
Abstract
Objectives:
The primary aims of this study were to determine if any correlation exists in cases of fracture fixation among: (1) bacterial profiles recovered from the instrumentation and adjacent tissues; (2) the type of orthopedic injury; and (3) the clinical outcome—union versus nonunion. A secondary goal was to compare culture and molecular diagnostics for identifying the bacterial species present following fracture fixation.
Design:
Single-institution, prospective case-control cohort study.
Setting:
Single level 1 trauma center.
Patients:
Forty-nine bony nonunion cases undergoing revision internal fixation and 45 healed fracture controls undergoing removal of hardware.
Intervention:
Bacterial infection was detected by standard microbial culture methods and by a pan-eubacterial domain, molecular diagnostic (MDx) assay. Confirmation of culture and MDx results was achieved with bacterial ribosomal 16S rRNA fluorescence in situ hybridization (FISH) to visualize bacterial biofilms.
Main Outcome Measurements:
MDx and microbial culture methods results were the primary study outcomes.
Results:
Ninety-four percent of the nonunion cohort and 93% of the union cohort had bacteria detected by the MDx. Seventy-eight percent of the nonunion cases and 69% of the controls were culture negative, but MDx positive. Although no significant differences in bacterial composition were observed between the cases and controls, differences were observed when cases were divided by comorbidities.
Conclusion:
The MDx is more sensitive than microbial culture in detecting bacterial presence. The lack of significantly different findings with regard to bacterial profile identified between the cases and controls suggests that host factors and environmental conditions are largely responsible for determining if bony union will occur.
Level of Evidence:
Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.
Introduction
Bony fracture healing can be affected by many variables. Some of these are properties of the host, some are nutritional, and some are secondary to the trauma (Sen et al., 2000; Hannigan et al., 2015; Lawrenz et al., 2017). Delay in fracture healing can lead to prolonged morbidity for the patient and increased burden on the patient and health care system. One variable that has been associated with delay in healing is infection (Glass et al., 2011; Hannigan et al., 2014; Palmer et al., 2014).
Chronic bacterial infections including device-related infections are caused predominantly by bacteria that have adopted the multicellular biofilm mode of growth (Costerton et al., 2003; Ehrlich et al., 2005, 2008, 2010; Stoodley et al., 2005, 2011a,b; Wolcott and Ehrlich, 2008). These medically important biofilms can develop on mucosal surfaces (Ehrlich et al., 2005, 2010), and on inert materials used in the construction of medical implants including orthopedic devices (Costerton et al., 2003; Schaudinn et al., 2007). Once formed, bacterial biofilms even when composed of largely what are considered nonpathogenic bacteria through population-level virulence factors can persist and result in devitalization of adjacent tissues (Hu and Ehrlich, 2008). Their presence can often go undetected for long periods of time by both the host's defense systems and by medical practitioners, particularly when they are composed of nonpyogenic bacterial species. Moreover, even when there is clinical suspicion of biofilm infection, the biofilm bacteria can be extremely difficult to identify with current cultural microbiological diagnostic methods (Post et al., 1995; Marshall et al., 1997; Shen et al., 2005; Aul et al., 1998; Kathju et al., 2009; Jacovides et al., 2012; Kreft et al., 2013; Zmistowski et al., 2014). Treating them medically is even more difficult as they are highly recalcitrant to antibiotics owing to metabolic quiescence triggered by the bacterial stringent response (Borriello et al., 2004, 2006; Nguyen et al., 2011).
We have hypothesized that biofilms are much more common than previously thought at fracture sites treated with internal fixation (Palmer et al., 2014). In a preliminary study we reported 30 of 34 nonunions had biofilm bacteria present using pan-domain molecular diagnostics and fluorescence in situ hybridization (FISH), whereas only 8 of 34 were culture-positive infections (Palmer et al., 2014). Similar findings have also been reported in revision hip and knee arthroplasty (Jacovides et al., 2012). In this study we investigated three hypotheses: (1) molecular diagnostic methods are superior compared with culture for the detection of bacteria associated with bony fracture infections; (2) biofilms are present at a higher frequency in nonunions than healed fractures; and (3) biofilms are more prevalent in open fractures compared with closed fractures.
