
Abstract
Background:
Epstein-Barr virus (EBV) infection and microRNA-155 (miR-155) are considered etiological factors that contribute to nasopharyngeal carcinoma (NPC). The regulation of miR-155 expression induced by EBV infection has been reported to be important in NPC tumorigenesis.
Aims:
This study was designed to explore the relationships among the expression levels of miR-155, LMP-1 (latent membrane protein-1), and LMP-2 (latent membrane protein-2) in tumor and nontumor specimens of Vietnamese NPC patients. The study was also designed to investigate the association between miR-155 expression and LMP-1 and LMP-2 expression in Vietnamese NPC patients.
Materials and Methods:
Ninety-three NPC biopsy samples and 100 noncancerous swab specimens were collected from patients and analyzed by real-time reverse transcriptase polymerase chain reaction.
Results:
LMP-1, LMP2, and miR-155 were significantly upregulated in 76.34%, 67.74%, and 75.27% of NPC samples, respectively, with decreased expression observed in the control group (p < 0.0001). Moreover, the statistical analysis showed that there was a close association between LMP-1 and LMP-2 expression and miR-155 expression in the NPC samples.
Conclusion:
miR-155 expression was upregulated and significantly associated with the expression of LMP-1 and LMP-2, in Vietnamese NPC cases.
Introduction
MicroRNAs (miRs or miRNAs), originally discovered in Caenorhabditis elegans by Lee et al. (1993) and typically represent ∼20 nucleotides in length, are an abundant class of evolutionarily conserved, small noncoding RNAs. miRNAs play important roles in regulation of gene expression by binding to sequences in the 3′-untranslated region of their target mRNAs, resulting in blocking of their translation (Bartel, 2004; Ha and Kim, 2014). Their target regulation activities are involved in numerous cellular processes, including cell proliferation, differentiation, apoptosis, and metabolism (Bartel, 2004). In recent years, growing evidences indicate that miRNAs function as both oncogenes and tumor suppressor genes, and the abnormal expression of miRNAs contributes to many human tumor pathogenesis, including nasopharyngeal carcinoma (NPC) and other cancers (Calin and Croce, 2006; Faraoni et al., 2009; Macfarlane and Murphy, 2010; Du et al., 2011; Lovat et al., 2011; Amin and Lam, 2015; Lee et al., 2016; Lao et al., 2018). Therefore, for miRNAs to be clinically applied, it is necessary to identify whether miRNAs play major functions as oncogenic miRNAs or tumor suppressors in the pathogenesis of human tumorigenesis.
The understanding of miRNAs' role will make the development of molecular target therapy possible, by their suppression or reactivation. Among the known oncomiRs, miR-155, an evolutionarily conserved miRNA encoded by the MIR155 host gene (also named MIR155HG), stands out as an important entity (Teng and Papavasiliou, 2009). The dysregulation of miR-155 has been linked to different biological processes, including hematopoiesis, inflammation, immunity, as well as the development of various human cancers, such as NPC and breast cancer (Faraoni et al., 2009; Du et al., 2011; Tili et al., 2009; Jiang et al., 2010; Higgs and Slack, 2013; Zhu et al., 2013; Vigorito et al., 2013; Wan et al., 2016). As such, miR-155 has been considered an important target for diagnosis, prognosis, and cancer therapy (Higgs and Slack, 2013). Zhu et al. (2013) reported that miR-155 was upregulated in NPC tissue. The overexpression of miR-155 induced NPC cell proliferation, cell migration, and invasion (Zhu et al., 2013).
A well-established etiological factor of NPC is its strong association with the Epstein-Barr virus (EBV), a ubiquitous human γ-herpes-virus (Mahdavifar et al., 2016, Rowe et al., 1992; Vera-Sempere et al., 1996; See et al., 2008). Latent EBV infection has been reported to be an early event in the development of human cancer (Pathmanathan et al., 1995). Among the latent gene products, LMP-1 (latent membrane protein-1) and LMP-2 (latent membrane protein-2) have been shown to display useful oncogenic targets of NPC diagnosis (Hao et al., 2004; See et al., 2008; Lao et al., 2017). LMP-1 encodes its LMP that induces morphological and phenotypic alterations in epithelial cells (Hao et al., 2004; Kang and Kieff, 2015; Dawson et al., 2012). LMP-2 is considered to play an important role in carcinogenesis by driving EBV into latency (Thompson and Kurzrock, 2004; Dawson et al., 2012). Many previous studies showed that LMP-1 and LMP-2 are considered the molecular prognostic and diagnostic as well as the outcome of therapy in NPC (Hao et al., 2004; Hariwiyanto et al., 2010; Rosales-Pérez et al., 2014; Lao et al., 2017).
