
Abstract
Aim:
Celiac disease (CD) is strongly associated with HLA-DQ2.2, HLA-DQ2.5, and HLA-DQ8. Up to 99.7% of all CD patients are positive for either one or two of these genetic markers, demonstrating a high negative predictive value. This has led to the development of diagnostic kits that, instead of providing a full HLA-DQ typing, detect only these three HLA-DQ types. Our aim was to compare three different kits for their performance, utilization, and costs. Because 0.4-3.6% of all CD patients test positive for HLA-DQ7 and negative for the aforementioned types, information provided by the kits regarding DQ7 alpha and beta chains was evaluated as well.
Materials and Methods:
Fifty DNA samples previously typed with the SSCP method were analyzed using three commercial kits.
Results and Discussion:
All kits report hetero- or homozygosity for HLA-DQ2.5. The XeliGen kit directly detects HLA-DQ7, but is relatively expensive. The MLPA kit is the least expensive in terms of reagents and may indirectly detect HLA-DQ7. The CeliaSCAN kit is easy to use and provides indirect information about HLA-DQ7.5.
Conclusion:
All kits correctly identify the CD risk genes. The resources of the laboratory and the intended use should determine the preference for any of the HLA-DQ typing kits herein described.
Introduction
Celiac disease (CD) is strongly associated with HLA-DQ2 and HLA-DQ8. This association was shown to be due to preferential binding of deamidated gliadin peptides by these HLA proteins. HLA-DQ2.5 (encoded by HLA DQA1*05:01 and DQB1*02:01) has the strongest association, with a higher risk for (complicated) disease when homozygous.
Depending on the study size and ethnicity of the study population, 80-97% of the CD patients are HLA-DQ2.5 positive [reviewed in Ref. (Basturk et al., 2017)], compared with ∼35% of the general population. The remaining CD patients are generally either HLA-DQ2.2 (HLA DQA1*02:01, DQB1*02:02) or HLA-DQ8 positive. Most HLA-DQ8-positive CD patients are HLA DQA1*03, DQB1*03:02 positive. However, HLA-DQ8 does also include the less frequently occurring DQB1*03:05 allele. The DQB1*03:10 allele is an HLA-DQ8 allele as well, but is extremely rare in Western Europe and is therefore not discussed here.
Depending on the study, up to 99.7% of the CD patients are positive for either one or two of these three HLA-DQ types, demonstrating a high negative predictive value (Karell et al., 2003; Rostami-Nejad et al., 2014; Tinto et al., 2015; Martinez-Ojinaga et al., 2018). This observation has led to the development of diagnostic kits that, instead of providing a full HLA-DQ typing, detect only HLA-DQ2.2, HLA-DQ2.5, and HLA-DQ8.
Several studies have now indicated that a larger part of the HLA-DQ2.2-, HLA-DQ2.5-, and HLA-DQ8-negative CD patients are HLA-DQ7 positive. The majority of HLA-DQ7-positive individuals are DQA1*05 and DQB1*03:01 (DQ7.5), but the low frequently occurring DQB1*03:04 is also part of HLA-DQ7, and DQB1*03:01 can also pair with other alpha chains such as DQA1*03 and DQA1*02. Frequencies of these HLA-DQ7-positive, other DQ risk haplotype-negative CD patients vary from 0.4% to 3.6% (Karell et al., 2003; Araya et al., 2015; Tinto et al., 2015; Martinez-Ojinaga et al., 2018). DQ9 (defined by DQB1*03:03 paired with DQA1*02:01 or DQA1*03:02) is not associated with CD, although DQ9-restricted gliadin-specific T cells have been described from a DQ2.2/DQ9-positive CD patient (Bodd et al., 2012).
Materials and Methods
Here, three commercial HLA-DQ2.2, HLA-DQ2.5, and HLA-DQ8 typing kits were compared in terms of utilization and costs. Because of the current interest in HLA-DQ7, some HLA-DQ7-positive samples were included as well. Fifty samples, previously typed with the SSCP method (Hadithi et al., 2007), were selected. These included 13 at-risk patients for each CD-associated DQ type, 3 homozygous and 10 heterozygous, including DQ2 (DQ2.2 or DQ2.5) combined with DQ8, and 10 samples negative for DQ2.2, DQ2.5, and DQ8 but positive for DQ7, including 2 homozygous DQ7 samples.