Materials and Methods
Patient selection
The study was approved by the Allegheny General Hospital Institutional Review Board before the start of enrollment. All patients in the study provided consent and were enrolled prospectively by one of the clinical authors (M.P.P., D.T.A., G.T.A., J.J.S.). Exclusion criteria included skeletally immature patients and patients with insufficient sampling for molecular diagnostics. A total of 94 patients were enrolled; 49 patients with the diagnosis of fracture nonunion, and 45 patients with the diagnosis of fracture union. The diagnosis of nonunion was made based on criteria previously described (Palmer et al., 2014). Patients with united fractures following internal fixation were offered inclusion into the union cohort when they were scheduled for elective hardware removal. These patients were followed until clinically stable for discharge (wounds healed, pain resolved, functional limitations overcome, or infection cleared). Patients were entered into the nonunion cohort if they had not achieved fracture healing in the time expected following trauma and were subsequently followed for another 2 years, or until there was clinical and radiographic evidence of union. Nonunion patients were not treated with preoperative antibiotics, but in some cases of frank infection during surgery antibiotic beads were used. Treating surgeons were blinded to the results of the molecular diagnostic (MDx) results as the technology is not U.S. Food and Drug Administration (FDA) approved for clinical use.
Sample collection
During surgery, the explanted hardware and specimens of adjacent soft tissue and “membrane” (slimy amorphous accretions in the area around the fracture) were collected aseptically and sent for analysis. Specimens were collected from the area immediately surrounding the hardware to be removed, with the exact location for each sample being chosen at the surgeons' discretion. All specimens were analyzed separately by routine microbiological culture methods at the hospital's onsite clinical microbiology laboratory and by the eubacterial pan-domain BACS assay performed on the Ibis T-5000 multiplex PCR-MS system (MDx). The results of the MDx system were independently confirmed by FISH. Clinicians were blinded to the Ibis and the FISH data until after the expiration of the IRB mandate.
Microbiology
Wound specimens were collected intraoperatively using swabs to sample the immediate area surrounding the nonunion. After sampling the deepest portion of the wound, the swabs were replaced into the holder, placed into a biohazard bag, and transported immediately to the onsite clinical microbiology laboratory. If a tissue sample was taken at the same time, it was collected in a sterile container, placed in a biohazard bag, and transported immediately to the onsite clinical microbiology laboratory for processing.
Routine wound swabs were used to inoculate blood agar plates (BAP), chocolate agar plates (CHOC), MacConkey agar plates (MAC), and Columbia-colistin-nalidixic acid agar (CAN). In addition, a Gram stain was made by rolling the other swab on a glass slide to make a thin film. The agar plates were then incubated in 5% CO2 at 35°C. The tissue samples collected for culture and Gram stain were first cut with a sterile scalpel to make a touch prep. The rest of the tissue was lysed in a sterile disposable tissue grinder and aliquots of the lysate were used to inoculate a set of agar plates as described previously, as well as being used to inoculate a tube of thioglycolate media (THIO). All incubations were again performed at 35°C in 5% CO2.
All slides made for Gram stain were examined for cells and bacteria using a high-magnification oil immersion objective. Microorganisms were reported based on type and number; and any polymorphonuclear leukocytes (PMNL) and mononuclear cells were recorded, and all organisms seen were reported and quantified numerically. The incubated cultures (both agar plates and broth) were examined at 24 h. If there was no growth on plates or in broth, they were incubated for an additional 24 h. After day 2, if no growth was seen in broth or plates, the plates were discarded and reported as “no growth day 2” and the THIO tubes were placed in the incubator for an additional 3 days. The THIO tubes were examined every 24 h until 5 days, and if no growth was found “no growth day 5” was reported.
If growth was seen on plates after the first 24 h, then the sample was re-incubated on plates and in broth for an additional 24 h. All significant isolates were reported on day 2, and any relevant plates were saved until day 5. If there was no growth on the plates, but growth in the THIO tube, the THIO culture was Gram stained and subcultured on appropriate plates based upon the findings. All plates inoculated from the THIO tubes were incubated and analyzed daily for 5 days and then disposed.