It is worth emphasizing that EBV could downregulate or upregulate some miRs and contribute to increased tumor incidence in NPC cells (Yu et al., 2012; Zhao et al., 2012). miR-155 expression has been proven to be upregulated in NPC cell line and EBV-positive NPC tissue samples collected from Chinese NPC patients. In recent years, more attention has been gradually focused on the relationship between the role of miR-155 and EBV presence. Du et al. (2011) reported that miR-155 was upregulated in NPC tissue, partly driven by LMP1 and LMP2. In the study of Zhu et al. (2013), they determined the expression of miR-155 in the EBV-positive NPC tissues and EBV-infected NPC cell line, and concluded that miR-155 upregulation was associated with LMP-1 DNA accumulation and contributed to nasopharyngeal tumorigenesis. The EBV LMP-1 activating the expression of miR-155 through the nuclear factor-κB (NF-κB) pathway has been reported, and the underlying mechanisms of oncogenic roles in NPC progression need further evaluation (Gatto et al., 2008).
Vietnam, located in Southern Asia, is well known for its high incidence and mortality rate of NPC within 86,691 cases (age-standardized rate (ASR) = 1.2/100,000) and 50,831 deaths (ASR = 0.7/100,000) (GLOBOCAN, 2012; Mahdavifar et al., 2016). However, to our knowledge, the detection and evaluation of miR-15, LMP-1, and LMP-2 expression as well as the association among them in Vietnamese NPC patients have not been reported yet. Therefore, this is the first case/control study that focused on Vietnamese local clinical NPC samples with the aim to explore the characteristics of the expression of miR-155, LMP-1, and LMP-2 as well as their association in Vietnamese NPC samples, as well as to support that the miR-155, LMP-1, LMP-2 can be a potential target for anticancer therapy in NPC.
Methodology
Ethics statement, sample collection
Institutional Ethics Board approval was obtained from the Medical Ethics Committee of the Cho Ray Hospital, Ho Chi Minh City, Vietnam (the decision number of the permission: 516/BVCR-HDDD). All the samples used in this study were approved by Cho Ray Hospital and obtained from all participants. The patients enrolled in this study were required to sign consent forms to approve the usage of the samples for laboratory work and analysis.
A total of 93 NPC biopsy tissues that were archived were obtained from the Cho Ray Hospital, Vietnam. All the samples were submitted to the histopathological department and were subsequently confirmed by hematoxylin and eosin staining (Fig. 1A). Also, 100 nonmalignant swab samples that were negative for NPC were collected from non-NPC patients. In brief, a 15-cm-long cotton stick was inserted into the nasal cavity and moved toward the nasopharyngeal wall; it was then swept over the surface of the posterior and lateral nasopharyngeal wall. The cotton stick was withdrawn and immediately immersed in phosphate-buffered saline stored at −20°C for further experiments.

Histological examination of
Total RNA extraction and real-time polymerase chain reaction assay
RNAs, including miRNAs and mRNA, were isolated from NPC biopsy samples and noncancerous samples by applying the mirVana TM miRNA Isolation Kit (Ambion, Life Technology). cDNA was reverse transcribed from ∼5 ng of total RNA using the High Capacity cDNA Reverse Transcription Kit (Thermo Fisher Scientific) (for LMP-1 and LMP-2 detection) and TaqMan® Advanced miRNA cDNA Synthesis Kit (for miR-155 detection) (Thermo Fisher Scientific). All the RNA extraction and the reverse transcriptions assays were performed according to the manufacturer's instructions. For miR-155, quantitative real-time (qRT)-polymerase chain reaction (PCR) was performed by the TaqMan Advanced miRNA assay kit (Thermo Fisher Scientific), and UniSp6 rRNA was used as the internal control candidate. For LMP-1 and LMP-2, qRT-PCR was done by means of a qSYBR-green, and GAPDH was used as an endogenous control. The internal control candidate was used to normalize the Ct values of LMP-1, LMP-1, and miR-155 because of the nondifferential expression level in the tumor and noncancerous samples.
