
Abstract
Objective:
We aimed to study the relationship between single nucleotide polymorphisms (SNPs) in the 3′-untranslated region of the nuclear factor-kappaB (NF-κB) gene NFKB1 and the risk of acute kidney injury (AKI) in sepsis.
Methods:
The genotypes of the NFKB1 gene loci rs41275743 and rs4648143 were obtained by Sanger sequencing from 235 AKI patients and 235 non-AKI patients (No AKI). The plasma levels of Homo sapiens (human) microRNAs (hsa-miR)-580, hsa-miR-671-3p, hsa-miR-886-5p, hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 were determined by quantitative real-time polymerase chain reaction. The P50 protein in lymphocytes and the levels of tumor necrosis factor alpha (TNF-α), serum creatinine (SCr), cystatin (Cys)-C, and kidney injury molecule (KIM)-1 in plasma were detected by enzyme-linked immunosorbent assays.
Results:
The risk of AKI in patients with sepsis in A-allele carriers of the NFKB1 gene rs41275743 locus was 1.46 times higher than that of the G-allele carriers. The risk of AKI in patients with sepsis in A-allele carriers of the NFKB1 gene rs4648143 locus was 1.56 times higher than that of the G-allele carriers. Acute Physiology and Chronic Health Evaluation (APACHE) III score, Simplified Acute Physiological Score (SAPS) II, Sequential Organ Failure Assessment (SOFA), rs41275743, and rs4648143 were all independent risk factors for AKI. The plasma levels of P50 protein, TNF-α, SCr, Cys-C, and KIM-1 from patients with sepsis carrying the rs11475743 GG and rs4648143 GG genotypes were significantly lower than in those carrying the A-alleles (GA/AA). The levels of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p in the plasma of patients carrying the rs41275743 GA/AA genotypes were significantly lower than in those with the GG genotype, whereas the levels of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 showed no significant difference in patients with different genotypes of the rs41275743 locus. The levels of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 in the plasma of patients carrying the GA/AA genotype of the rs4648143 locus were significantly lower than in those with the GG genotype, whereas the levels of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p did not change significantly in patients carrying different genotypes at the rs4648143 locus.
Conclusion:
SNPs in the NFKB1 gene loci rs41275743 and rs4648143 are associated with the risk of AKI in patients with sepsis.
Introduction
Sepsis is a life-threatening failure of multiple organs caused by dysfunctional responses to infection, and it is the leading cause of death in intensive care units (ICUs) (Rhodes et al., 2017). Sepsis can be caused by a variety of pathogens, with severe cases resulting in multiple organ dysfunction syndrome and multiple organ failures (Rossaint and Zarbock, 2015; Misheva et al., 2018). In such cases, the kidney is one of the most commonly involved organs, and acute kidney injury (AKI) is often an independent risk factor for predicting death in patients with sepsis (Muller et al., 2012; Shibahashi et al., 2017).
The nuclear factor-kappaB (NF-κB) signaling pathway exists widely in eukaryotic cells and is able to bind to the specific binding sites of multiple gene promoter regions or enhancer regions (Hayden and Ghosh, 2014), promoting transcriptions of the downstream genes (Shih et al., 2015), and participating in inflammatory responses, immune responses, cell proliferation, differentiation, apoptosis, and tumorigenesis (Wang et al., 2009; Tong et al., 2015; Yang et al., 2015). NF-κB regulates the expression of many immune-related genes, such as the gene for tumor necrosis factor alpha (TNF-α), which is closely related to the occurrence of sepsis (Wu et al., 2015; Markó et al., 2016). The NF-κB transcription factor family plays a key role in the induction and regulation of inflammation through classical and alternative pathways under many pathological conditions (Xiao et al., 2001; Liang et al., 2006).
The NFKB1 gene encodes the P50 protein, which is located on the 4q23-q24 chromosome, and polymorphisms of this gene are associated with the occurrence of various diseases. For instance, ATTG insertion/deletion polymorphism in the promoter at the 94 locus (-94ins/del ATTG, rs28362491) affects the expression of P50 and changes the level of inflammatory responses (Tek et al., 2016; Yin et al., 2016). The NFKB1 promoter polymorphism (-94ins/delATTG) alters the nuclear translocation of NF-κB1 in monocytes after lipopolysaccharide stimulation and is associated with increased mortality in sepsis (Adamzik et al., 2013). Hydrocortisone fails to abolish the nuclear translocation of NF-κB1 protein in deletion-allele carriers of the polymorphism in NFKB1 promoter (-94ins/delATTG), and the occurrence of this polymorphism is associated with increased 30-day mortality in septic shock (Schäfer et al., 2014).
In this study, we selected the single nucleotide polymorphism (SNP) loci corresponding to the microRNA (miRNA)-binding sites in the 3′-untranslated region (UTR) of the NFKB1 gene, namely, rs41275743 and rs4648143. A case-control study was conducted to analyze the correlation of these miRNA-binding site SNPs and the risk of AKI in sepsis.
