
Abstract
Aims:
Ficolin-3 is a circulating pattern recognition molecule of the lectin pathway, which participates in the host immune responses to cancer. Our study aimed to evaluate the prognostic efficacy of ficolin-3 in patients with esophageal cancer (EC).
Methods:
A total of 233 patients with EC were recruited for this study during a period from March 2013 to March 2016. Clinical information and pretherapeutic tumor specimens from all of the patients were analyzed. Serum ficolin-3 levels were determined by enzyme-linked immunosorbent assay. Patients were then assigned into quartiles according to their serum ficolin-3 levels. The Cox proportional hazards model was utilized to explore the correlation between ficolin-3 levels with overall survival (OS) and disease-specific survival (DSS).
Results:
The serum ficolin-3 level in the esophageal squamous cell carcinoma (ESCC) group was significantly higher than in the esophageal adenocarcinoma (EAC) group (19.59 ± 4.35 ng/mL vs. 18.39 ± 5.42 ng/mL, p < 0.01). There were great differences in prevalence of ESCC, tumor length, involvement of adventitia, and lymph node status among patients in different ficolin-3 groups (all p < 0.01). Both univariate analyses and further multivariate analyses revealed the close association between ficolin-3 levels and EAC (For OS and DSS, all p < 0.05). Out of 233 patients, survival information was available for 220, including 100 (45.45%) females and 120 (54.54%) males. When dividing the ficolin-3 levels into quartiles, patients with higher serum ficolin-3 levels showed a trend toward longer OS and DSS no matter whether they were diagnosed as ESCC or EAC (HR 0.21-0.55, all p < 0.05).
Conclusions:
Serum ficolin-3 levels were identified as an independent prognostic biomarker for DSS and OS in Chinese patients with EC, especially EAC.
Introduction
Esophageal cancer (EC) is the sixth leading cause of cancer-related deaths and the eighth most common cancer worldwide; it can be subdivided into two major histologic types: esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma (EAC) (Ferlay et al., 2010). There are a plethora of differences among both the clinical and molecular features between these two cancer types.
Worldwide, there were an estimated 398,000 ESCC cases and 52,000 EAC cases in 2012, translating to incidence rates of 5.2 and 0.7 per 100,000 persons, respectively. The highest burden of ESCC was found in South-Eastern and Central Asia (79% of the total global SCC cases) (Ferlay et al., 2015). China contributed approximately half of the new global EC cases in 2012; it was also the sixth most common cancer in China in 2011 (Chen et al., 2015). The most recent population-based cancer registration data in the crude incidence and mortality rates in China for EC were 21.62/100,000 and 16.25/100,000 persons, respectively, which were both much higher than those in developed countries (Zeng et al., 2016). EC causes a heavy burden and remains a major public health issue in China. Primary and secondary prevention are essential for disease control.
The development of malignant tumors induced immune responses against tumor cells as host defense mechanisms, mainly including cell- and humoral factor-mediated pathway (Zimmermann-Nielsen et al., 2002). Complement system was a major effector pathway among humoral factor-mediated responses (Zimmermann-Nielsen et al., 2002). The complement system had classically been implicated not only as a defense against infection by microorganisms and parasites but it also participated in host immune responses to cancer (Inoue et al., 2002). There were three different routes, including classical, lectin, and alternative pathways, which could mediate the activation of the complement system. In human, five recognition molecules of the lectin pathway had been described: mannose-binding lectin (MBL), ficolin-1 (M-ficolin), ficolin-2 (L-ficolin), and ficolin-3 (H-ficolin or Hakata antigen), and collectin-11 (Garred et al., 2009; Ma et al., 2013). Among these, ficolin-3 appeared to have the strongest potential in the complement activation (Prohaszka et al., 2013). Recently, a decreased level of serum ficolin-3 was subsequently found in Type 2 diabetes, gestational diabetes mellitus (GDM), and diabetic peripheral neuropathy (DPN) (Li et al., 2008; Zhang et al., 2016; Yuan et al., 2018b). There was also a report of an elevated level of ficolin-3 in the vitreous fluid of patients with hyperplastic diabetic retinopathy (Zheng et al., 2011). As research on ficolin-3 has increased, it has been revealed that the serum ficolin-3 levels are associated with the outcomes of acute ischemic stroke, traumatic brain injury, chronic heart failure, leprosy, and many other diseases. Notably, Szala et al. (2013) reported a close relationship between serum ficolin-2 and ficolin-3 levels in women with both malignant and benign ovarian tumors, and confirmed the elevation of ficolin-3 in ovarian cancer and obtained similar results with ficolin-2. However, no relevant study has been undertaken to explore the use of ficolin-3 as prognostic biomarker in Chinese patients with EC.
