
Abstract
Background:
We aimed to evaluate the association between the vascular endothelial growth factor (VEGF) gene +936C>T polymorphism and digestive system tumors using a meta-analysis.
Methods:
Studies of the association between the VEGF+936C>T polymorphism and digestive system tumors published before December 2019 were searched in PubMed, EMBASE, Web of Sciences, the Chinese Biological and Medical Database (CBM), and the China National Knowledge Infrastructure (CNKI). The odds ratio and the corresponding 95% confidence interval were used as the effect indicators. A meta-analysis of original data was performed with different genetic models using the Stata 13.0 software. The reliability of the association was evaluated using the heterogeneity test, sensitivity analysis, false-positive report probability (FPRP), and bias test.
Results:
This meta-analysis included 37 publications with a total of 8568 digestive system tumor patients and 10,870 cases in the control populations. The overall combined analyses showed that the VEGF+936C>T gene polymorphism was significantly correlated with digestive system cancer susceptibility with the T allele increasing the risk of digestive system cancers. A stratified analysis based on ethnicity showed that the VEGF+936C>T gene polymorphism significantly increased the risk of digestive system tumors in both Asian and Caucasian populations. Additional stratified analyses based on tumor type showed that the VEGF +936C>T gene polymorphism was associated with colorectal cancer, oral cancer, and esophageal cancer. The sensitivity analysis (p < 0.2) and FPRP results also confirmed the reliability of these associations.
Conclusions:
This meta-analysis supported previous findings that the VEGF +936C>T gene polymorphism is significantly associated with an increased risk of the development of digestive system malignant tumors. This association still requires large-scale epidemiological studies for further validation.
Introduction
Currently, digestive system tumors have a high incidence and mortality. They are considered the main reason for malignant tumor deaths and have become one of the most important pubic heath issues in the world (Wang et al., 2016). The causes of digestive system cancer are complicated, and genetic and environmental factors play important roles in cancer development and progression. Epidemiological studies indicate that smoking, drinking, eating habits, geographical environment, and Helicobacter pylori infection are important external factors that increase the risk of digestive system cancer (Goh et al., 2014; Abnet et al., 2018). However, even when exposed to the same environmental factors, only a small portion of people develop cancers, indicating that genetic factors may play a leading role in the development and progression of cancers. A large number of studies have reported the association between gene polymorphism and the risk of digestive system tumors (Ma et al., 2014; Li et al., 2020). For example, many sites on the vascular endothelial growth factor (VEGF) gene have been extensively studied (Ruggiero et al., 2011).
Previous studies have shown that VEGF is a heparin-binding growth factor specific to vascular endothelial cells and can induce angiogenesis in the body. VEGF is a highly conserved homodimeric glycoprotein. As a vascular endothelial cell-specific mitogen, it has the functions of both promoting vascular endothelial cell division and proliferating and increasing vascular permeability, and it is closely associated with the growth and metastasis of malignant tumors (Ferrara et al., 2003; Yang et al., 2015). The VEGF gene localizes in 6p21.3 of the chromosome 6. Its full length is 14 kb, including 8 exons and 7 introns (Vincenti et al., 1996). A large body of literature has confirmed that many mutation sites on this gene can affect VEGF protein expression. For example, the VEGF -2578C, -460T, and +405C alleles can increase the VEGF concentration in plasma and can significantly increase the risk of ovarian cancer (Steffensen et al., 2010), whereas the +936T allele can reduce the VEGF concentration in serum and reduce the risk of breast cancer (Renner et al., 2000; Krippl et al., 2003). Many studies on the association between the VEGF +936C>T polymorphism and digestive system tumors have been published. However, this association is still inconclusive. Because of different ethnicities and disease types, the difference in the distribution of the VEGF +936C>T is large. In addition, due to the limitation of the sample size in a single study, these studies are not adequate to completely explain this potential association. Therefore, this study aimed to use a meta-analysis for the quantitative pooling of existing studies to obtain a reliable conclusion regarding the association between the VEGF +936C>T gene polymorphism and digestive system cancer susceptibility.
Materials and Methods
Search strategy
Studies on the association between the VEGF +936C>T gene polymorphism and digestive system cancer susceptibility were systemically searched in PubMed, EMBASE, Web of Sciences, Chinese Biological and Medical Database (CBM), and the China National Knowledge Infrastructure (CNKI). The search time was from the establishment of these databases to December 2019. Relevant conference articles were manually searched using the journal databases in the library of Army Medical University. The search terms were (VEGF) and (polymorphism or SNP or variant or mutation), and (cancer or tumor or carcinoma).
Inclusion and exclusion criteria
Studies included in the meta-analysis were required to meet the following criteria: (1) the research topic of the articles was the association between the VEGF +936C>T gene polymorphism and digestive system cancer susceptibility; (2) the research design was human-related case controlled, cohort or cross-sectional studies; (3) digestive system cancer patients were diagnosed and confirmed by pathological and/or histological examinations; (4) there were enough genotype data to calculate odds ratios (ORs) and the corresponding 95% confidence intervals (CIs). If the following conditions were present, the publication was excluded: (1) studies with inadequate information, including incomplete research data or data that could not be obtained; (2) studies that were abstracts, reviews, or repeatedly published articles; or (3) studies on the mortality or survival rates of digestive system cancer. As this was a systematic review and did not use primary data, the need for institutional review board approval was waived.