Molecular diagnostics
MDx analysis of the samples was carried out as previously described (Melton-Kreft and Spirk, 2016). In brief, 1 mm (Lawrenz et al., 2017) biopsies collected from the immediate area surrounding the nonunion were placed into sterile microcentrifuge tubes containing 270 μL of ATL lysis buffer (cat. no. 19076; Qiagen, Germantown, MD) and extracted using the Qiagen DNeasy Tissue kit (cat. no. 69506; Qiagen). Ten microliters of each sample was loaded per well (16 wells/specimen) into Ibis BAC detection polymerase chain reaction (PCR) plates (cat. no. PN 05N13-01; Abbott Molecular). The BAC detection plate is a 96-well plate, which utilizes 16 separate PCRs for each sample to comprehensively survey all bacterial species, several important antibiotic resistance genes, and common Candidal species. This is accomplished by using a combination of: (1) domain-based omnipresent loci (e.g., 16s and 18S rDNA); (2) and various phyla/class specific genes; and (3) pathogen-specific genes for key species of interest (e.g., the Staphylococcus-specific tufB gene).
An internal calibrant consisting of a synthetic nucleic acid template is also included in each well of each assay, controlling for false negatives (e.g., from PCR inhibitors) and providing for quantitation of signal. PCR amplifications were carried out as described (Jiang and Hofstadler, 2003). The PCR products were then desalted in a 96-well plate format and sequentially electrosprayed into a time-of-flight mass spectrometer. The Ibis technology can detect any bacterial genome that exceeds 1-2% of the total bacterial population, and it identifies the cognate species by comparing the calculated base ratio of the amplimers with a database covering thousands of species (Ecker et al., 2008). The inclusion of an internal calibrant provides for a quantitative determination of the number of copies of any bacterial gene in the sample, which is expressed as “genomes per well.”
All samples in which Staphylococcus epidermidis or Propionibacterium acnes were found to contain fewer than 10 genomes per well were excluded as potentially representing skin contaminants. However, all other species were recorded and considered significant. At present, it takes 6-8 h to complete a sample analysis with the Ibis. For confirmation, all MDx-positive cases with suitable remaining tissue samples were then subjected to FISH using 16S RNA probes corresponding to the bacterial species identified by the Ibis. There were three cases where there was insufficient tissue to perform FISH.
Biofilm imaging
FISH analysis of the samples was carried out as previously described (Nistico et al., 2009, 2011; Palmer et al., 2016). In brief, specimens were fixed in 4% paraformaldehyde, then washed three times with phosphate-buffered saline (PBS), and stored at −80°C in 1:1 ethanol/PBS until processed. The bacterial cells were permeabilized with lysozyme and hybridized with the FISH probes as described (Nistico et al., 2009, 2011). The FISH-stained tissue was then mounted and imaged by confocal laser scanning microscopy. Probes used to perform FISH on any given sample were selected based on the MDx or culture results, and corresponded to species-specific, genus-specific, or “universal” eubacterial probes (Table 1) (Wagner et al., 1994; Amann et al., 1996; Moter et al., 1998; Hogardt et al., 2000; Kempf et al., 2000; Trebesius et al., 2000; Wellinghausen et al., 2007; Poppert et al., 2010).
List of Species-Specific and Genus-Specific Fluorescent 16S rRNA Probes and Their Intended Targets Used for Fluorescence In Situ Hybridization
Statistics
Participant demographics and various categorical outcomes were summarized and presented as mean (standard deviation) for continuous variables or median (interquartile range) for nonparametric continuous variables and frequency (n, percentage) for categorical variables. A chi-square or Fisher's exact test were used for categorical variables for comparing various groups (e.g., union vs. nonunion). Histograms were generated from frequency of total number of bacteria detected per each categorical variable (Figure 3).
Patients medical records listing, current or prior history of tobacco or alcohol use; body mass index (BMI) >30; osteopenia; depression; anxiety; and diabetes were included in the positive comorbidities cohort. Patients without these diagnoses were included in the negative comorbidities cohort. StataCorp. 2009. Stata Statistical Software: Release 11 (College Station, TX; StataCorp LP) was used to conduct the statistical analysis and generate the histograms.