Considering the high mortality rate and impaired quality of life during treatment for EC, there is an urgent need for prognostic biomarkers that can help predict recurrence, sensitivity to therapy, and ultimately lead to better personalized care of patients. Previous studies associated with prognostic biomarkers for ESCC or EAC have focused on indexes related to the biological behavior of tumors or relevant protein and DNA expression, such as tumor length and phospholipase C epsilon 1 (PLCE1) (Zeybek et al., 2013; Cui et al., 2014). The effect of serum microRNA levels in predicting prognosis of EC has also been frequently discussed in recent years (Jiang et al., 2015). Their predictive values, however, are not satisfactory. Therefore, we carried out this study to clarify the potential connection between ficolin-3 with EC and assess the prognostic value of serum ficolin-3 levels for ESCC and EAC in Chinese patients.
Materials and Methods
Study population
A total of 233 patients with EC at the People's Hospital of Xixian (Henan Province, China) were recruited for this study during a period from March 2013 to March 2016. The medical records of these patients were reviewed retrospectively. Clinical information and pretherapeutic tumor specimens from all of the patients were analyzed. Patients who had received neoadjuvant chemoradiotherapy after a noncurative resection and patients who died in the hospital in the early postoperative term were excluded. All patients were evaluated by means of barium meal, esophagogastroscopy, and computed tomography of the chest and abdomen for preoperative staging. Written informed consents were obtained from all participants. The study was approved by the Human Research and Ethics Committee of People's Hospital of Xixian with adherence to the tenets of the Declaration of Helsinki.
Data collection and anthropometric measurements
Information on age, weight, height, and history of smoking, drinking, diabetes, and hypertension were obtained via a questionnaire. The body mass index (BMI) was calculated as the weight (kg) divided by the square of height (m).
Serum ficolin-3 measurement
Blood samples were collected from an antecubital vein before treatment and the serum cryopreserved for the determination of ficolin-3 levels. The serum ficolin-3 concentrations were determined by enzyme-linked immunosorbent assays (ELISAs) (Hycult biotech, Netherlands). The intra-assay and interassay variations were 3.5% and 5.5%, respectively. Serial dilutions of recombinant ficolin-3 were included in all assays as a standard.
Statistical analysis
For the statistical analysis, SPSS v. 16.0 (SPSS, Inc., Chicago, IL) was used. Figures were created by GraphPad Prism 5.0 (GraphPad Software, Inc.). Data are expressed as mean ± standard deviation for continuous variables and percentages (%) for categorical variables. Differences among the groups were analyzed using the Student's t-test or chi-square test as appropriate for the measurement data. Multiple logistic regression analyses were performed to evaluate the odds ratios and associated factors. For each cohort (ESCC and EAC), the survival analysis was carried out by dichotomizing the ficolin-3 value using the average level as a cutoff. Survival estimates were calculated according to the Kaplan-Meier method and compared using the univariate Cox proportional hazards model. All p values were two-tailed, and p < 0.05 was considered statistically significant.
