed the statistical analysis and analyzed the results. S.-J.H. and M.-S. P. contributed to revised article. S.K.K and S.W.K. wrote the article. All authors approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.