Results
A total of 94 patients were included in this prospective cohort study: 49 (52%) in the nonunion cohort and 45 (48%) in the union cohort. Patients in the nonunion and union cohorts had similar demographics with no statistically significant differences between the groups in age (49.4 vs. 44.1), BMI (28.9 vs. 27.0), and tobacco use (24 vs. 17). Overall 58 patients experienced an open fracture: 29 nonunion patients and 29 union patients. Patients in the nonunion cohort had an average of 2.34 surgeries before enrollment, compared with 2.09 in the fracture union cohort. After their enrollment in the study, the nonunion cohort underwent an average of 0.92 more surgeries per patient and all achieved fracture union by 12 months after their enrollment (Table 2). OTA fracture classification was varied for patients enrolled in the study (Table 3) (Marsh et al., 2007).
Patient Demographics Divided by Clinical Diagnosis
BMI, body mass index.
Orthopedic Trauma Association Classification for Fractures
Frequency and percentage listed for each class of fracture included in the study. Classification was not obtained at the time of data collection for nine patients; these fractures are listed as N/A.
N/A, not available.
Ninety-four percent (46/49) of the nonunion and 96% (43/45) of the fracture union cohort were found to have bacteria present by MDx testing compared with 16% (8/49) and 24% (11/45) with positive cultures, respectively. Seventy-eight percent (38/49) of patients in the nonunion cohort and 69% (31/45) of the fracture union cohort patients were negative by culture, but positive by MDx. Five total patients, three from the nonunion and two from the fracture union cohort were negative by both MDx and culture (Table 4).
Comparison of Culture and Molecular Diagnostic Testing Divided by Clinical Diagnosis
Cx = culture; MDx = molecular diagnostic (polymerase chain reaction-electrospray ionization-time-of-flight-mass spectroscopy [PCR-ESI-TOF-MS]).
The most common bacterial species identified by the Mdx included P. acnes (35%), Staphylococcus aureus (32%), Treponema denticola (21%), and Enterococcus faecalis (21%); the latter two are known periodontal pathogens. The most common bacteria identified by culture were staphylococcal species 15/19 (79%). The MDx findings in the culture-positive cases correlated with the culture in 7/8 (88%) cases in the nonunion cohort and 8/11 (73%) cases in the fracture union cohort. In those cases where the MDx did not confirm the culture results, FISH confirmed the MDx finding in 4/4 (100%) of the cases (Fig. 1). Overall, FISH was used as an MDx confirmatory technique on 91 cases and confirmed the MDx result in 86 cases (95%). FISH also illustrated the presence of bacterial biofilms on both orthopedic implants and host tissue at the fracture site (Fig. 2).