Results
Demographic characteristics between ESCC and EAC
Data from 134 ESCC and 86 EAC patients were collected during our study. The study population (n = 220, 120 men and 110 women) had a mean age of 65.94 ± 9.91 years, ranging from 36 to 85 years at the time of diagnosis, with a median survival time of 7.9 ± 1.9 (confidence interval [95% CI] 5.9-10.6) months. A summary of the characteristics, including the clinical and tumor information of the patients in the ESCC and EAC groups is shown in Table 1. There were no significant differences in sex, age, distribution of smoking, alcohol use, and tumor clinical N and M stages between the two groups of patients. Compared to EAC, the patients with ESCC had a significantly higher BMI value (24.72 ± 3.09 vs. 24.10 ± 4.10), percentage of diabetes (41.8% vs. 24.4%), and serum ficolin-3 levels (19.59 ± 4.35 vs. 18.39 ± 5.42), along with much lower percentage of hypertension (26.9% vs. 43.0%) (all p < 0.05). The distribution of the tumor topography stage between ESCC and EAC was also of significant difference (all p < 0.05).
Characteristics of Patients with Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma
p < 0.05 between two groups.
BMI, body mass index; EAC, esophageal adenocarcinoma; ESCC, esophageal squamous cell carcinoma.
Comparison of variables between different ficolin-3 groups
The patients were also divided into two groups according to the average value of serum ficolin-3 levels. The patients' demographics and clinical tumor data for the two groups with different ficolin-3 levels are summarized in Table 2. There were remarkable differences in tumor length, clinical stage, and the percentage of diabetes and ESCC between the groups (all p < 0.01). The tumor length (5.27 ± 1.51 vs. 3.62 ± 1.14) and incidence of diabetes (57.3% vs. 52.7%) and ESCC (70.0% vs. 51.8%) in the high ficolin-3 group were significantly higher than the low ficolin-3 group (all p < 0.01).
Patients and Tumor Characteristics Between Ficolin-3 Groups
p < 0.05 between two groups.
Association of serum ficolin-3 level with risk for EC
A univariate analysis of all variables was performed to determine the association between serum ficolin-3 levels with risk for EC. As shown in Table 3, there was a significant positive association between being at high risk for EAC and an elevated level of serum ficolin-3. It was observed that the risk of death from any cause and the risk of disease-specific death in EAC were positively associated with higher serum ficolin-3 levels (both p < 0.01). In addition, nodal classification was significantly associated with risk of death from any cause and disease-specific death in EAC (both p < 0.05). However, there was no significant trend between death risk of ESCC and ficolin-3, no matter death from any cause or disease-specific death.
Univariate Analyses of Variables with Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma
p < 0.05 between two groups.
CI, confidence interval.
After adjusting for all other potential confounders, including gender, age, BMI, smoking, drinking, diabetes, hypertension, tumor classification, and nodal classification, the association between the risk of death in EAC and ficolin-3 still existed. As shown in Table 4, results of the multivariate analyses indicate an increased risk of death from any cause and the risk of disease-specific death with ficolin-3 in patients with EAC (both p < 0.01). Nodal classification was also significantly associated with the risk of disease-specific death in EAC (p < 0.05).
Multivariate Analyses of Variables with Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma
p < 0.05 between two groups.
Prognostic value of serum ficolin-3 levels in ESCC and EAC
To assess the potential prognostic impact of ficolin-3, serum ficolin-3 level values derived from ELISA analyses were dichotomized into quartiles (ng/mL) (Q1: >30.17; Q2: 21.29-30.17; Q3: 13.92-21.29; Q4: <15.67). Taking Q4 as referent, Cox proportional hazards analysis showed a trend toward a better overall survival (OS) for ESCC patients with Q1 and Q2 (Q1: HR 0.29; 95% CI 0.19-0.44; Q2: HR 0.55; 95% CI 0.37-0.82; both p < 0.01) (Fig. 1A). Similarly, when evaluating disease-specific survival (DSS), a better outcome was observed in patients of Q1 and Q2 by taking Q4 as referent (Q1: HR 0.25; 95% CI 0.18-0.33; Q2: HR 0.54; 95% CI 0.34-0.74; both p < 0.01) (Fig. 1C).