Data extraction and quality evaluation
Data were extracted by two researchers independently using the uniform data table. In cases of disagreement, agreement was reached through discussion. The extracted data included first author, publication time, area, cancer type, source of the control group, matching conditions, samples sizes of the disease group and the control group, the number of carriers of all genotypes, and the Hardy-Weinberg equilibrium (HWE) test results of the control group. For repeatedly published articles, only the article with the highest quality and the largest sample size or the most detailed information was selected. If a study included multiple sources or study populations, data were extracted separately.
Each included publication was scored using a previously developed standard (Thakkinstian et al., 2005; Zhang et al., 2017). This standard was extracted and modified from previous studies (Table 1) and included six items: representativeness of cases, source of controls, case-control matching, specimens used for determining genotypes, HWE, and total sample size. These scoring items were evaluated based on traditional epidemiological factors and cancer gene issues. The total score was 18 points. Studies with a score <12 were considered “low quality,” and those with a score ≥12 were considered “high quality.”
The Quality Evaluation Scale for Included Studies
HWE, Hardy-Weinberg equilibrium.
Statistical methods
All statistical tests used in this study were two-tailed tests unless otherwise stated. p < 0.05 indicated that the difference had statistical significance. The association between mutation sites and the digestive system cancer risk was evaluated using ORs and the corresponding 95% CI. The statistical significance of the combined OR value was determined using the Z test. Whether the genotype of the control group conformed to HWE was evaluated using the χ2 test. The heterogeneity among all studies was analyzed using the Cochrane Q test (Cochran, 1954). The statistic Q approximately conformed to the χ2 distribution with a degree of freedom of k-1 (k was the number of studies); when p was lower than 0.10, there was heterogeneity among studies. In addition, the I2 value was combined to quantitatively evaluate the level of heterogeneity. The I2 value was between 0% and 100%; when the value was higher, the heterogeneity was higher. Usually, I2 lower than 25% indicated the presence of mild heterogeneity; I2 between 25% and 50% indicted the presence of moderate heterogeneity; I2 higher than 50% indicated the presence of high heterogeneity. When the heterogeneity test of all studies showed p < 0.10 or I2 > 50%, the random effects model (DerSimonian and Laird, 1986) was used for the meta-analysis; otherwise, the fixed effects model (Mantel and Haenszel, 1959) was used. For the sensitivity analysis, each study was excluded one by one, the meta-analysis was reperformed, and changes in the results were observed to determine the stability of the conclusion. The funnel plot was plotted using the effect size and standard deviation to analyze whether the included studies had publication bias. In addition, Begg's rank correlation method was applied to examine the asymmetry of the funnel plot (Begg and Mazumdar, 1994). All meta-analyses were performed using Stata13.0.
The method developed by Wacholder et al. (Wacholder et al., 2004) was used to calculate the false-positive report probability (FPRP) of the associations under each significant genetic model to determine whether the association was a false-positive result. The FPRP value was calculated under the condition of an OR value of 1.5 using the prior probability of 0.05. When the FPRP value was lower than 0.2, the association was noteworthy. The FPRP value and the statistical performance were obtained using the Excel calculator provided by Wacholder et al.
Results
Characteristics of the included studies
The preliminary search obtained 529 related articles. After repeated articles were excluded, there were 426 articles. Based on the inclusion and exclusion criteria, the preliminary screening of articles was performed by reading the titles and abstracts. A total of 364 articles that were not related to the study topic were excluded. After further reading the whole articles, 28 articles were excluded, including 16 non-case-controlled or cohort studies, 6 abstracts or systemic reviews, 4 studies on the mortality and survival rates of digestive system cancer, and 2 articles for which the complete genotype frequency or data could not be obtained. In addition, through screening the references of the included studies, previous meta-analyses of the association between VEGF gene polymorphism and digestive system cancer, and review articles, 3 additional articles were obtained. Therefore, 37 articles (Chae et al., 2006, 2008; Tzanakis et al., 2006; Wu et al., 2006, 2009a, 2009b; Nikiteas et al., 2007; Yapijakis et al., 2007; Bae et al., 2008a, 2008b; Cheng et al., 2008; Hofmann et al., 2008; Hsing et al., 2008; Ke et al., 2008; Zhai et al., 2008; Al-Moundhri et al., 2009; Dassoulas et al., 2009; Guan et al., 2009; Tahara et al., 2009; Vairaktaris et al., 2009; Kämmerer et al., 2010; Xia et al., 2010; Antonacopoulou et al., 2011; Giacalone et al., 2011; Zhou et al., 2011; Supic et al., 2012; Jang et al., 2013; Sivaprasad et al., 2013; Credidio et al., 2014; Gu et al., 2014; Jannuzzi et al., 2015; Li, 2015; Qasim et al., 2015; Yvamoto et al., 2015; Baitello et al., 2016; and Bai and Ren, 2017; Liu et al., 2017) that conformed to the inclusion criteria were finally obtained, including 8568 patients and 10,870 controls (Fig. 1).