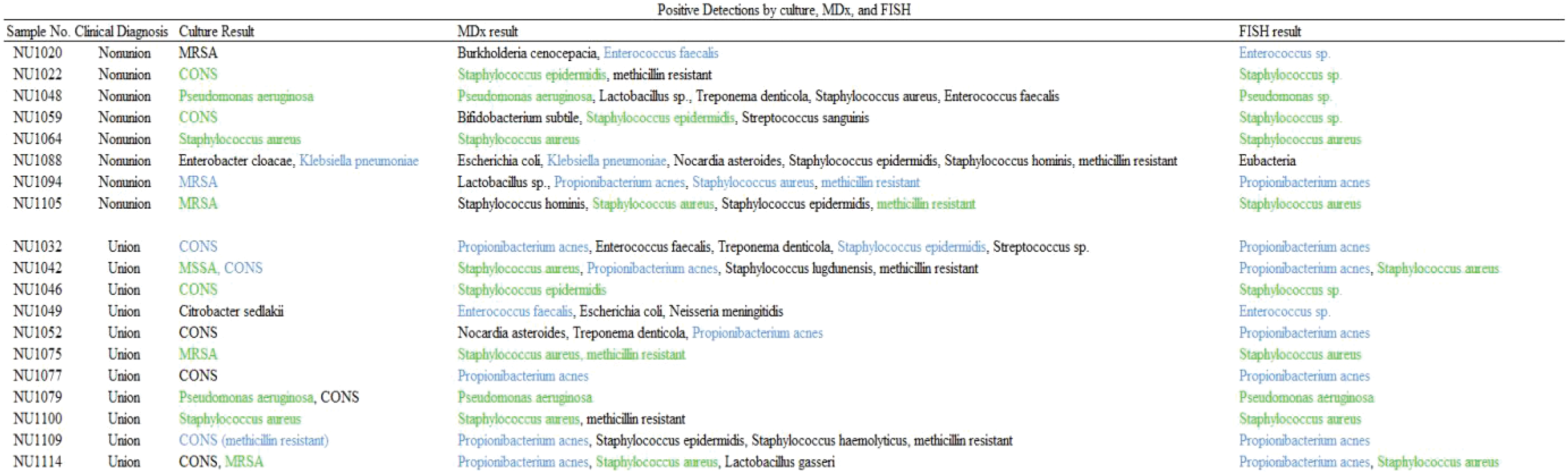
Bacterial species detected by culture, pan-domain MDx, and 16S FISH associated with internal fixation of bony fractures. Bacterial infections were identified using three independent and orthologous methods of detection: microbial culture; a pan-domain MDx; and 16S rRNA gene fluorescent in situ hybridization (16S FISH). Bacterial species that were detected by two of the detection methods are highlighted in blue, and those that were identified by all three techniques are highlighted in green. MDx = molecular diagnostic (polymerase chain reaction-electrospray ionization-time-of-flight-mass spectroscopy [PCR-ESI-TOF-MS]). CONS, coagulase-negative staphylococci; FISH, fluorescence in situ hybridization; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive Staphylococcus aureus.

Confocal micrographs of samples from bacterial culture-negative, MDx (Ibis)-positive cases in which the tissues were reacted with bacterial 16S FISH probes corresponding to the bacterial species identified using the Ibis-MDx.
The eight most common bacterial species were evenly distributed with no discernible pattern differences between the nonunion and union cohorts or the open and closed cohorts (p = 0.53), such that no species seemed clearly associated with promoting or inhibiting bone union (Fig. 3). However, there was a correlation between bacteria and the presence/absence of comorbidities in the nonunion cases. In the nonunion cases, in the absence of comorbidities, the rates of methicillin-resistant Staphylococcus aureus (MRSA) were significantly higher (33%) than the cases with comorbidities (5%). In addition, E. faecalis was detected in 23% of cases with comorbidities (Table 5) but was never detected when comorbidities were absent (Table 6). In addition, bacterial species diversity was increased in open wounds with a union diagnosis than in open wounds with a nonunion diagnosis (Fig. 4).
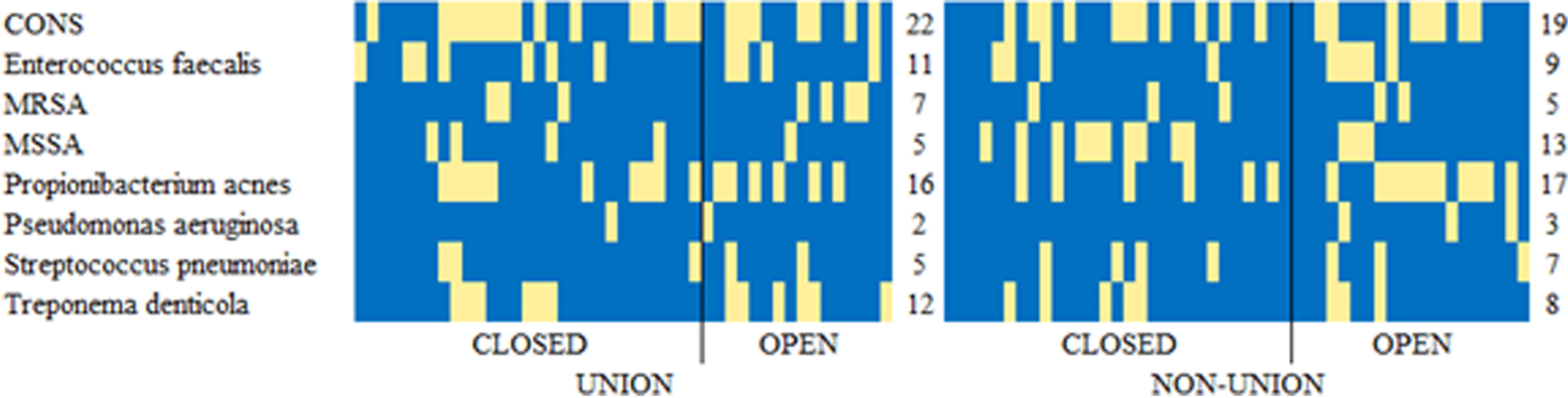
Heat map shows the distribution of top species detected in 94 samples. Bacteria with at least 10 unique detections by MDx across all cases are reported. A yellow colored square represents a detection of species (row) in a patient (column). The columns are ordered by categories, with black line separating closed/open fracture. The numbers on the right of each heat map indicate the total frequency of species in the union and nonunion cohort. CONS, coagulase-negative staphylococci.