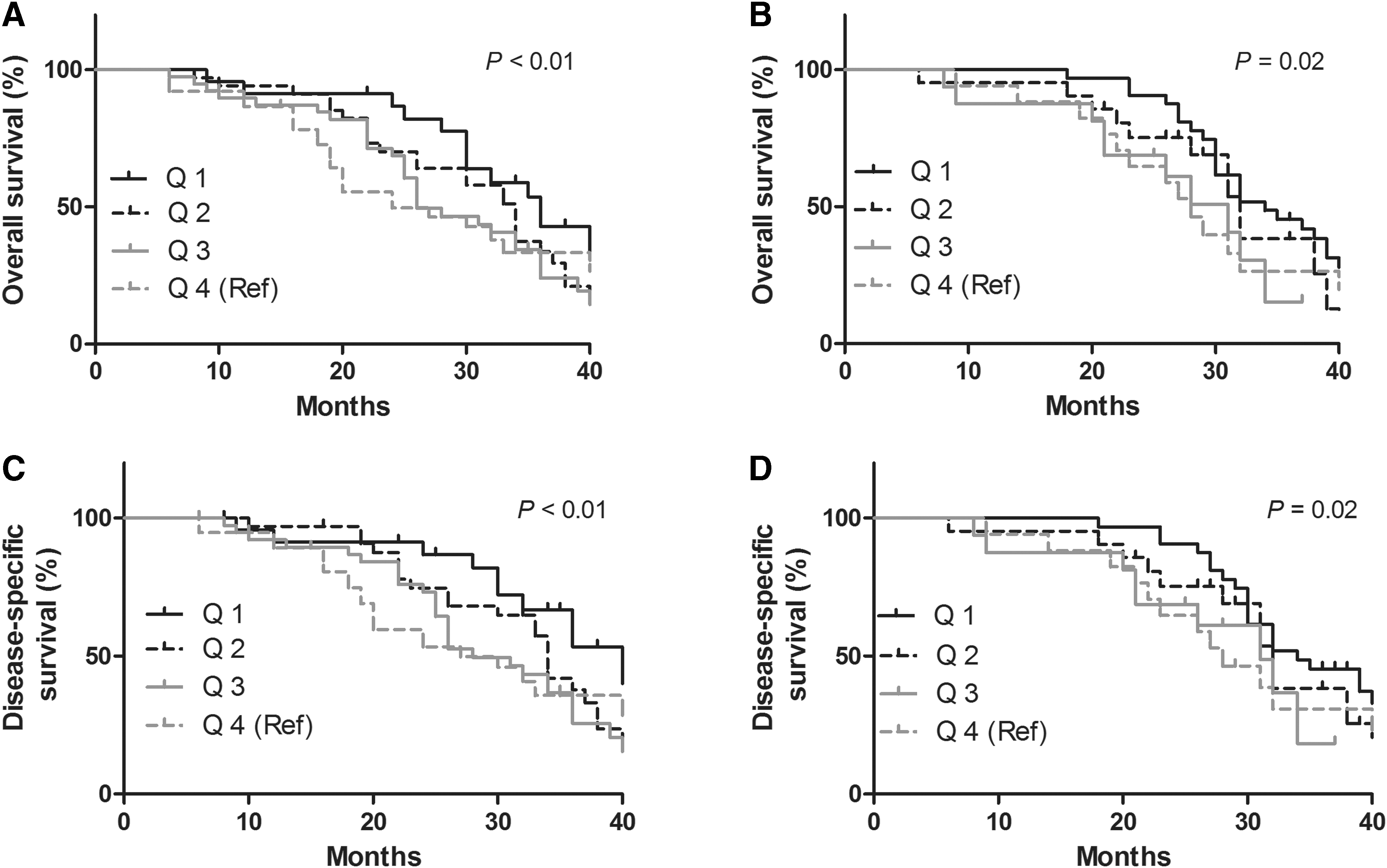
Kaplan-Meier survival of ESCC and EAC patients according to serum ficolin-3 level (ng/mL).