Statistical analysis
Data were analyzed using MedCalc® Version 12.7.0.0. All p values were two-sided, and values <0.05 were considered significant. All values were reported as mean ± standard error of mean. The relative expression of miR-155, LMP-1, and LMP-2 as determined using q-PCR was analyzed using the 2−ΔΔCt method within the endogenous control (Livak and Schmittgen, 2001). The findings greater and less than one were determined to classify upregulation and downregulation, respectively. The chi-square test was used to determine the association between the expressions of miR-155, LMP-1, and LMP-2 and NPC status, as well as the association between miR-155 expression and LMP-1 and LMP-2 expression. Moreover, the odds ratio (OR), relative risk (RR), and its 95% confidence interval (CI) are calculated according to Altman (1991). The p value for identification of the association between the expression of miR-155 and the risk of NPC was estimated according to Sheskin (2004).
Results
Sample collection
The characteristics of all 93 NPC patients are summarized in Table 1. The mean age of the 93 NPC cases was 53.51 ± 1.43 (range: from 20 to 81). Among them, the number of males (accounting for 73.12%) is more than that of females (accounting for 26.88%). Also, 100 nonmalignant swab samples, which were confirmed negative for NPC, were collected from non-NPC patients. Among them, the number of males (accounting for 60.00%) is more than that of females (accounting for 40.00%). Concerning the NPC biopsy samples, the age incidence profile indicated an increase in NPC risk up to late middle age (range: from 40 to younger than 60). Tumor histological types were classified according to the World Health Organization (WHO) classification for NPC criteria. Type 3 (undifferentiated carcinoma [UC]) accounted for the highest proportion of all types of NPC; 67.74% (n = 63) of NPC cases were classified as type 3 (UC). Stage wise, 48.39% (n = 45) of NPC patients were in an advanced stage, and no case was in the early stage (stage 1).
Characteristics of Nasopharyngeal Carcinoma Patients
Type 1, keratinizing squamous cell carcinoma; type 2, nonkeratinizing carcinoma; type 3, undifferentiated carcinoma.
Expression of LMP-1 and LMP-2 in NPC biopsy samples
Expression of LMP-1 and LMP-2 was quantified by real-time PCR by means of a qSYBR-green. GAPDH was used as the internal control for the evaluation of LMP-1 and LMP-2 expression in both NPC clinical samples (case group) and noncancerous samples (control group). Both the NPC clinical and noncancerous samples were positive for GAPDH (Fig. 2). In the NPC set, 71 of the 93 NPC specimens (accounting for 76.34%) were positive for LMP-1 expression (Table 2), whereas none of the controls was positive. Also, 63 of the 93 NPC samples (accounting for 67.74%) and 1 of the 100 noncancerous samples (accounting for 1.00%) were positive for LMP-2 expression, respectively (Fig. 2). Figure 2 shows the validity of expression for each gene in clinical NPC biopsy samples. A value of p < 0.0001 indicated that each gene expression was significantly associated with NPC. Using the LMP-1 expression, the OR and RR were 511.98 (95% CI = 30.68-8545.19, p < 0.0001) and 4.76 (95% CI = 3.38-6.67, p < 0.0001), respectively. NPC was diagnosed with a sensitivity of 76.34 (71 of the 93 NPC cases were positive), specificity of 100.00% (100 of the 100 control cases were negative), κ value of 0.73, and an AUC (area under the receiver operating characteristic curve) value of 0.86. Regarding verification with the LMP-2 expression, the OR and RR were 255.12 (95% CI = 33.79-1925.57, p < 0.0001) and 4.74 (95% CI = 3.36-6.68, p < 0.0001), respectively. NPC was diagnosed with a sensitivity of 67.74 (63 of the 93 NPC cases were positive), specificity of 99.00% (99 of 100 control cases were negative), κ value of 0.72, and an AUC value of 0.86. No significant association was found between LMP-1 and LMP-2 expression and other clinical characteristics, such as patient's gender (LMP-1: p = 0.06; LMP-2: p = 0.83), age (LMP-1: p = 0.19; LMP-2: p = 0.26), tumor histological types (LMP-1: p = 0.29; LMP-2: p = 0.28), as well as stage (LMP-1: p = 0.07; LMP-2: p = 0.40).