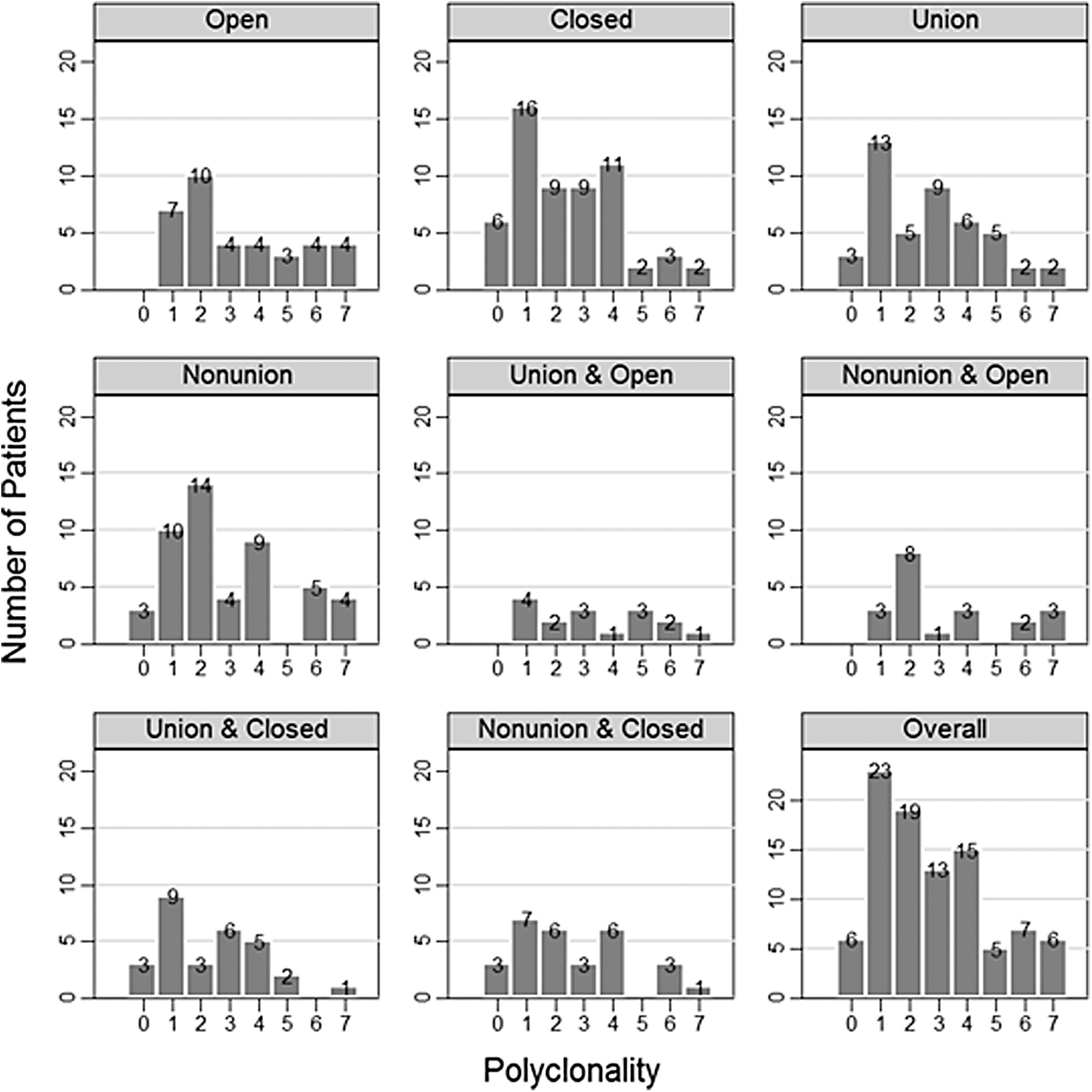
Polyclonality plots show the frequency of patients (y-axis) with the given number of bacterial species identified via MDx by all pairwise combinations of open/closed and union/nonunion states. Numbers above the bars show the exact frequencies. Note that each plot has a different total number of patients (refer Table 2).