Flow chart of the inclusion and exclusion of articles.
Among the 37 included studies, the study subjects were Asian populations in 17 articles and Caucasian populations in 20 articles. The tumor types were colorectal cancer in 12 articles, gastric cancer in 10 articles, oral cancer in 5 articles, hepatocellular carcinoma in 5 articles, esophageal cancer in 3 articles, and pancreatic cancer in 1 article. In addition, 1 article contained 3 independent data sets and reported gallbladder cancer, extrahepatic bile duct cancer, and ampulla of Vater cancer. Among these 39 independent data sets, the distribution of genotypes in the control group in 33 studies conformed to HWE. The quality scores ranged from 8 to 18. There were 25 high-quality studies (≥12). The results indicated that the overall quality of the included studies was high. The basic characteristics of all the included studies are shown in Table 2.
Basic Characteristics of the Included Articles
The association between the VEGF +936C>T gene polymorphism and the risk of digestive system cancer
The heterogeneity test results showed that there was statistical significance among all the studies in the allele model, dominant model, and heterozygous model. The combination of effect sizes used the random effects model. There was no statistical heterogeneity among all studies in the recessive model and homozygous model. Therefore, the meta-analysis was performed using the fixed effects model. In all genetic models, the VEGF +936C>T mutation and the increase in the risk of digestive system cancer had significant correlation (T vs. C: OR = 1.16, 95% CI = 1.05-1.29, p < 0.001; TT/TC vs. CC: OR = 1.19, 95% CI = 1.05-1.34, p < 0.001; TT vs. CC/TC: OR = 1.19, 95% CI = 1.01-1.39, p = 0.397; TT vs. CC: OR = 1.27, 95% CI = 1.08-1.49, p = 0.297; TC vs. CC: OR = 1.18, 95% CI = 1.03-1.34, p < 0.001). Except for the recessive model, the FRRP values calculated using the prior probability of 0.05 were all lower than 0.2, indicating that the results were noteworthy (Table 3).
The Stratified Analysis Results of the VEGF +936C>T Gene Polymorphism and Digestive System Cancer Susceptibility
Bold values indicate that there is statistical significance in these gene models when subgroup analysis was conducted.
CI, confidence interval; FPRP, false-positive report probability; OR, odds ratio; VEGF, vascular endothelial growth factor.