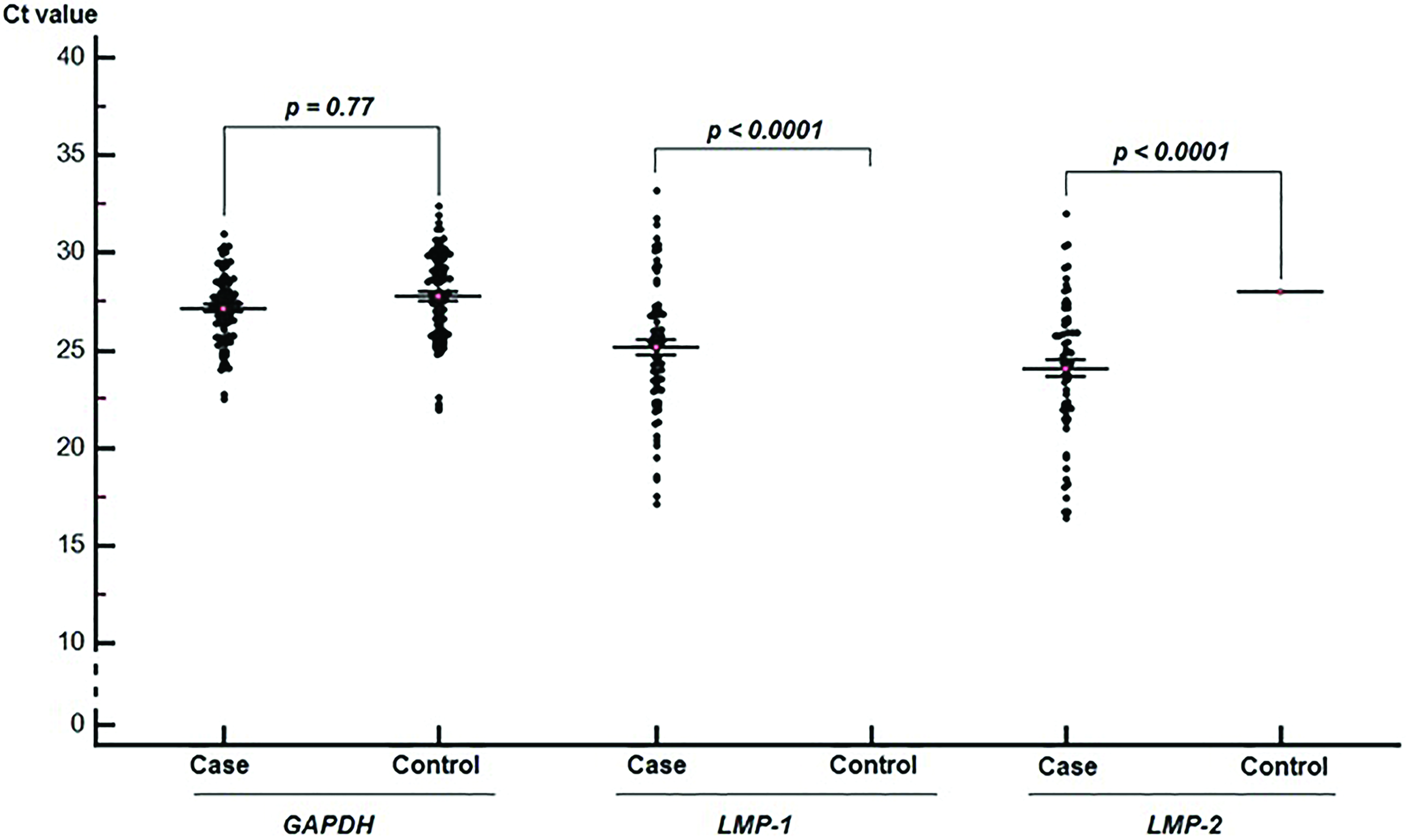
The mean Ct value (mean ± SE) of GAPDH, LMP-1, and LMP-2 in the case group and control group. Each black dot indicated the Ct value of each sample. The red dots indicate the mean of Ct. LMP-1, latent membrane protein-1; LMP-2, latent membrane protein-2; SE, standard error. Color images are available online.
Data Analysis of LMP-1, LMP-2, and miR-155 Expression
LMP-1, latent membrane protein-1; LMP-2, latent membrane protein-2; NPC, nasopharyngeal carcinoma.