Comorbidities Included in the Analysis
Bacterial Species Prevalence Based on Presence/Absence of Comorbidities and Clinical Diagnosis
CONS, coagulase-negative staphylococci; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive Staphylococcus aureus; WBC, white blood cell count.
Discussion
Infection after bony fracture can be a devastating complication increasing costs of care and leading to poorer outcomes (MacKenzie et al., 2007; Bachoura et al., 2011). With the advent of improving technologies for diagnosing bacterial infection and better understanding of biofilm biology, infections following orthopedic surgery are being detected with increased frequency. In this study, we have shown that cultures have a very poor sensitivity for detecting bacterial presence in a sample. These findings are similar to those reported elsewhere (Jacovides et al., 2012; Palmer et al., 2014).
It is important to point out, however, that our cultural methods, as performed in our routine clinical microbiology laboratory, are probably insufficient for the detection of certain slow-growing bacterial species, in particular P. acnes. This organism has been reported to require 13 or more days of culture for isolation (Butler-Wu et al., 2011; Portillo et al., 2013). Moreover, it is possible that if we had used sonication of the removed implants that we would also have increased our culture yield (Trampuz et al., 2007; Wyatt et al., 2016). These methodologies were not used in this study because they were not standard of care at the time of study enrollment. Finally, we did not use any of the emergent biomarker assays for detecting infection associated with orthopedic procedures such as leukocyte esterase strips or Synovasure® for detection of alpha defensins (Wyatt et al., 2016).
Owing to the fact that all medical implants are associated with greatly elevated risks of bacterial biofilm infection (Costerton et al., 2003; Ehrlich et al., 2005, 2012; Wolcott and Ehrlich, 2008; Stoodley et al., 2011a,b; Jacovides et al., 2012), making a diagnosis of a clinically actionable infection following internal fixation, regardless of clinical outcome, is necessary so that appropriate surgical principals can be applied to remove the infection and/or source of infection to help create a healthy healing environment and minimize the risk of sequelae. In this study all the patients in the nonunion cohort did eventually go on to heal their fractures—on average 12 months and 0.9 surgeries after study enrollment.
Somewhat surprisingly, a significant majority of even the healed fracture (control) cases were demonstrated by multiple methods (MDx and FISH) to have bacterial species of known pathogenic potential present. There were, however differences in the percentages of nonunion cases with respect to the bacterial species isolated based on patient comorbidities. In the absence of comorbidities 33% of nonunion cases were infected with MRSA, whereas only 5% of cases with comorbidities had MRSA. This suggests that MRSA, which would likely be picked up from the environment, is able to cause infection in an otherwise healthy individual. In contrast E. faecalis was only found associated with nonunions in the presence of comorbidities. Because this organism is most likely to infect implants through hematogenous spread, its finding in patients with comorbidities is consistent with known role in chronic apical periodontal disease. Of importance, the nonunion patients also were experiencing pain, possibly as a sequela of infection.