The stratified analysis was performed based on ethnicity (Fig. 2). The results showed that VEGF +936C>T in Asian populations (T vs. C: OR = 1.15, 95% CI = 1.01-1.33, p < 0.001) and Caucasian populations (T vs. C: OR = 1.18, 95% CI = 1.02-1.36, p = 0.005; TT/TC vs. CC: OR = 1.21, 95% CI = 1.01-1.45, p = 0.002; TT vs. CC: OR = 1.34, 95% CI = 1.05-1.71, p = 0.965; TC vs. CC: OR = 1.20, 95% CI = 1.00-1.44, p = 0.003) were significantly associated with the increase of the risk of digestive system cancer. However, the values of the FPRP analysis were all higher than 0.2, indicating that the evidence of a true association for positive results was not sufficient.
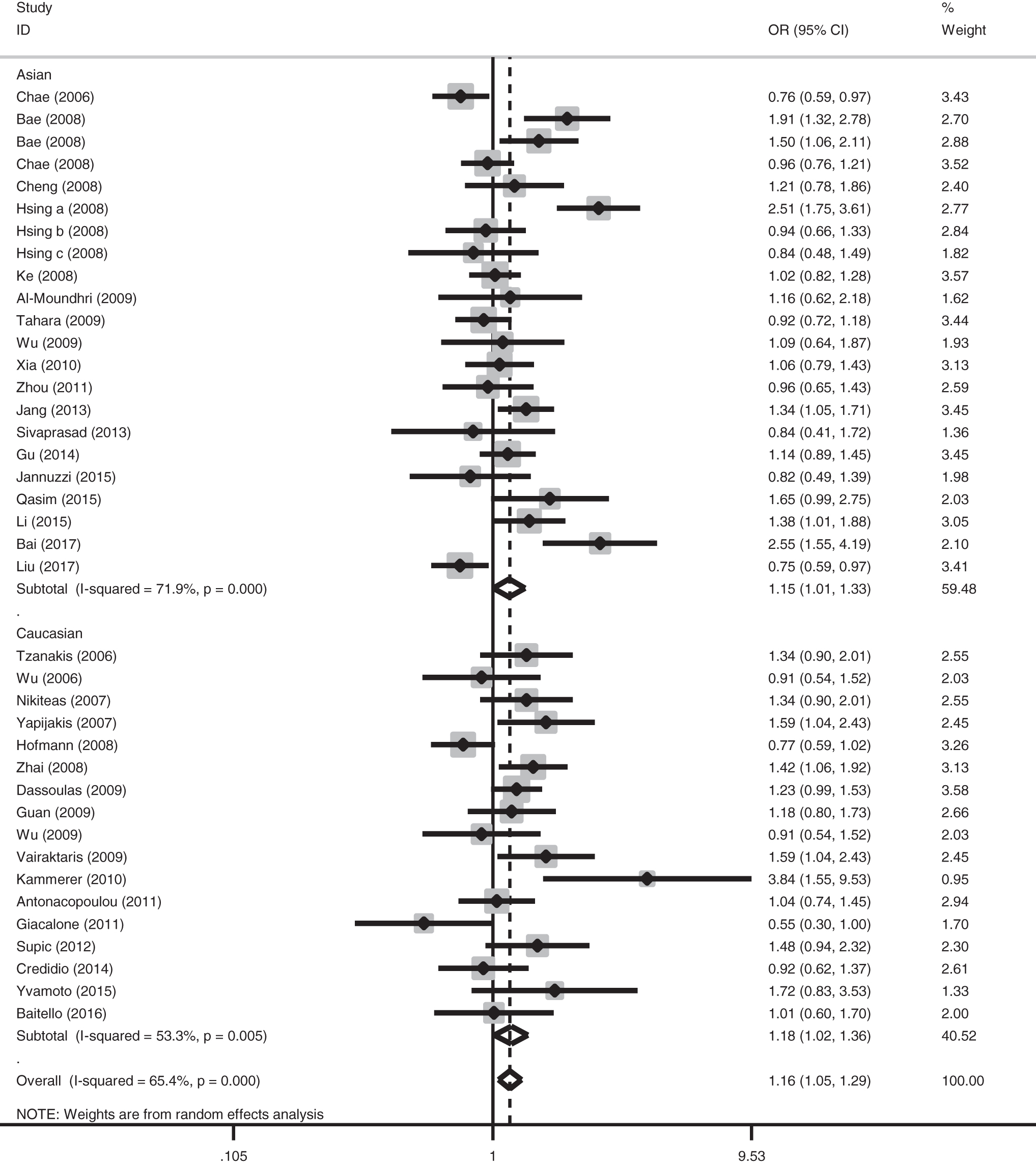
The forest plot of the association between the VEGF +936C>T gene polymorphism and digestive system cancer susceptibility in the allele model (T vs. C) in different ethnicities. The squares and horizontal lines correspond to the study-specific ORs and 95% CIs. The size of the square reflects the weight of each study and the diamonds indicate the overall estimate or pooled ORs in subgroups with their corresponding 95% CIs. CI, confidence interval; OR, odds ratio; VEGF, vascular endothelial growth factor.
The stratified analysis results based on cancer types (Fig. 3) showed that there was no statistical heterogeneity among all studies for all significant associations. In addition, in the colorectal cancer group (TT vs. CC: OR = 1.41, 95% CI = 1.10-1.81, p = 0.431), the oral cancer group (T vs. C: OR = 1.56, 95% CI = 1.22-1.99, p = 0.267; TT/TC vs. CC: OR = 1.69, 95% CI = 1.26-2.25, p = 0.242; TC vs. CC: OR = 1.65, 95% CI = 1.24-2.18, p = 0.295), and the esophageal cancer group (T vs. C: OR = 1.30, 95% CI = 1.07-1.58, p = 0.320), the FPRP values were lower than 0.2, and the results were stable and reliable. It is worth noting that although the association did not have statistical significance for hepatocellular carcinoma, the results for all genetic models showed a trend of reduced risks.
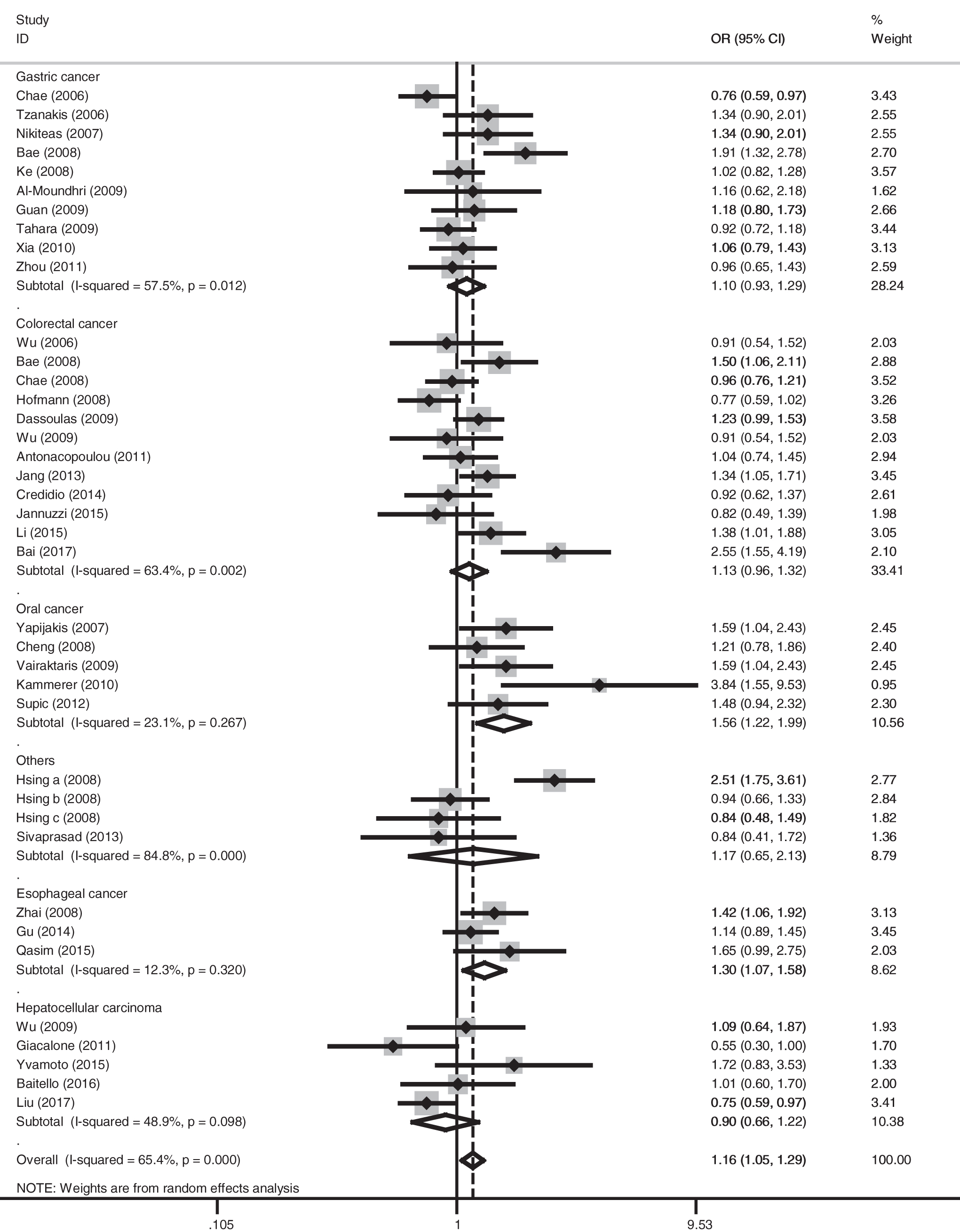
The forest plot of the association between the VEGF +936C>T gene polymorphism and digestive system cancer susceptibility in the allele model (T vs. C) for different cancer types. The squares and horizontal lines correspond to the study-specific ORs and 95% CIs. The size of the square reflects the weight of each study and the diamonds indicate the overall estimate or pooled ORs in subgroups with their corresponding 95% CIs.