The mean Ct values for GAPDH in the case and control groups were 27.14 ± 2.31 and 27.75 ± 2.24, respectively. No significant difference in the GAPDH expression was found between the case and control groups (p = 0.77). Therefore, GAPDH was suitable as a reference gene (internal control) to normalize LMP-1 and LMP-2 expression between the case and control groups. The mean Ct value of LMP-1 in the case group was 25.14, and no Ct value was recorded in the control group because no control samples were positive for LMP-1 expression. The mean Ct values of LMP-2 in the case and control groups were 24.07 and 27.97, respectively. Therefore, the relative expression of LMP-2 was computed by the 2−ΔΔCt method. The result shows that LMP-2 expression level was 9.78 times higher in NPC samples than noncancerous samples (2−ΔΔCt = 9.78, p < 0.05) (Fig. 3).
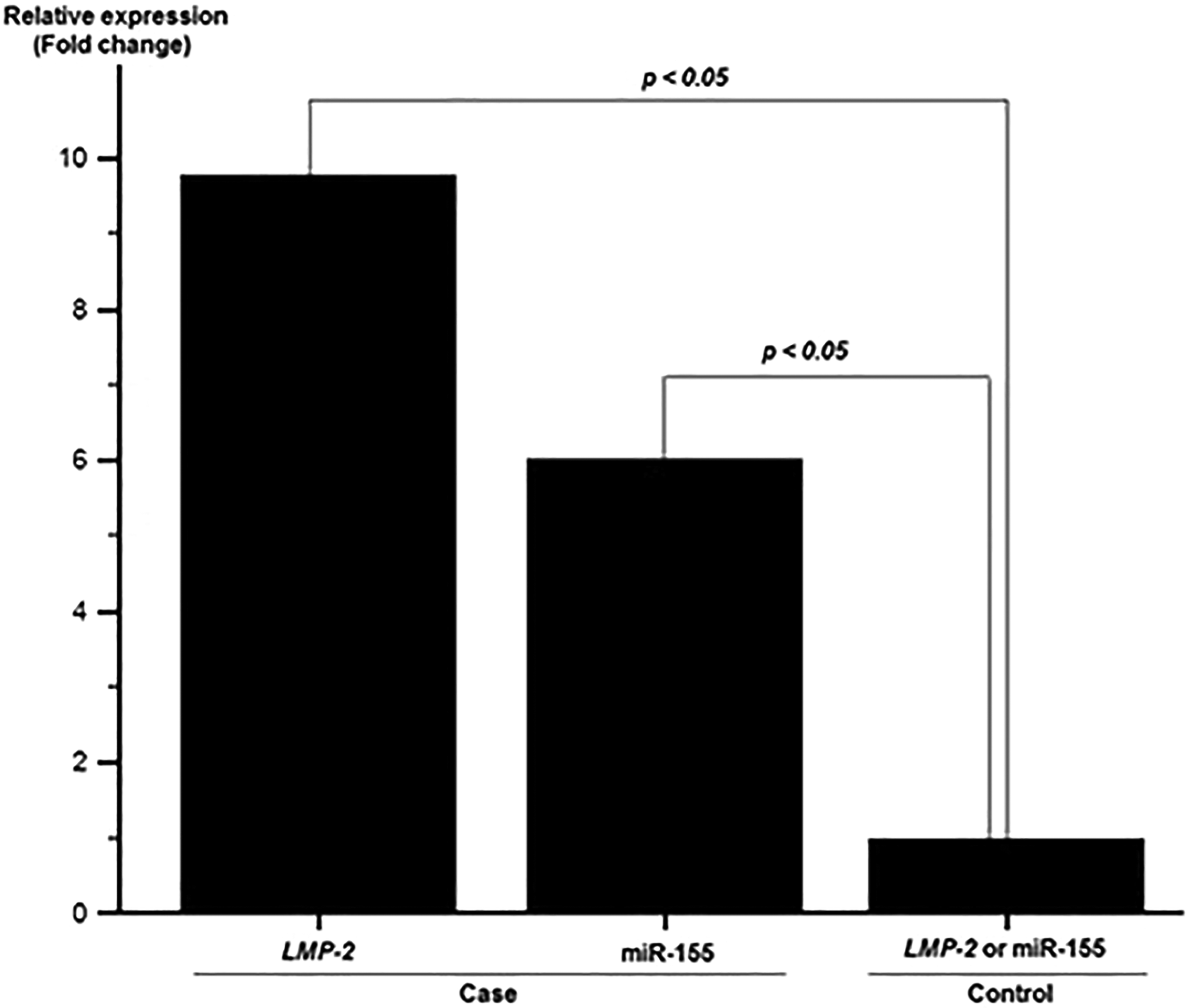
The upregulation of LMP-2 and miR-155 in nasopharyngeal carcinoma biopsy samples compared with noncancerous samples.