The commercial kits used were the “Celiac Disease, HLA-DQ2.5, HLA-DQ8, HLA-DQ2.2 MLPA kit” (MRC Holland, Amsterdam, The Netherlands) (Vijzelaar et al., 2016), “CeliaSCAN” kit (TubaScan, Amsterdam, The Netherlands) and “XeliGen” kit (Eurospital, Trieste, Italy) (D'Ippolito et al., 2016). The MLPA kit is based on multiplex ligation-dependent probe amplification and analysis with capillary electrophoresis, CeliaSCAN is based on a multiplex real-time polymerase chain reaction (RT-PCR) melting curve analysis, and XeliGen is based on RT-PCR. All tests were performed according to the manufacturer's instructions.
Results and Discussion
Utilization and costs
Table 1 shows the characteristics of the three kits regarding the amount of DNA needed, ability to detect zygosity, execution (extra), reagent costs, and equipment needed.
HLA-DQ Typing Kit Characteristics
Based on positivity for DQB1*03 and negativity for DQB1*03:02, 03:03, and 03:05.
HLA-DQ7.5 can be predicted based on the presence of HLA-DQA1*05 and absence of HLA-DQB1*02.
Based on eight samples per run.
Based on list prices in 2018.
PCR, polymerase chain reaction; RT, reverse transcriptase.
As the XeliGen uses 16 reactions per sample, a relatively high amount of DNA is necessary, and for the MLPA kit, the lowest amount of DNA is needed. The alpha chains for DQ2.5, DQ2.2, DQ8, and DQ7.5 (DQA1*05, DQA1*03, and DQA1*02) as well as the beta chains for DQ2.5/DQ2.2 and DQ8 (DQB1*02 and DQB1*03:02) are directly reported by all kits.
Hetero- or homozygosity for HLA-DQ2.5 is reported by all kits as well. The MLPA and XeliGen kits also report heterozygosity or homozygosity for HLA-DQ8 and DQ2.2, including homozygosity of the DQB1*02 chain only. There are few studies available on the increased risk for HLA-DQ2.2 and HLA-DQ8 homozygous individuals, but a recent study suggests that HLA-DQ8 homozygosity may indicate an increased risk for CD, however, this needs confirmation in larger studies (Martinez-Ojinaga et al. 2018).
Only the XeliGen kit directly reports HLA-DQ7 (DQB1*03:01 and DQB1*03:04 in combination with the most common DQ7 alpha chains DQA1*02, DQA1*03, or DQA1*05) and DQ9. The MLPA kit includes probes for DQB1*03, DQB1*03:02, 03:05, and 03:03. Based on certain combinations of positive and negative probes, DQ7 and DQ9 may be resolved, although positivity for low-frequent DQB1*03 alleles cannot be excluded at this time and DQ9-positive samples were not included in this study. Although the CeliaSCAN kit does not provide information regarding the beta chain of DQ7, the most common DQ7.5 haplotype can be predicted with high probability when DQA1*05 is present and DQB1*02 is absent.
To calculate hands-on time for execution and analysis, runs of eight samples were used. When running larger series, particularly, analysis time per sample will be reduced further depending on the kit. The total hands-on time for setting up the assay was similar for the MLPA and XeliGen kits, while this was significantly shorter for the CeliaSCAN assay. Due to an overnight step in the MLPA method, the running time is relatively long for this kit.
Overall user friendliness for both experimental setup and software is the highest for the CeliaSCAN kit. The software is extremely simple to use, however, a disadvantage of this uncomplicated software is the lack of direct insight into potential problems with, for example, sample quality or execution errors when there is an invalid result. However, there is a contact address from the manufacturer available to solve the problem if the troubleshooting guide in the instructions for use is not sufficient. The MLPA software is more complicated and takes more training to use it efficiently. The advantage is, however, that it provides direct sample-specific information on potential problems with, for example, DNA quality when there is an invalid result. The XeliGen kit provides a scoring list that needs to be filled out by hand and interpreted according to a results table. Software for analysis and troubleshooting is not provided, but there is a short troubleshooting guide provided in the manual.