Materials and Methods
Subjects
This study was conducted from August 2016 to February 2019. We recruited 530 patients with septic shock from the First People's Hospital of Yuhang District, Hangzhou and the Tiantai Hospital of Hangzhou Medical College. The diagnosis of septic shock was based on the Third International Consensus Definitions for Sepsis and Septic Shock (Seymour et al., 2016). The age of all patients with septic shock was >18 years. The exclusion criteria were as follows: patients with end-stage renal disease receiving chronic dialysis, patients with diffuse alveolar hemorrhage, patients with chronic lung diseases without asthma and chronic obstructive pulmonary disease, patients with immune inhibition who did not continue to use corticosteroids and were treated with granulocyte colony-stimulating factors, and direction to withhold intubation. The patients' Acute Physiology and Chronic Health Evaluation (APACHE) III scores and basal characteristics were recorded on the day of ICU admission. The diagnostic criteria for AKI were based on the standard definitions of the AKI Network (Mehta et al., 2007); the patient was diagnosed as suffering from AKI if his/her serum creatinine (SCr) increased by ≥0.3 mg/dL or the percentage increase was ≥50% within the first 72 h of ICU admission. Among the 530 patients with septic shock, 32 patients were excluded because of chronic dialysis, and 23 patients were excluded because of lack of data on creatinine. Among them, 235 patients with AKI were defined as the AKI group, and 235 patients without AKI were included in the No AKI group in a 1:1 ratio, and the remaining 5 patients without AKI were excluded. This study was approved by the Ethics Committee of the First People's Hospital of Yuhang District, Hangzhou and the Tiantai Hospital of Hangzhou Medical College. The recruitment procedure was conducted in accordance with the World Medical Association Declaration of Helsinki and all participants in this study signed informed consents.
Genotyping analysis
Blood was obtained from all patients within 48 h after admission to the ICU for DNA extraction. Genomic DNA was extracted using the QIAamp DNA Blood Mini Kit (Qiagen, Inc., Valencia, CA) and stored in a refrigerator at −80°C. The polymerase chain reaction (PCR) primers for the NFKB1 gene rs41275743 locus were as follows: 5′-TGT CCA CAA GAC AGA AGC TGA-3′ (forward); 5′-TCG AGA ATG ATT CAG GCG GG-3′ (reverse). The PCR primers for the NFKB1 gene rs4648143 locus were as follows: 5′-TAG CCT GCT GAC AAT TTC CCA-3′ (forward); 5′-TGT CTT GTG GAC AAC GCA GT-3′ (reverse). The PCR system had the following in a volume of 20 μL: 50 ng extracted genomic DNA, 1.5 μL of 25 mM Mg2+, 2 μL of 10 × PCR buffer, 1 μL of 10 μM deoxynucleoside triphosphate, 1 μL of 10 pM forward and reverse primers, and 0.25 μL of DNA polymerase; the reaction mix was supplemented with sterile water to the final volume. The PCR conditions were as follows: 95°C, 5 min; 94°C, 20 s; 56°C, 30 s; and 72°C, 30 s for 35 cycles; and finally 72°C, 5 min. The PCR products were purified and sequenced by the Sanger sequencing method, and the sequencing results were compared with the sequences in the NCBI SNP database to determine the genotype.
Quantitative real-time PCR
Total RNA was isolated from plasma using TRIzol reagent (Invitrogen, Carlsbad, CA) according to the manufacturer's instructions. The extracted RNA was reverse transcribed into complementary DNA using PrimeScript RT Master Mix (TaKaRa, Dalian, China). Subsequently, quantitative real-time polymerase chain reaction (qRT-PCR) was performed using the PrimeScript RT Kit and SYBR Premix Ex Taq (TaKaRa); the miRNA primers were synthesized by RiboBio (Guangzhou, China) (Table 1), and glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was used as an internal control. The PCR conditions were as follows: 95°C, 30 s; 95°C, 5 s; and 60°C, 34 s for 40 cycles. The qRT-PCR was performed on an ABI 7500 real-time PCR system (Applied Biosystems, Foster City, CA), and the fold change in expression of miRNAs relative to GAPDH was calculated using the 2−ΔΔCT method.
micro RNA Primer Information
GAPDH, glyceraldehyde 3-phosphate dehydrogenase; miRNA, microRNA.
Enzyme-linked immunosorbent assay
Five milliliters of venous blood was obtained from all patients; after standing for 30 min, this was centrifuged at 3000 r/min for 20 min, and then the supernatant was retrieved and stored in a refrigerator at −80°C. Lymphocytes were isolated using human lymphocyte separation solution (catalog no. P8610; Solarbio Life Sciences) according to the supplier's instructions, and the P50 protein was extracted from the isolated lymphocytes. The levels of TNF-α, SCr, cystatin (Cys)-C, kidney injury molecule (KIM)-1, and P50 protein in the lymphocytes were determined by enzyme-linked immunosorbent assay (ELISA). The TNF-α detection kit was E-EL-H0109c (Elabscience, Wuhan, China), Cys-C detection kit was E-EL-H3643c (Elabscience,), KIM-1 detection kit was E-EL-H0186c (Elabscience), and the SCr detection kit was E-EL-0058c (Elabscience).
Statistical analyses
Statistical analyses in this study were performed using SPSS Version 22.0 (IBM Corp., Armonk, NY). The continuous variables were expressed as mean ± standard deviation, and statistical analyses were performed using an independent t-test. The categorical variables were expressed as percentages [n (%)], and statistical analyses were performed using the chi-squared test. The association of the NFKB1 gene SNPs with the risk of AKI was determined based on the distribution of allele frequencies and genetic models (additive, dominant, and recessive models); odds ratios (ORs) and 95% confidence intervals (CIs) were used in an unconditional logistic regression analysis, adjusted to age, gender, and body mass index (BMI). All tests were two tailed, and p < 0.05 was considered to be statistically significant.