The stratified analysis results based on the sources of the control groups showed that studies with controls drawn from community populations had significant combined effect sizes for digestive system cancer in the meta-analysis (T vs. C: OR = 1.18, 95% CI = 1.05-1.33, p < 0.001; TT/TC vs. CC: OR = 1.21, 95% CI = 1.04-1.41, p < 0.001; TT vs. CC/TC: OR = 1.23, 95% CI = 1.03-1.47, p = 0.657; TT vs. CC: OR = 1.33, 95% CI = 1.11-1.60, p = 0.672; TC vs. CC: OR = 1.20, 95% CI = 1.02-1.42, p < 0.001). In addition, the FPRP values in the T versus C model (FPRP-0.113) and the TT versus CC model (FPRP = 0.050) in community populations were lower than 0.2, indicating that the association was noteworthy. All the genetic models in studies with controls drawn from hospital populations did not show significant associations.
Finally, the stratified analysis was performed based on different genotyping methods. The meta-analysis results showed that in studies using the PCR-RFLP genotyping methods, the VEGF +936C>T gene polymorphism and the increase of the risk of digestive system cancer had a significant association (T vs. C: OR = 1.18, 95% CI = 1.05-1.34, p < 0.001; TT/TC vs. CC: OR = 1.20, 95% CI = 1.04-1.39, p < 0.001; TT vs. CC/TC: OR = 1.23, 95% CI = 1.02-1.50, p = 0.553; TT vs. CC: OR = 1.34, 95% CI = 1.10-1.64, p = 0.424; TC vs. CC: OR = 1.18, 95% CI = 1.02-1.35, p = 0.00). The FPRP values in the T versus C model (FPRP = 0.169) and the TT versus CC model (FPRP = 0.090) were lower than 0.2, indicating that the association was noteworthy. There was no significant association for genotyping methods using TaqMan and other technologies.
Sensitivity analysis and cumulative meta-analysis
For the sensitivity analysis, each study on VEGF +936C>T and the risk of developing digestive system cancer was excluded one by one, and the meta-analysis was reperformed. The pooled results did not change significantly, indicating that the results were stable and reliable (Fig. 4). A cumulative meta-analysis was performed based on the order of the studies' publication years. With the increase of the number of studies, the combined effect sizes and their CIs tended to be stable and had better change trends (Fig. 5).