miR-155 expression in NPC samples
cDNA U6 (UniSp6 rRNA, abbreviated U6), which was used as an endogenous control for the assessment of miR-155 expression in the current study, was positive in both case and control groups. The Ct values of U6 were 29.41 ± 1.51 and 30.11 ± 1.61 in the case and control groups, respectively. The p value (p = 0.53) indicated no significant difference in the expression of U6 between the two groups (Fig. 4). Therefore, U6 was used as a reference gene (internal control) to normalize miR-155 expression in the comparison between the NPC group (case group) and the noncancerous group (control group). In the current study, the expression of miR-155 in both NPC biopsy samples and noncancerous samples was detected by real-time RT-PCR. As shown in Table 2, the proportion of positive and negative cases in NPC samples was 75.27% (70 of 93 cases) and 24.73% (23 of 93 cases), respectively. In the noncancerous group, the positive and negative rates were 35.0% (35 of 100 cases) and 65.0% (65 of 100 cases), respectively. A p value (p < 0.0001) showed the significantly higher correlation between the miR-155 and NPC (Fig. 4). Based on the proportion of miR-155 detection, the OR and RR values were computed between the expressions of miR-155 and NPC. The results show that the OR and RR values were 5.65 (95% CI = 3.03-10.56, p < 0.0001) and 2.55 (95% CI = 1.75-3.72, p < 0.0001), respectively. The mean Ct values of miR-155 in the case and control groups were 26.08 and 29.37, respectively. The relative quantification of miR-155 expression in the case and control groups was analyzed by the 2−ΔΔCt method. The result showed that the expression of miR-155 was 6.02 times higher in tumor samples in comparison with the noncancerous samples (p < 0.05) (Fig. 3). No significant association was found between LMP-1 and LMP-2 expression and other clinical characteristics, such as patient's gender (p = 0.71), age (p = 0.16), tumor histological types (p = 0.49), as well as stage (p = 0.84).

The mean Ct value (mean ± SE) of U6 and miR-155 expression in the case group and control group. Each black dot indicated the Ct value of each sample. The red dots indicate the mean of Ct. Color images are available online.
Association between LMP-1 and LMP-2 expression and miR-155 expression
The chi-square test was applied to evaluate the association between LMP-1 and LMP-2 expression and miR-155 expression, as shown in Table 3. As shown, in the 70 NPC tissue samples that were miR-155 positive, 61 samples (accounting for 65.59%) were LMP-1 positive, 54 samples (accounting for 58.07%) were LMP-2 positive, and 63 samples (accounting for 67.74%) were either LMP-1 or LMP-2 positive (real-time-PCR index [RPI] ≥0.5). The p value indicated that miR-155 expression in LMP gene was positively significantly associated with the subject with LMP negative. Therefore, miR-155 was upregulated in NPC samples with LMP positive compared with the NPC samples with LMP negative.
Statistical Analysis of Association Between miR-155 Expression and LMP-1 and LMP-2 Expression in Nasopharyngeal Carcinoma Samples
RPI, real-time polymerase chain reaction index.
Discussion
NPC, a prevalent malignant tumor of the nasopharynx, is remarkably characterized by its distinctive geographic and ethnic distribution, occurring with high frequencies in Southeast Asian countries, including Vietnam. Presently, NPC is challenging to diagnose because the tumors typically arise from the mucosal epithelium of the nasopharynx. Moreover, most of the NPC remains clinically silent for a long period of time, especially in patients with vague symptoms, such as hearing loss, bloody nasal discharge, diplopia, and headache. Therefore, most patients are first diagnosed at an advanced stage (stage 3 or 4) (Lee et al., 1992; Hao et al., 2004; Lee and Ho, 2012; Wang et al., 2017). It is essential to find a biomarker that achieves early diagnosis to achieve favorable treatment and increase patient survival.