When analyzing the association in EAC, a significantly correlation between longer OS and increased serum ficolin-3 level was observed for EAC patients in Q1 (HR 0.21; 95% CI 0.11-0.32; p = 0.02) (Fig. 1B). In addition, by taking Q4 as referent, a trend toward a longer DSS was shown for patients with higher serum ficolin-3 level in Q1 (HR 0.23; 95% CI 0.17-0.39; p = 0.02) (Fig. 1D).
Discussion
In this study, we investigated the relationship between death risk and serum ficolin-3 levels in patients with EC. We analyzed the difference in ficolin-3 levels between patients with ESCC and EAC and evaluated the correlation of ficolin-3 with OS and DSS. The results of this retrospective cohort study revealed that serum ficolin-3 levels were observably associated with the characteristics and prognosis of EC. There was a significant trend toward poorer OS or DSS for patients with increased serum ficolin-3 levels, regardless of whether they suffer from ESCC or EAC. This suggests that a high serum ficolin-3 level is not only an independent-associated factor of EC but also provides us a new potential pathway in the prognostic judgment of ESCC or EAC.
Improvements in the early detection of EC and optimal selection of appropriate treatment for patients might help to improve the OS rates. Currently, tumor features, including tumor grade, stage, and histological type, are the most commonly used clinical parameters in predicting the prognosis of EC (Kaz and Grady, 2014). Although these parameters are the best known prognostic markers, they are suboptimal for the accurate prediction of an individual's disease-free and OS (Zhang and Guo, 2010). To improve the accuracy of the determination of every patient's prognosis, recent research has focused on genetic changes, which are involved in the development and progression of EC (Kaz and Grady, 2014). The tumor suppressor cyclin-dependent kinase inhibitor 2A (CDKN2A) (p16INK4a), which blocks phosphorylation of the Rb protein and inhibits cell cycle progression, was one of the first genes shown to be methylated in Barrett's esophagus (BE) and EAC. The incidence of DNA methylation of the genes somatostatin (SST), tachykinin-1 (TAC1), neural EGFL-like 1 (NELL1), cadherin 13 (CDH13), and A-kinase anchoring protein 12 (AKAP12) were evaluated in ∼260 esophageal tissue specimens in a series of reports (Urashima et al., 1997; Jin et al., 2008a, 2008b). Although all these genes have the potential to be used as diagnostic molecular markers for BE or EAC, none of them has been subjected to rigorous validation studies (Kaz and Grady, 2014). Hypermethylation of CDKN2A in ESCC cases mostly ranged from 40% to 60%. It was revealed that expression loss of CDKN2A is associated with an advanced histological grade of cancer (Guo et al., 2006; Salam et al., 2009). The APC gene demonstrates a frequent methylation in both EAC and ESCC patients and shows a trend of reduced survival in ESCC patients after treatment (Zare et al., 2009). Other studies also evaluated the utility of epigenetic and gene biomarkers for estimating the risk of EC recurrence after treatment and include, but not limited to secreted frizzled-related protein 1 (SFRP1), dickkopf WNT signaling pathway inhibitor 3 (DKK3), and runt-related transcription factor 3 (RUNX3) (Lima et al., 2011). In addition to epigenetic biomarkers, patients' age or tumor length has been evaluated for use to predict survival rate and other clinical aspects of EC (Mirinezhad et al., 2014). However, the positive methylation status is regarded as a better predictor of survival stage (Brock et al., 2003). After reviewing previous studies associated with the prognosis of EC, we found that this retrospective cohort study was the first report which discussed the relationship between ficolin-3 and EC and evaluated the potential prognostic effect of serum ficolin-3 levels for EC in Chinese patients.