Results
General clinical characteristics of the participants
In this study, a total of 530 patients with septic shock were selected; 32 patients among these were excluded due to chronic dialysis, and 23 patients were excluded because of lack of data on creatinine. Thus, 235 patients with AKI were defined as the AKI group, another 235 patients without AKI were selected as the No AKI group in a 1:1 ratio to the case group, and the remaining 5 patients without AKI were finally excluded. The general clinical characteristics of the AKI group and the No AKI group are presented in Table 2. No significant difference in age, BMI, gender, source of infection, and type of infectious pathogen was detected between the AKI group and No AKI group (p > 0.05). However, the APACHE III score, the Simplified Acute Physiological Score (SAPS) II, and Sequential Organ Failure Assessment (SOFA) score of patients with AKI were significantly higher than the scores of those without AKI (p < 0.001).
Comparison of the General Clinical Characteristics of the Acute Kidney Injury Group and the No Acute Kidney Injury Group
AKI, acute kidney injury; APACHE, Acute Physiology and Chronic Health Evaluation; BMI, body mass index; SAPS, Simplified Acute Physiological Score; SOFA, Sequential Organ Failure Assessment.
SNP in the 3′-region of the NFKB1 gene was associated with AKI
We analyzed the association of different genotypes and alleles of the NFKB1 gene at the rs41275743 and rs4648143 loci with the risk of AKI. The results showed that the risk of AKI in patients with GA and AA genotypes was increased compared with the risk with the GG genotype at the rs41275743 locus (adjusted OR = 1.35, 95% CI: 1.07-1.63, p = 0.01; adjusted OR = 1.94, 95% CI: 1.35-2.18, p < 0.01; respectively). The risk of AKI was significantly increased in both the dominant and recessive models (adjusted OR = 1.45, 95% CI: 1.18-1.71, p < 0.01; adjusted OR = 1.82, 95% CI: 1.27-2.03, p < 0.01; respectively), but not in the additive model (adjusted OR = 1.10, 95% CI: 0.95-1.28, p = 0.22). The risk of occurrence of AKI in patients with sepsis was 1.46 times higher in subjects carrying the A allele at the rs41275743 locus than in the G allele carriers (95% CI: 1.25-1.66, p < 0.01) (Table 3).
Association of Different Genotypes and Alleles at the rs41275743 and rs4648143 Loci of the NFKB1 Gene with the Risk of Acute Kidney Injury
Adjusted to age, gender, and BMI.
CI, confidence interval; NF-κB, nuclear factor-kappaB; OR, odds ratio.
In addition, the risk of AKI in patients with sepsis was significantly higher in the GA and AA genotypes compared with the risk with the GG genotype at the rs4648143 locus (adjusted OR = 1.53, 95% CI: 1.23-1.82, p < 0.01; adjusted OR = 1.90, 95% CI: 1.23-2.19, p = 0.01; respectively). The risk of AKI was significantly increased in both the dominant and recessive models (adjusted OR = 1.59, 95% CI: 1.31-1.86, p < 0.01; adjusted OR = 1.75, 95% CI: 1.14-2.01, p = 0.02; respectively), but not in the additive model (adjusted OR = 1.11, 95% CI: 0.96-1.29, p = 0.17). The risk of occurrence of AKI in patients with sepsis was 1.56 times higher in the A allele carriers of the rs4648143 locus than in the G allele carriers (95% CI: 1.33-1.76, p < 0.01) (Table 3).
Stratified analysis
We divided patients with sepsis into the following groups: young patients (age <60 years) and elderly patients (age ≥60 years); nonobese patients (BMI <24 kg/m2) and obese patients (BMI ≥24 kg/m2); or men and women, and analyzed the data for the association of NFKB1 gene SNPs with a risk of AKI in different stratifications. The results showed that patients with sepsis of different ages, BMI values, and gender had a significantly higher risk of AKI (p < 0.05) when carrying the A allele (GA/AA) of the NFKB1 gene rs41275743 and rs4648143 loci (Tables 4 and 5).
Stratified Analysis of the Relationship Between Different Genotypes and Alleles at the rs41275743 Locus of the NFKB1 Gene and the Risk of Acute Kidney Injury
Adjusted to age, gender, and BMI.
Stratified Analysis of the Relationship Between Different Genotypes and Alleles at the rs4648143 Locus of the NFKB1 Gene and the Risk of Acute Kidney Injury
Adjusted to age, gender, and BMI.
Multifactor dimensionality reduction analysis of the interaction between NFKB1 gene SNPs at the rs41275743 and rs4648143 loci and environmental factors
We then used multifactor dimensionality reduction (MDR) to analyze the interaction between NFKB1 gene rs41275743 and rs4648143 SNPs and the factors age, sex, and BMI. The results showed that there was a strong interaction between BMI and rs4648143 SNP, followed by the rs41275743 SNP (Fig. 1).