It is interesting to note that many of the infections in both the union and nonunion cases resulted from periodontal pathogens including T. denticola, Brevundimonas sp., and E. faecalis. These findings are suggestive of systemic spread following transient bacteremias after both tooth brushing and dental procedures that have long been documented (Lindqvist and Slätis, 1985; Lockhart et al., 2008). Thus, in the absence of device removal, these occult infections could potentially lead to chronic osteomyelitis even after repair of the fracture. These findings collectively serve to not only reinforce the need for meticulous sterile technique and attention to detail during operative procedures, but also that infection can occur following systemic spread and that infection monitoring using sensitive means should be used in all cases.
The rates of discordance between culture and MDx/FISH are directly attributable to the type of bacteria detected. When MDx detects staphylococci, whether S. aureus or one of the coagulase-negative species, the culture is also frequently positive for these organisms, but for any of the fastidious, slow-growing, anaerobic, or nonpyogenic species, the culture did very poorly. These dichotomous cultural findings are again consistent with previously published comparative diagnostic studies (Jacovides et al., 2012; Ehrlich, 2016; Palmer et al., 2016). The few culture-positive/MDx-negative results among the control cohort likely reflect contamination of the swabs with Staphylococci during collection, as these specimens were all FISH-negative.
This study demonstrated that bacteria are abundant in both fracture nonunions, as well as healed fractures that are undergoing removal of hardware. Such findings are not surprising as bacteria such as P. acnes, Pseudomonas aeruginosa, and the staphylococcal species likely gained entry either during the initial trauma in the case of open fractures, or during the fixation process for any fracture with internal fixation. Moreover, it is also likely that in some cases the infections resulted from systemic spread following brief bouts of bacteremia, particularly when the observed species are known periodontal pathogens such as T. denticola, Brevundimonas sp., and E. faecalis.
As stated previously, cultures are inferior to molecular diagnostics and this dichotomy is even greater when dealing with fastidious organisms. This likely explains why the majority of culture-positive infections involved either staphylococci (both coagulase negative and positive) or P. aeruginosa, as these are rapidly growing aerobic, pyogenic pathogens. The role of host factors determining clinical outcome in the face of bacterial burden is supported by the findings that the control group was younger, had a lower BMI on average, and also contained fewer patients with diabetes and smokers than the case group. In addition, the influence of host comorbidities on bacterial populations, in the nonunion cases, is an interesting finding. The high prevalence of S. aureus along with the absence of E. faecalis and P. aeruginosa in the zero-comorbidity cohort suggests that healthy hosts are less likely to experience nonunion owing to hematogenous spread and more likely to experience nonunion from the initiating trauma. However, this trend needs to be explored in larger cohort studies.
The findings from this study again point to the superiority of pan-domain MDx methods over microbial culture for the detection of bacteria in clinical specimens (Tuttle et al., 2011; Nickel et al., 2015; Earl et al., 2018) and support their use in clinical diagnostics for bone fracture—particularly in cases of nonunion that are culture negative. However, in the case of bony union versus nonunion, the lack of significantly different MDx findings with regard to bacterial profiles identified between the cases and controls suggests that whether a given patient heals in the face of infection is likely dependent on many factors including the overall health and lifestyle of the patient (comorbidities), infecting bacterial load, and host genetics.
It is important to note that in multiple controlled studies of persistence of nonviable bacteria and bacterial DNAs that both forms are rapidly cleared from the host, whereas live bacteria—even when antibiotic treated can be detected for weeks following loss of culturability (Post et al., 1996; Kaplan et al., 2018); therefore, MDx findings are prima facie evidence of an ongoing infection.
Footnotes
Acknowledgments
The authors acknowledge the contribution of Bill Costerton to the development of the orthopedic biofilm program, of which this study is a part, at Allegheny General Hospital and Allegheny Singer Research Institute, prior to his untimely death. The authors thank Kelly J. Shields, PhD and Curren Katz, PhD at the Data Science R&D, Highmark Health for statistical guidance. The authors thank Carol Hope for help with the preparation of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The work was supported by Allegheny General Hospital and Allegheny Singer Research Institute; Drexel University College of Medicine; a grant from Synthes Corporation; a grant from Ibis Biosciences; and grants from Abbott Molecular.