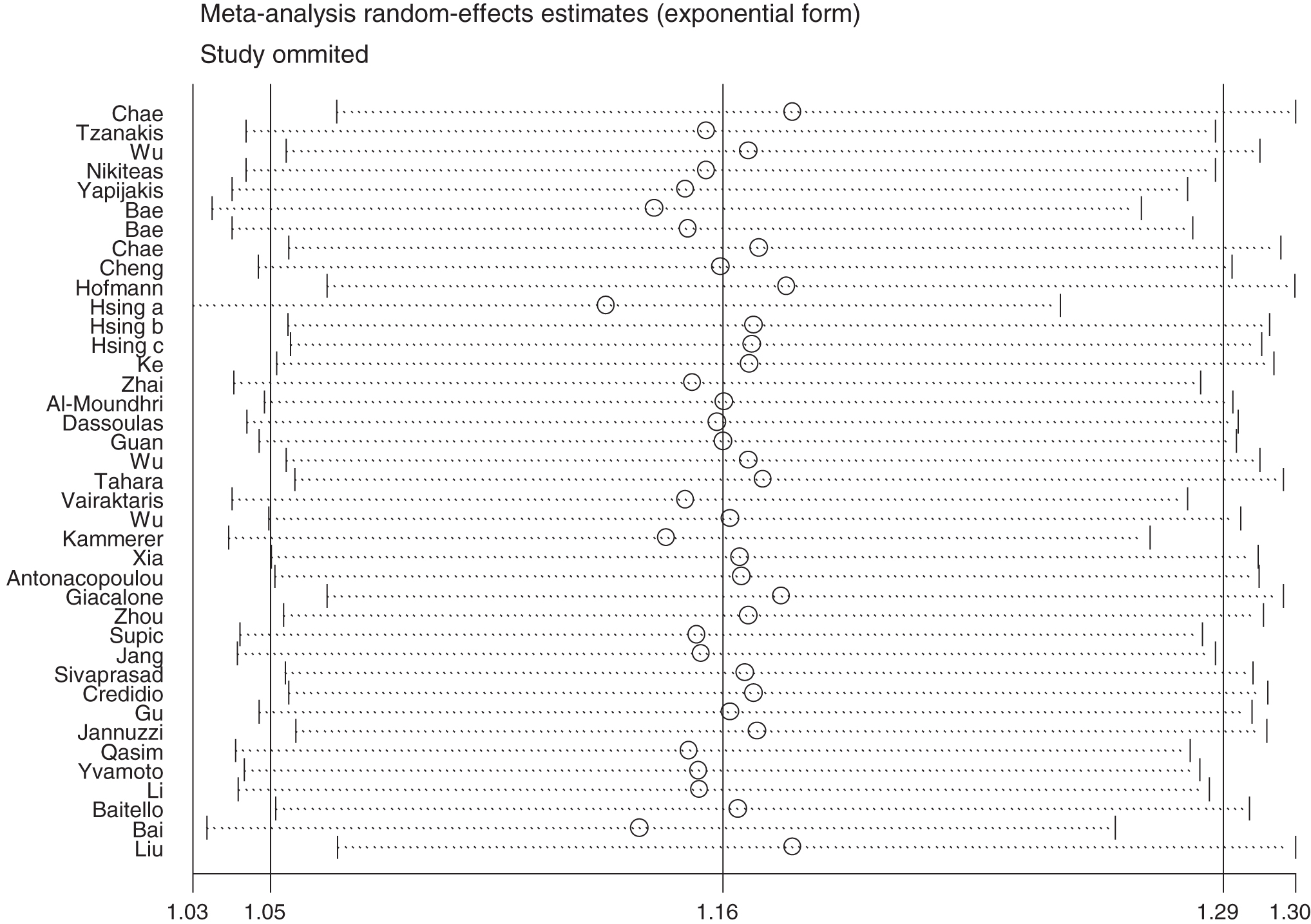
Effect of each single study on the overall combined OR in the allele model (T vs. C). The points and the horizontal lines represent the ORs and 95% CIs after omitting studies in turn.