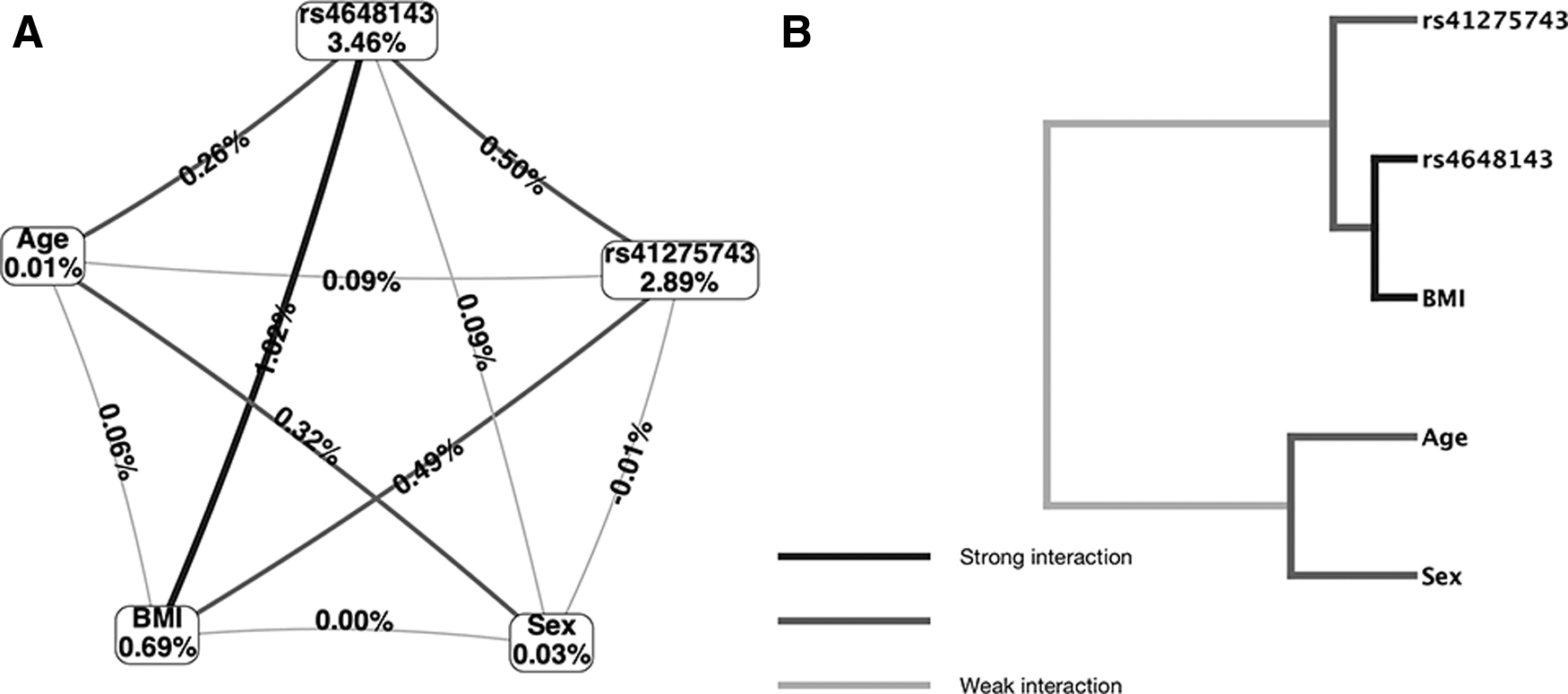
MDR analysis of the interaction between NFKB1 gene SNPs and age, gender, and BMI.
Multivariate logistic regression analysis
We performed multivariate logistic regression analysis, and the result showed that APACHE III score, SAPS II, SOFA, rs41275743, and rs4648143 were independent risk factors for AKI (p < 0.05, Table 6).
Multivariate Logistic Regression Analysis for Identifying Risk Factors of Acute Kidney Injury
Kidney injury-related factors
We compared the kidney injury-related factors of the patients with AKI and those with No AKI. The results showed that the level of P50 protein in the lymphocytes of patients with AKI was significantly higher than that in the No AKI patients (p < 0.01, Fig. 2A). Moreover, the levels of TNF-α, SCr, Cys-C, and KIM-1 in the plasma of patients with AKI were significantly higher than the levels in No AKI patients (p < 0.05; Fig. 2B-E).