Many previous studies have demonstrated that multiple etiological factors, including EBV infection, genetics/or genetic susceptibility, and environmental factors, are strongly linked with NPC risk (Hildesheim and Levine, 1993; Kumar and Mahanta, 1998; Lao et al., 2017; Wu et al., 2018). Because of the close association between EBV infection and NPC tumorigenesis, it may throw light on the development of EBV-based molecular screening, diagnosis, and prognosis for NPC in high-incidence areas, including Vietnam. In the latent stage of EBV, EBV genome expresses EBV-encoded nuclear antigens, LMPs, EBV-encoded small RNA, and nontranscribed BamHI-A region rightward transcripts. Among them, LMP-1 and LMP-2 expressions, which are expressed in EBV latency type II, exemplified by NPC, contribute to cell survival by activation of NK-κB and PI3K signaling pathways (Xu et al., 2006; Kang and Kieff, 2015). LMP-1 is the key viral protein that functions as a viral mimic of a TNFR family member, CD40, engaging in a number of signaling pathways, such as NF-κB, JNK, and p38 pathways (Hao et al., 2004; Xu et al., 2006; Dawson et al., 2012; Kang and Kieff, 2015). LMP-2 plays an important role in carcinogenesis by driving EBV into latency and providing essential survival signals through the constitutive activation of the extracellular-signal-regulated kinase/mitogen activated protein kinase pathway (Thompson and Kurzrock, 2004; Dawson et al., 2012). Thus, LMP-1 and LMP-2 are thought to be meaningful biomarkers for NPC management. In the current study, a case/control study was carried out to evaluate whether or not LMP-1 and LMP-2 could be further applied in NPC screening, diagnosis, as well as therapy. The result pointed out the significantly high expression of LMP-1 and LMP-2 in NPC clinical samples, 76.34% and 67.74%, respectively. Whereas in the control group, no LMP-1 expression was observed, and only 1 of 100 specimens was detected with LMP-2 positive (p < 0.0001). In addition, the LMP-2 expression was confirmed to be 9.78 times higher in tumor samples compared with noncancerous samples (2−ΔΔCt = 9.78, p < 0.05). LMP-1 was not detected in the control group, but it was confirmed that the expression of LMP-1 was elevated in patient samples. The increased expression of LMP-1 and LMP-2 was strongly associated with NPC risk, with statistical significance, based on the calculated RR and OR (p < 0.05). It indicated that the NPC risk associated with the expression of LMP-1 and LMP-2 was 4.76 and 4.74 times higher than the NPC risk without LMP-1 and LMP-2 expression, respectively. Thus, all these results imply that the oncogenic role of LMP-1 and LMP-2 in NPC was well evaluated in this case/control group study.
As described above, NPC is difficult to diagnose and screen, especially in the early stage, by clinical symptoms as well as histological evaluation. Molecular biomarkers may be considered the ideal NPC detection tools. Besides the EBV infection, numerous studies have demonstrated that miRNAs, associated with the pathogenesis of NPC, are novel markers with an impact on cancer (Lu et al., 2005; Higgs and Slack, 2013; Hou et al., 2016). In the current case/control study, the expression of miR-155 was determined by real-time RT-PCR. Based on the result, a higher expression of miR-155 was clearly shown in the clinical NPC sample group, with the positive result of miR-155 being 75.27% (sensitivity = 75.27%), compared with the noncancerous group. It indicated that 75.27% of the NPC biopsy samples were positive for miR-155 expression (p < 0.0001). In addition, the upregulation of miR-155 was strongly correlated with NPC risk, and the results were significant on the basis of RR and OR, accounting for 2.55 (95% CI = 1.75-3.72, p < 0.0001) and 5.65 (95% CI = 3.03-10.56, p < 0.0001), respectively. It is noteworthy that the overexpression of miR-155 was once confirmed to be 6.02 times higher in tumor samples in comparison with the noncancerous samples (2−ΔΔCt = 6.02). Therefore, we investigated the potential differential expression of miR-155 in NPC biopsy samples and noncancerous nasopharyngeal swabs. According to a previous study by Chen et al. (2009), miR-155 was significantly upregulated in NPC samples. Also, the relative expression level of miR-155 observed in our study (about 6.02 times) was similar to that obtained in the report of Chen et al. (2009) (about 6.04 times). Moreover, miR-155 was also reported as an onco-miR in NPC tumorigenesis by regulating NPC cell proliferation, differentiation, and apoptosis (Zhu et al., 2013; Tan et al., 2015). To our knowledge, there is no previous literature evaluating the differential miR-155 expression between clinical NPC samples and noncancerous specimens. Therefore, this study is considered the first case/control study to determine whether or not an association between LMP-1 and LMP-2 expression and miR-155 expression was observed in Vietnamese NPC patients. In agreement with the findings from previous studies, we found that miR-155 is upregulated and has an oncogenic role in NPC development. Notably, in the current study, tumor biopsy samples were used, as they provide direct information with regard to the tumor biology. However, based on current trends in the development of biomarkers for diagnoses and prognoses, future studies should be designed to look at the values of these molecular markers in both circulating tumor cells and circulating tumor DNA.