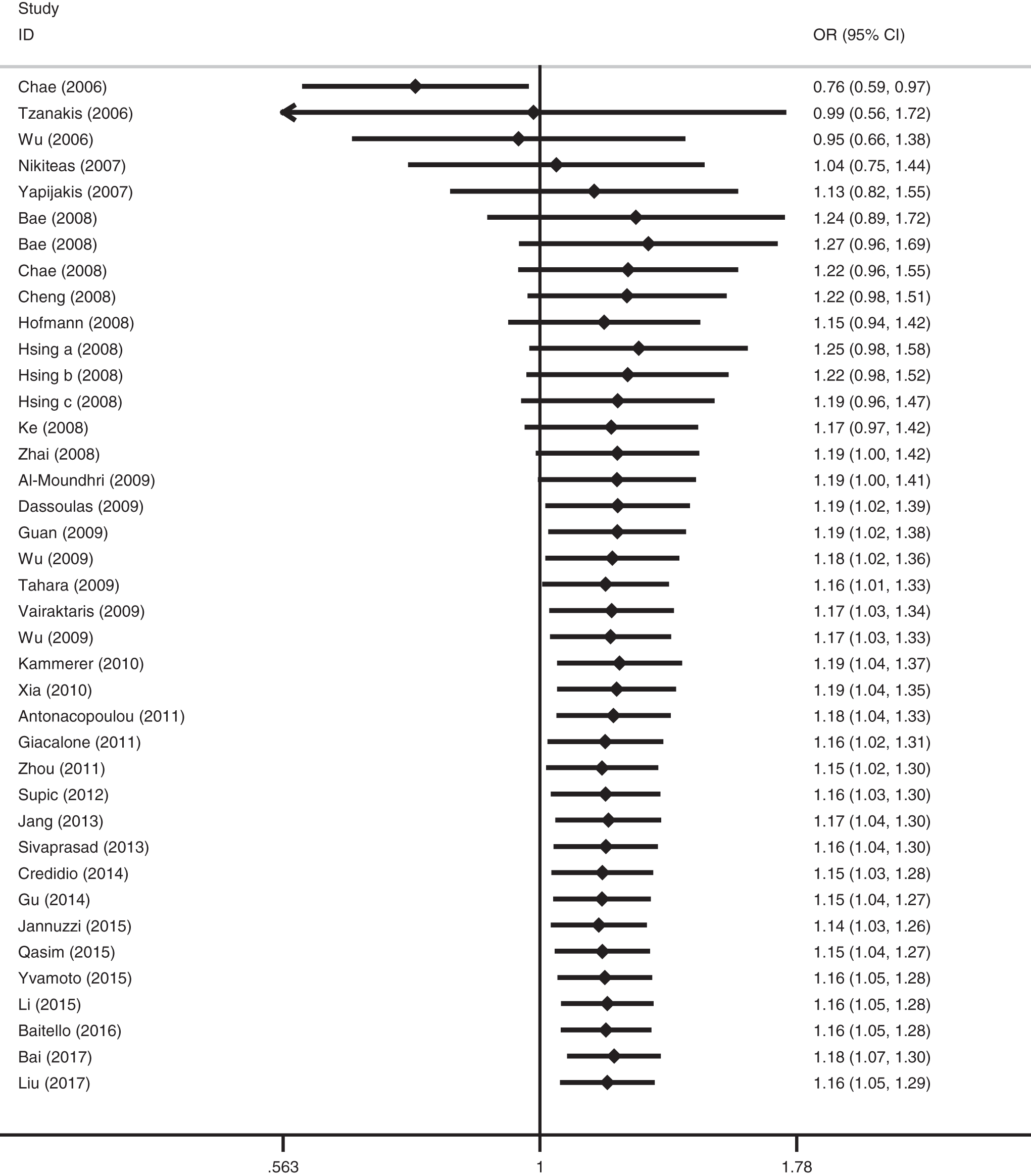
The cumulative meta-analysis of the association between the VEGF +936C>T polymorphism and digestive system cancer susceptibility in the allele model (T vs. C). The black squares indicate the cumulative ORs while the horizontal lines represent the 95% CIs.
Publication bias
A funnel plot analysis was performed to determine whether the included studies had publication bias. The results showed that the funnel plots of all genotypes were basically symmetric, indicating that the meta-analysis results did not have significant publication bias. In the allele model of the association between the VEGF +936C>T polymorphism and digestive system cancer, Begg's test had p = 0.432 and the Egger's test had p = 0.102. These results suggested that there was no significant publication bias (Fig. 6).

The Begg's funnel plot of the publication bias of the VEGF +936C>T allele model (T vs. C). Each point represents a separate study for the indicated association.
Discussion
The tumor microenvironment plays an important role in the development, progression, and metastasis of tumors. The division and growth of tumor cells require a large amount of nutrients; therefore, tumors show a large degree of irregular angiogenesis according to their location (Folkman, 1971; Kushner and Bautch, 2013). The growth and maturation of new blood vessels is the result of a complicated process involving multiple factors and multiple signal transduction pathways. In normal tissues, pro-VEGFs and anti-VEGFs are present together and maintain a relative balance. This balance allows the normal synthesis and differentiation of human vessels. Under conditions with tumor growth, irregular angiogenesis can easily form highly hypoxic areas. The low oxygen environment induces a surge in the number of pro-VEGFs (Safran and Kaelin, 2003). The function of pro-VEGFs far exceeds that of anti-VEGFs; therefore, a large number of vessels, mainly blood vessels, grow, providing an excellent growth environment for tumors.
It was recently discovered that VEGF and its receptor are closely associated with the development of digestive system cancer. Blocking or interference with the VEGF/VEGFR signal transduction pathway can effectively inhibit angiogenesis to control tumor growth. With the extensive application of antitumor drugs that use VEGF/VEGFR as the target (Takahashi, 2011; Sitohy et al., 2012), nucleotide polymorphism of VEGF and its receptor has become a research hotspot. Currently, there are an increasing number of studies on the association between malignant tumor susceptibility and VEGF gene sites, including -460C>T, -2489C>T, and -2578C>A in the promoter region, -634G>C and -7C>T in the 5′-UTR region, and +936C>T and 1612G>A in the 3′-UTR region. Further studies on these markers are expected to elucidate important information on the outcome of tumors and the treatment efficacy. Therefore, this study focused on the VEGF +936C>T allele and performed a meta-analysis to investigate the association between polymorphisms of this site and digestive system tumors.