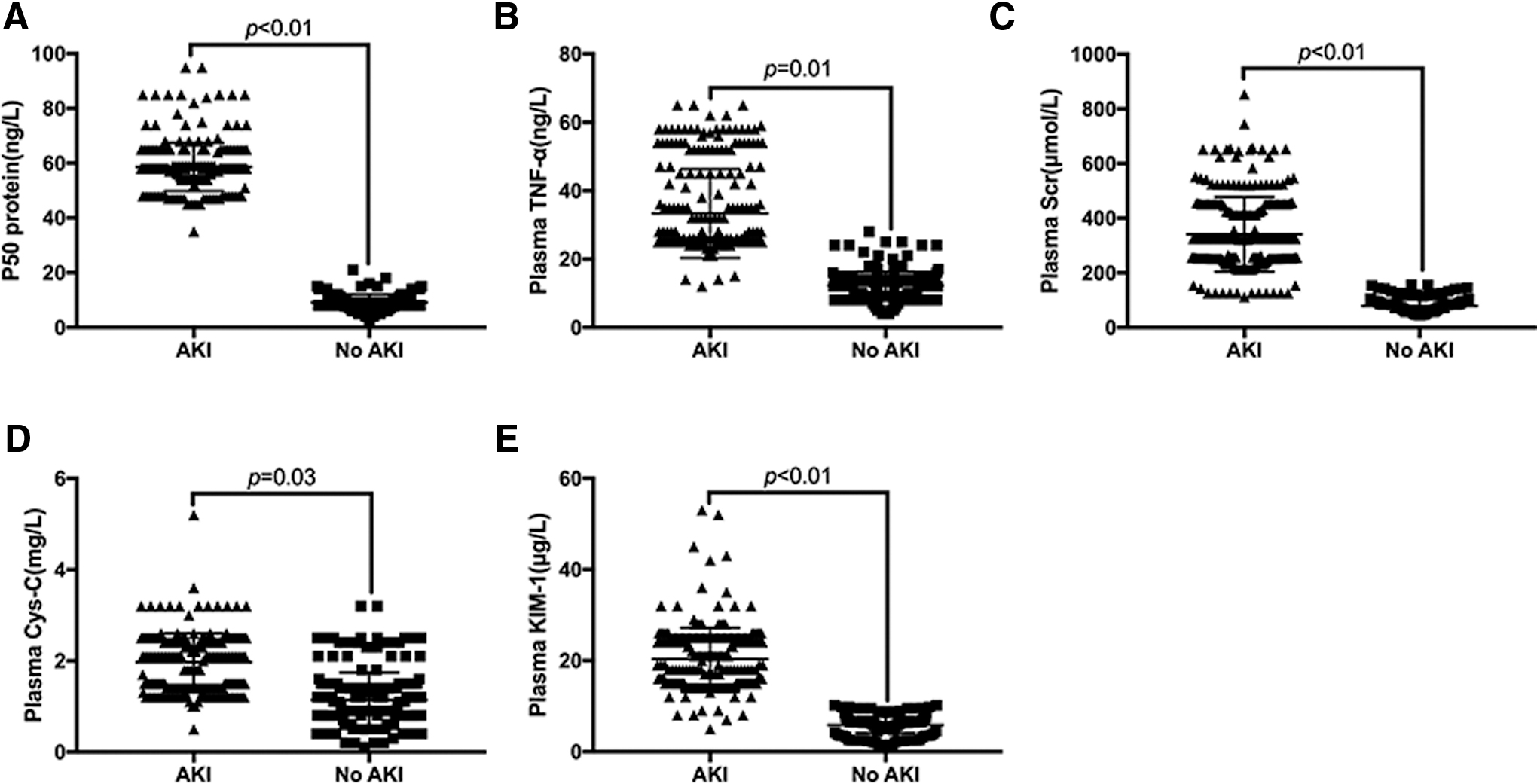
Comparison of kidney injury-related factors between patients with AKI and No AKI.
Correlation between SNPs in the 3′-UTR of the NFKB1 gene and the kidney injury-related factors
We analyzed the association of the NFKB1 gene SNPs rs41275743 and rs4648143 with the levels of P50, TNF-α, SCr, Cys-C, and KIM-1 in patients with AKI and No AKI. The results showed that the levels of P50 protein in lymphocytes, as well as of TNF-α, SCr, Cys-C, and KIM-1 in the plasma of patients with AKI and No AKI subjects with the GG genotype at the rs4648143 and rs41275743 loci were significantly lower than in those with the A allele (GA/AA) (p < 0.05) (Figs. 3 and 4).
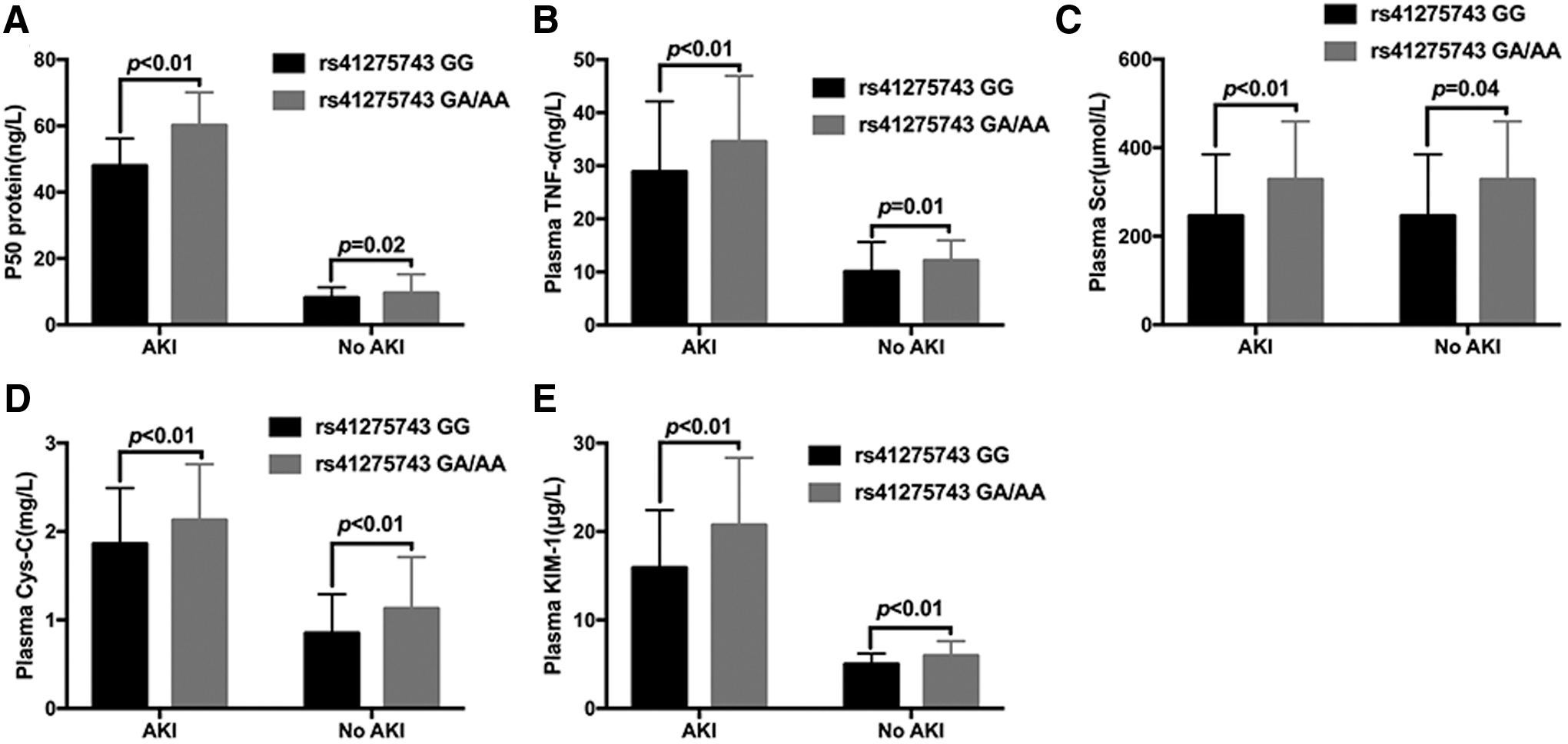
Correlation between the NFKB1 gene rs41275743 SNP and kidney injury-related factors.