Recent studies have shown that the dysregulated miRNA expression, such as miR-10b, 18b, and 34a post-EBV infection in human cancers, includes NPC (Li et al., 2010; Forte et al., 2012; Luo et al., 2013). According to miR-155, our results successfully demonstrated that there was a significant association between LMP-1 and LMP-2 expression and miR-155 expression in NPC clinical samples. In this study, 70 NPC samples were positive for miR-155 expression. Of these, 61 of the 70 samples (accounting for 87.14%), 54 of the 70 samples (accounting for 77.14%), and 63 of the 70 samples (accounting for 90.00%) were, respectively, positive for LMP-1, LMP-2, and either LMP-1 or LMP-2 (RPI ≥0.5). The result indicates that there is a significant tendency of LMP-1 and LMP-2 expression in subjects with miR-155 expression in Vietnamese NPC patients (p < 0.05). These results were similar to a previous study, reported by Zhu et al., that an upregulated miR-155 was detected in EBV-positive NPC tissue samples and was correlated with LMP1 DNA copies. In their study, a higher expression of miR-155 was clearly shown in the comparison between LMP-negative and NPC tissue specimens. In addition, the upexpression of miR-155 was also confirmed in an in vitro study, which stated that the miR-155 expression was significantly induced in the LMP-1-transfected cell line (Zhu et al., 2013). In another study, the regulation of miR-155 also confirmed that its upregulation is partly driven by LMP-1 and LMP-2, and results in downregulation of JMJD1A gene, and consequently increased NPC tumorigenesis (Du et al., 2011). The expression of miR-155 induced by EBV LMP-1 through the NF-κB has been reported in a previous study (Gatto et al., 2008). The underlying mechanism details for the regulatory effects of miR-155 and LMP-1, as well as LMP-1 on the progression of NPC, are needed for more evaluation in in vitro and in vivo studies. Taken together, our investigations reveal that the expressions of miR-155 are upregulated in NPC clinical samples, with an association with LMP-1 and LMP-2 expressions; therefore, they were identified as promising biomarkers for NPC.
Conclusion
In conclusion, the frequencies of LMP-1, LMP-2, and miR-155 were 76.34%, 67.74%, and 75.27% in NPC samples, respectively. In addition, a significant association between LMP-1 and LMP-2 expression and miR-155 expression in NPC clinical samples was demonstrated. This approach may facilitate the development of promising biomarkers for the diagnosis and therapy of NPC based on LMPs and miR-155 expression. For future study, it is necessary to improve the invasion method in NPC diagnosis in Vietnamese NPC patients.
Footnotes
Acknowledgments
We wish to express our thanks to the research project sponsored by Ho Chi Minh City Open University. We thank all the recruited participants in this work. We also express our gratitude to Dr. Nguyen Trong Minh, Dr. Nguyen Huu Dung, and all the staff members of Otorhinolaryngology in Cho Ray Hospital, Ho Chi Minh City, for collecting the samples used in these studies. We are thankful to the participants in our study and appreciate the contributions of the staff from Molecular Biology Laboratory, Ho Chi Minh City Open University.
Ethical Approval and Consent
All patients signed informed consent before entering into the study. No study drug or procedure was applied. This is an observational study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Ministry of Education and Training, Ha Noi, Vietnam (Grant No. B2017-MBS-05), Ho Chi Minh City Department of Science and Technology, Ho Chi Minh City, Vietnam (Grant No. 42/2017/HD-SKHCN), and Ho Chi Minh City Open University, Ho Chi Minh City, Vietnam (Grant No. E2016.2.2.1).