The CeliaSCAN and XeliGen kits provide all reagents; the MLPA kit only provides PCR reagents. Nevertheless, the reagent cost price is the lowest for the MLPA kit. The XeliGen kit is the most expensive. For both the XeliGen and CeliaSCAN kits, a real time (RT) thermocycler is needed, while for the MLPA kit both a thermocycler and a capillary electrophoresis instrument are needed (see the respective kit instructions for suitable platforms), which may lead to higher equipment (investment) costs for the MLPA kit as an RT thermocycler is, opposed to capillary electrophoresis equipment, relatively standard laboratory equipment.
Typing accuracy
The aim of this study was not to validate the kits, nevertheless, the concordance between the kits and SSCP assay for these selected samples was determined. There was one apparent discrepancy among the 50 samples tested. This sample was identified as HLA-DQ8 positive by SSCP, CeliaSCAN, and MLPA. The XeliGen kit typed this sample as DQA1*01 and 03; DQB1* 03:05 (DQB1*03:02 negative) and DRB1*04; according to the result sheet of the XeliGen kit, this patient is not at risk for developing CD. This sample was therefore retyped for HLA-DQB1 and -DQA1 with PCR-SSOP (LABType® SSO typing kit; One Lambda, Inc., Canoga Park, CA) following the manufacturer's protocol. This retyping confirmed that the sample is DQB1*03:05 positive, which is strictly speaking HLA-DQ8.
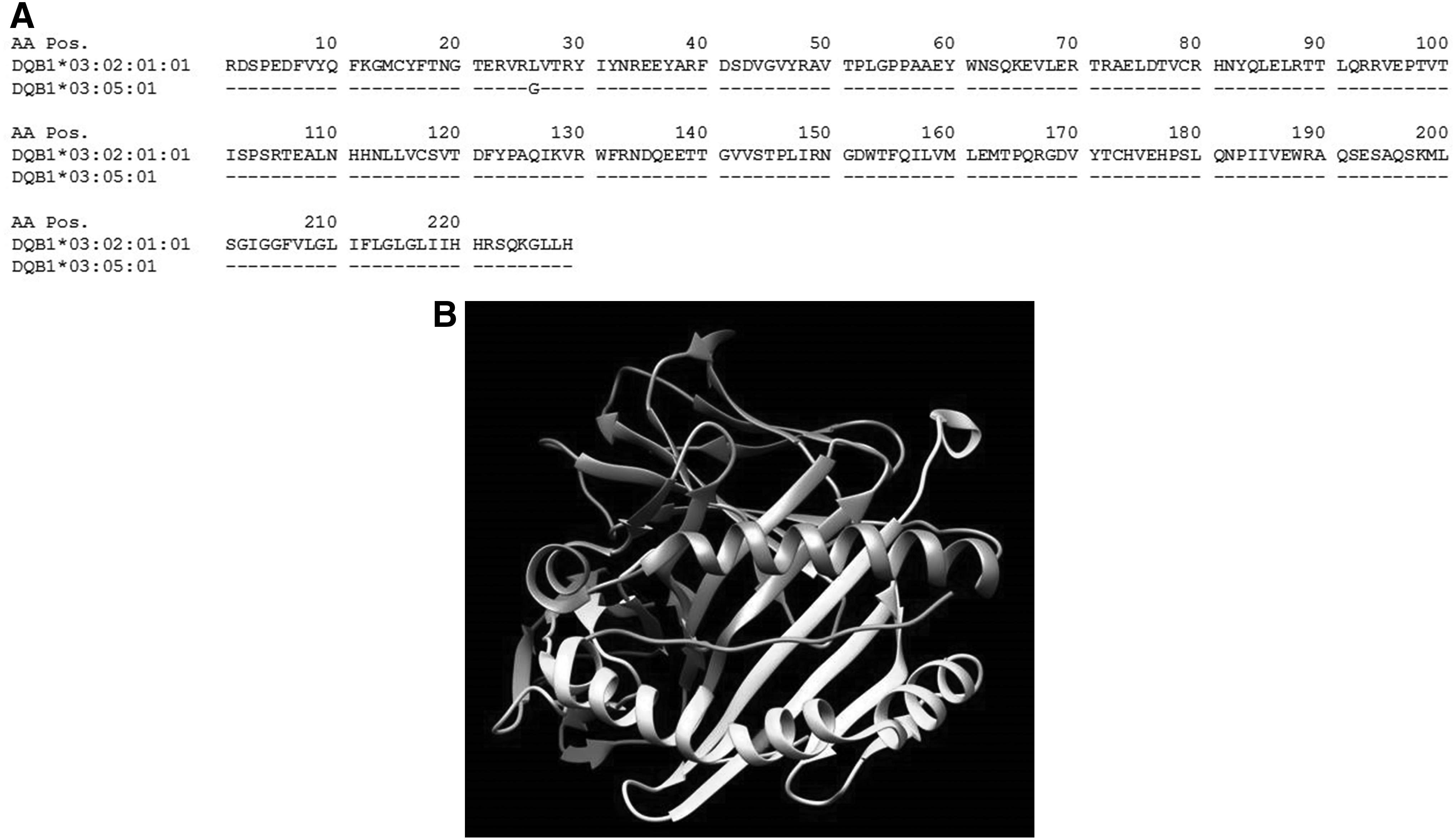
Sequence alignments of DQB1*03:02 and DQB1*03:05 show 5 base-pair sequence differences and only one amino acid change at position 26 (Fig. 1a). Structural analysis predicts similar interaction with gliadin peptides (Fig. 1b). Although this needs to be confirmed by binding analysis, based on these data, future development of CD may not be completely excluded in patients positive for this allele. Whether other low-frequent HLA-DQB1*03 variants with identical peptide binding domains to DQB1*03:02 and DQB1*03:05 † play a role in CD is not clear, but given their rarity, the impact of these alleles is expected to be very low.