Correlation between the NFKB1 gene rs4648143 SNP and kidney injury-related factors.
Comparison of plasma levels of miRNAs between AKI patients and No AKI patients
To detect the plasma levels of Homo sapiens (human) miRNA (hsa-miR)-580, hsa-miR-671-3p, hsa-miR-886-5p, hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9, we conducted qRT-PCR, and the results showed that plasma levels of hsa-miR-580, hsa-miR-671-3p, hsa-miR-886-5p, hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 in the AKI patients were significantly lower than the levels in No AKI patients (p < 0.05) (Fig. 5).
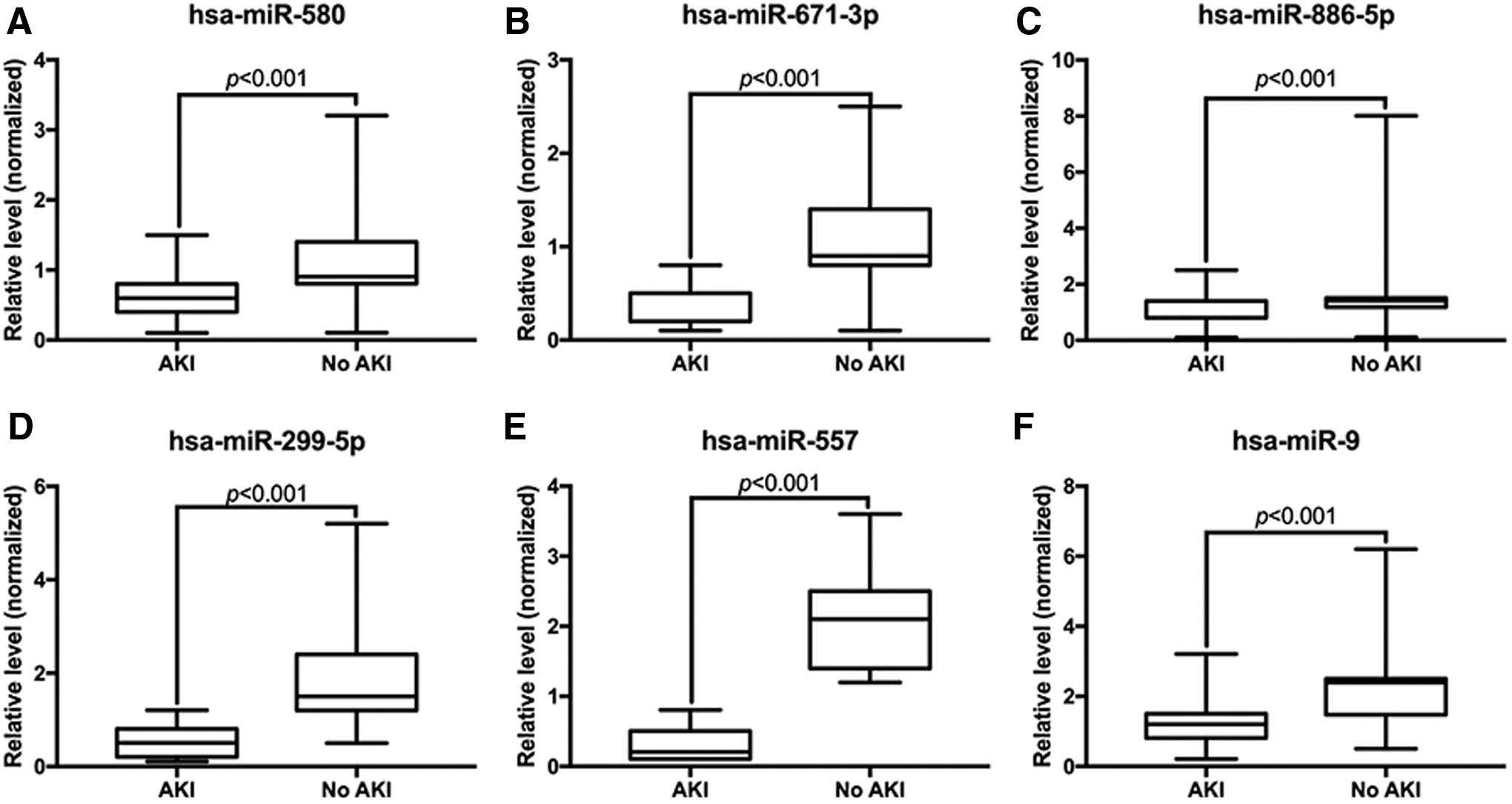
Comparison of plasma miRNAs in patients with AKI and No AKI.