A total of 37 articles met the inclusion criteria for this study, and 8568 patients and 10,870 controls were included. The study subjects were Asian in 17 articles and Caucasian in 20 articles. In the comparison of the VEGF +936C>T allele in five genetic models, the meta-analysis results all showed significantly increased combined OR values (T vs. C: OR = 1.16, 95% CI = 1.05-1.29, p < 0.001; TT/TC vs. CC: OR = 1.19, 95% CI = 1.05-1.34, p < 0.001; TT vs. CC/TC: OR = 1.19, 95% CI = 1.01-1.39, p = 0.397; TT vs. CC: OR = 1.27, 95% CI = 1.08-1.49, p = 0.297; TC vs. CC: OR = 1.18, 95% CI = 1.03-1.34, p < 0.001). The funnel plot analysis results for all models did not show significant publication bias. When the studies were excluded one by one, the combined effect size did not change significantly, and all studies increased the reliability of the association.
The conclusions of the included articles regarding the association between VEGF +936C>T polymorphism and digestive system cancer were not consistent. This inconsistency may have been caused by differences in genetic backgrounds, tumor types, sources of the control populations, and experimental methods. Therefore, this study performed a stratified analysis targeting the above factors. The stratified analysis was performed based on ethnicity. In the comparison of many genetic models, VEGF +936C>T polymorphism significantly increased the risk of digestive system tumors in the Caucasian population subgroup, whereas only the results of the allele model was significant in the Asian population subgroup. In the control groups of the Caucasian population subgroup and the Asian population subgroup, the minimum allele frequencies were 16.30% and 16.85%, respectively, and the difference did not have statistical significance (χ2 = 1.028, p = 0.311). Therefore, the differences in the risk of developing cancer in different populations might be caused by environmental factors. The stratified analysis results based on tumor type indicated that the VEGF +936C>T polymorphism had a clear association with susceptibility to colorectal cancer, oral cancer, and esophageal cancer. The results based on FPRP showed that the comparison of different genetic models of these three cancers all had FPRP values <0.2, indicating that the association was true and reliable. This study did not identify an association between the +936C>T polymorphism and gastric cancer or hepatocellular carcinoma. Interestingly, this site may be associated with a reduced trend in the risk of hepatocellular carcinoma. This result indicated that the VEGF +936C>T allele plays different roles in different tissues and that it might change the risk of developing digestive system tumors through gene-gene and gene-environment interactions. Its carcinogenesis still requires further studies. The stratified analysis results based on the sources of control populations showed that the COX-2-1195G>A gene polymorphism in the community population subgroup could significantly increase the risk of digestive system cancer, whereas the risk in the hospital populations was not significant. The presence of other diseases and the use of drugs in the hospital population might have some influence on the genotype detection results; therefore, the community population is more representative than control samples from hospitals. When selecting control individuals, community populations should be used whenever possible. Furthermore, we performed the stratified analysis based on genotyping methods. The results showed that the statistical results among different subgroups had significant differences. Therefore, we speculated that different detection methods might also influence genotyping results.
Although this study was reasonably designed and strictly implemented, there are still some limitations. First, the overall comparison of the allele model, the dominant model, and the heterozygous model showed that there was significant heterogeneity among all studies. The presence of heterogeneity might have influences on the interpretation of the results. When ethnicity, tumor type, sources of the control group populations, and genotyping methods were used for stratified analyses, heterogeneity was only partially reduced or eliminated for the hepatocellular carcinoma, oral cancer, and esophageal cancer subgroups. This study also showed that heterogeneity was not caused by one single study and that other unknown factors might be the real source of heterogeneity. Second, this study was a meta-analysis based on original data from the included articles. Unreasonable data and possible potential confounding factors in the original studies could not be corrected. Because digestive system tumors are influenced by many factors, future comprehensive studies and analyses should combine factors such as age, sex, occupation, eating habits, and environmental exposure. Third, the sample size of included studies was relatively small; in particular, the test performance of subgroups might be insufficient to determine whether significant associations were truly present. Therefore, the meta-analysis results should be interpreted carefully. Finally, this study only included articles published in Chinese or English. Articles published in other languages or articles that were not published because of negative results could not be obtained. Therefore, there might be a certain degree of publication bias.
Conclusion
In summary, this meta-analysis indicated that the VEGF +936C>T gene polymorphism and digestive system cancer susceptibility had a significant association. Carriers with T on this site were more susceptible to digestive system tumors, especially colorectal cancer, oral cancer, and esophageal cancer. The meta-analysis results provide evidence for further epidemiological studies to elucidate the role of the potential gene-gene or gene-environment interaction in the development of digestive system tumors.
Footnotes
Authors' Contributions
Conception and design: C.F. and P.Y.; Acquisition of data: C.F., P.L., and F.Z.; Analysis and interpretation of data: C.F. and P.L.; Writing, review, and/or revision of the article: F.Z. and H.C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.