Although HLA-DQ7 does not implicate an increased risk for CD, the aforementioned studies (Karell et al., 2003; Araya et al., 2015; Tinto et al., 2015; Martinez-Ojinaga et al., 2018) suggest that CD may not be completely ruled out in HLA-DQ2.2-, HLA-DQ2.5-, and HLA-DQ8-negative, and HLA-DQ7-positive individuals, particularly when there is a high suspicion but atypical presentation. Analysis of the endogenously presented peptide repertoire of HLA-DQ2.5 and HLA-DQ7.5 (DQA1*05, DQB1*03:01) revealed that the repertoire of HLA-DQ7 is significantly different from the HLA-DQ2.5 repertoire. HLA-DQ7-restricted epitopes lack charged residues, which suggests that, should they exist, HLA-DQ7.5-restricted gliadin epitopes do not need glutamine deamidation by tissue transglutaminase (Bergseng et al., 2015). In these cases, tissue transglutaminase autoantibodies may therefore be lacking as well.
Conclusion
In conclusion, all tested kits correctly identify the CD risk genes, although the conclusions regarding DQB1*03:05-positive samples with the XeliGen kit may need to be adapted. The XeliGen kit is relatively expensive, and no analysis or troubleshooting software is provided, but it is the only kit of the tested kits that directly detects HLA-DQ7. The MLPA kit is cheapest in terms of reagents and has software that directly provides sample-specific troubleshooting information, but may be more expensive in terms of equipment costs and needs more hands-on time than the CeliaSCAN kit. The CeliaSCAN kit and analysis software are easy to use, although the software does not provide direct sample-specific troubleshooting.
Indirect typing of HLA-DQ7 and HLA-DQ7.5 may be possible with the MLPA and CeliaSCAN kits, respectively. The resources of the laboratory and the intended use, that is, risk assessment for CD, diagnosis of complicated cases, family screening, research purposes, or a combination of the aforementioned, should determine the preference for any of the here-described HLA-DQ typing kits.
Footnotes
Acknowledgments
We thank TubaScan, MRC Holland (R. Vijzelaar), and Launch diagnostics, distributor for Eurospital (T. Jans), for providing reagents free of charge.
Author Disclosure Statement
No competing financial interests exist.