Correlation between SNPs in the 3′-UTR of the NFKB1 gene and plasma miRNAs
The plasma levels of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p in patients with AKI and No AKI carrying the rs41275743 locus GA/AA genotype were significantly lower than the levels in patients/subjects with the GG genotype (p < 0.05); however, the plasma levels of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 were not statistically different among patients with different genotypes at the rs41275743 locus (p > 0.05) (Fig. 6A). The plasma levels of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 in patients with AKI and No AKI carrying the rs4648143 GA/AA genotype were significantly lower than the levels in those with the GG genotype (p < 0.05). However, there was no significant difference in the plasma levels of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p among patients with different genotypes at the rs4648143 locus (p > 0.05) (Fig. 6C, D).
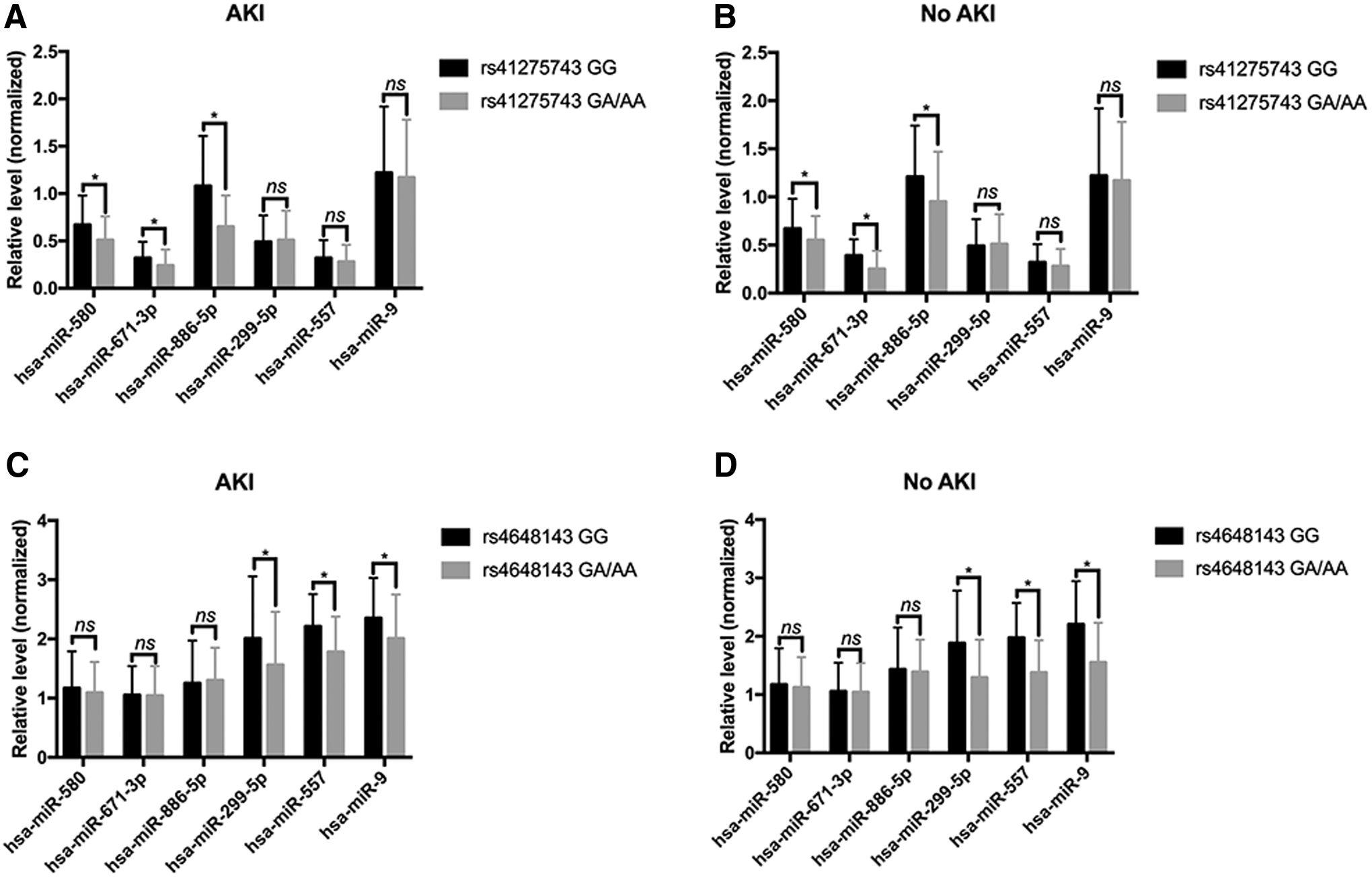
Association of NFKB1 gene SNPs at rs41275743 and rs44648143 loci with plasma levels of miRNAs.
Discussion
In this study, we analyzed the genotypes of the NFKB1 gene rs41275743 and rs4648143 loci in 235 patients with AKI and 235 No AKI patients by a case-control study. We found that the A-alleles of the NFKB1 gene rs41275743 and rs4648143 loci were high-risk factors for AKI in patients with sepsis (p < 0.05). The expression of P50 protein in lymphocytes and the levels of TNF-α, SCr, Cys-C, and KIM-1 in the plasma were abnormally elevated in patients carrying the A-allele, and the levels of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p in the plasma of the rs41275743 A-allele carriers were significantly lower than the levels in the G-allele carriers, whereas the levels of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 in the plasma of the rs4648143 A-allele carriers were significantly lower than the levels in the G-allele carriers. These findings indicate that the presence of the A-allele of the NFKB1 gene at the rs41275743 and rs4648143 loci is a risk factor for AKI in patients with sepsis.