As we mentioned before, the complement system played an important role in host immune responses to tumor cells (Zimmermann-Nielsen et al., 2002). In lectin pathways to mediate the activation of the complement system, five recognition molecules were reported (Inoue et al., 2002). It was reported that ficolin-3 was the predominant plasma molecule with a median concentration of 25 ng/mL in healthy Caucasians, followed by ficolin-2 and MBL, respectively. The important effect of ficolin-3 in immune system drew our attention at first. After reviewing the related researches, we found that altered expression of three complement regulatory proteins, decay-accelerating factor (CD55), membrane cofactor protein (CD46), and homologous restriction factor 20 (CD59) has been identified in human gastrointestinal malignancies and EC (Inoue et al., 2002; Shimo et al., 2004). Ficolins constitute a group of major serum pattern recognition molecules of the innate immune system, which promote opsonization of infecting microorganisms and activate the lectin pathway of complement (Endo et al., 2007). Ficolins' structure consists of an N-terminal cysteine-rich region, a collagen-like domain, and a C-terminal globular fibrinogen-like domain (Endo et al., 2011). It has been shown that ficolin-3 mRNA is expressed in the liver and lung and secreted into the bile, bronchus, and circulation. The circulating concentration of ficolin-2 and ficolin-3 are much higher than ficolin-1 (Matsushita, 2010). Recently, the novel effect of ficolin-3 toward predicting GDM in pregnant women has garnered attention (Yuan et al., 2018a). The ratio of ficolin-3/adiponectin during early gestation in pregnant women might provide effective early predicting and screening for GDM (Yuan et al., 2018a). Another study compared the concentration of serum ficolin-3 between diabetic patients with or without DPN. The results showed that lower ficolin-3 levels are independently associated with DPN, and it may be a potential biomarker for DPN (Zhang et al., 2016). Other epidemiologic studies indicate a close relationship between ficolin-3 and severity or outcome of chronic heart failure, leprosy, traumatic brain injury, and Crohn's disease (Prohaszka et al., 2013; Schaffer et al., 2013; Pan et al., 2015; Andrade et al., 2017). High ficolin-3 levels were also reported to be associated with systemic lupus erythematosus (Plawecki et al., 2016), ovarian tumors (Szala et al., 2013), and seem to be a risk factor for a shorter graft survival rate from kidney transplantation (Smedbraten et al., 2015). Indeed, we observed an association between ficolin-3 and EC and identified the prognostic effect of serum ficolin-3 levels in Chinese patients with ESCC and EAC. This is the first report to analyze the value of ficolin-3 in serving as a prognostic marker for EC.
This study is not without its limitations. First, the number of patients with EC in this single-center study was relatively small, especially for EAC. Second, there was no significant association between tumor classification and risk of EC, no matter ESCC or EAC, which might be associated with the statistical method of tumor classification and retrospective study type. It was a retrospective single center analysis, lacking the long-term follow-up outcome of survival in patients with higher serum ficolin-3 levels. Finally, the evaluation of ficolin-3 levels in our study only used serum ficolin-3 values via ELISA detection. There was a shortage of comparisons of ficolin-3 protein expression in the esophageal tissue of patients with ESCC and EAC and analysis of the association between ficolin-3 protein expression levels and survival data of patients with EC.
In summary, the serum ficolin-3 level appears to be an independent factor that is prognostic for OS and DSS of EAC in the Chinese patients. Serum ficolin-3 can be measured efficiently and inexpensively making it an attractive serum marker for further studies in EC. Ficolin-3 expression in esophageal tissue and prospective follow-up trials of serum levels are needed to determine the prognostic value of this biomarker.
Conclusions
This study is the first report to associate a relationship between serum ficolin-3 levels and EC in Chinese patients. Serum ficolin-3 levels are an independent associated factor for OS and DSS in patients with EAC. Kaplan-Meier analysis showed a trend toward longer OS and DSS in patients with higher serum ficolin-3 level no matter ESCC or EAC.
Footnotes
Acknowledgments
The authors thank the patients and volunteers recruited from People's Hospital of Xixian for participating in the research.
Author Disclosure Statement
No competing financial interests exist.