Sepsis is a common and serious disease for the patients in the ICU. It results in the rapid deterioration of the disease if the treatment is not timely; leads to multiple organ dysfunction syndrome, multiple organ failures, and other serious complications; and eventually threatens the patient's life (Polat et al., 2017; Rhodes et al., 2017). Recent studies have revealed that the organ damage caused by sepsis is not directly due to bacteria or other infectious microorganisms; rather, it is mainly due to the disorder of nonspecific inflammatory responses of the body, including the abnormal expression of inflammatory factors that damage multiple organs of the body (Hattori et al., 2016; Buendgens et al., 2017). A previous study has found that the clinical mortality rate of AKI caused by sepsis reaches up to 70%, and the mortality rate is significantly higher than that caused by other factors (Lameire et al., 2005). The possible reason is that sepsis directly damages the kidney by the increase of endotoxin and inflammatory mediators in the blood and triggers the coagulation and fibrinolysis system, which causes thrombosis in the glomeruli and blocks the renal microvasculature (Bagshaw et al., 2008; Doi et al., 2009). Additionally, the vascular bed of the renal blood vessel itself is different from that of other blood vessels, and the response to the contractile substance is enhanced under sepsis, which aggravates the renal blood flow and decreases the glomerular filtration rate (Yasuda et al., 2006; Lopes et al., 2009).
In the present study, we selected the rs41275743 and rs4648143 loci in the 3′-UTR of the NFKB1 gene. The reason for selecting these two SNP loci was predicted by the TargetScan tool, which revealed that these two loci are located at the binding sites of miRNAs to NFKB1 mRNA; thereafter, we speculated that these SNPs may affect the regulation of expression of the NFKB1 gene by miRNAs. Multivariate logistic regression analysis results showed that rs41275743 and rs4648143 SNP were independent risk factors for AKI. The results of this study show that the A-alleles of the NFKB1 gene at the rs41275743 and rs4648143 loci are high-risk factors for AKI in patients with sepsis. The possible reason is that SNPs at the rs41275743 and rs4648143 loci affect the expression level of the NFKB1 gene. Further studies showed that the expression level of the P50 protein in the lymphocytes of patients with the A-alleles at the rs41275743 and rs4648143 loci in the NFKB1 gene was significantly higher than that in the G-allele carriers. In addition, the levels of the kidney injury-related factors in the plasma of A-allele carriers were significantly higher than the levels in the G-allele carriers, indicating that patients carrying the A-allele at the rs41275743 locus or the rs4648143 locus of the NFKB1 gene were more likely to develop AKI after sepsis. Interestingly, we did not find significant differences in the risk of AKI in patients with sepsis of different ages, genders, and BMIs who carried different genotypes at the rs41275743 and rs4648143 loci of the NFKB1 gene. Furthermore, we performed MDR to analyze the association of the rs41275743 and rs4648143 SNPs of the NFKB1 gene with age, sex, and BMI. We found that there was a strong interaction between BMI and the rs4648143 SNP, indicating that obese patients carrying the A-allele at the rs4648143 locus are more susceptible to kidney damage, suggesting the importance of genotyping in such patients.
miRNA is an endogenous small noncoding single-strand small-molecule RNA that regulates gene expression. It was first discovered in Caenorhabditis elegans; it targets mRNA by specific base pairing and silences the function of the target mRNA after transcription. It can regulate many processes of cellular activities, including cell development, differentiation, proliferation, and apoptosis (Xiong et al., 2015). In this study, we selected several miRNAs, such as hsa-miR-580, hsa-miR-671-3p, hsa-miR-886-5p, hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9. According to the TargetScan prediction, the binding sites of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p to the NFKB1 gene exist at the rs41275743 locus SNP, while the binding sites of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9 to the NFKB1 gene exist at the rs4648143 locus SNP. From the results of this study, we showed that rs41275743 SNP was associated with plasma levels of hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p, while rs4648143 SNP was associated with plasma levels of hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9.
There are some limitations in this study. First, there was no direct evidence in this study to support the effect of rs41275743 locus SNP on the regulation of NFKB1 gene expression by hsa-miR-580, hsa-miR-671-3p, and hsa-miR-886-5p, as well as the effect of the rs4648143 locus SNP on the regulation of NFKB1 gene expression by hsa-miR-299-5p, hsa-miR-557, and hsa-miR-9. In addition, the results of this study need to be further confirmed in the sepsis model. Moreover, the occurrence of AKI in sepsis is likely to be caused by a combination of multiple genes and multiple factors. Therefore, to further elucidate the mechanism of AKI in patients with sepsis, it is necessary to expand the scope of the research.
Conclusion
The NFKB1 gene SNPs rs41275743 and rs4648143 are associated with the risk of AKI in sepsis. It is likely that SNPs rs41275743 and rs4648143 influence the regulation of NFKB1 gene expression by miRNAs; however, further experiments are needed to confirm the underlying mechanisms in vitro and in sepsis models.
Footnotes
Authors' Contributions
Q.X. conceived and designed the experiments. J.S., X.C., J.S., and G.J. performed the experiments. J.S., X.C., J.S., and G.J. analyzed the data. Q.X. and J.S. wrote the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Traditional Chinese Medical Science and Technology Plan of Zhejiang Province (2019ZB053).