
Abstract
Aims:
Previous studies have have reported inconsistent results regarding the association of the XRCC1 polymorphism Arg399Gln with oral leukoplakia (OLK) risk. This study was designed to assess the existing evidence of this association using a meta-analytic approach.
Materials and Methods:
The literature was searched using multiple databases, including PubMed, EMBASE, and China National Knowledge Infrastructure (CNKI), through October 22, 2020. Crude odds ratios (ORs) with 95% confidence intervals (CIs) were used to evaluate the strength of any associations.
Results:
A total of 671 Indian cases and 1009 Indian controls from seven case-control studies were included in the meta-analysis. The overall analysis revealed that the AA genotype was associated with a significantly increased OLK risk compared with the GG+GA genotypes (OR = 1.51, 95% CI = 1.10-2.06). In the subgroup analysis stratified by tobacco use, a significant association was found in the mixed group (OR = 1.51, 95% CI = 1.12-2.56), but not in the tobacco-using group or the no tobacco use group. In the OLK subtype subgroup analysis, a significantly increased risk was found in the hyperplastic subgroup (OR = 5.01, 95% CI = 1.39-18.11), whereas no associations were found in the dysplastic or mixed subgroups.
Conclusions:
The results of this meta-analysis suggest that the XRCC1 Arg399Gln polymorphism may significantly contribute to susceptibility to OLK in the Indian population.
Introduction
Oral leukoplakia (OLK) is a condition in which one or more white patches or spots form inside the mouth. The World Health Organization defines OLK as a potentially malignant disorder (Warnakulasuriya et al., 2007). Globally, the pooled prevalence of OLK is 1.5-2.6% with no gender predilection (Petti, 2003). The malignant transformation rate of OLK is ∼3.5% (Dong et al., 2019). OLK is a complex condition caused by environmental and genetic factors. Multiple environmental variables related to OLK development have been identified, including chronic irritation, human papillomavirus infection, tobacco smoking, heavy alcohol consumption, betel nut chewing, and poor oral hygiene (Arduino et al., 2013). However, the underlying genetic basis remains largely unknown.
The development of oral premalignant lesions has been linked to a reduction in DNA repair capacity (Thomas et al., 2020). Hereditary genetic factors are known to influence an individual's DNA repair capacity. The X-ray repair cross-complementing group 1 (XRCC1) gene is an important member of the base excision repair system pathway that repairs single-strand DNA breaks. XRCC1 Arg399Gln (rs25487) is one of the most studied polymorphisms of XRCC1 (Hoseini et al., 2021). Arg399Gln is a nonsynonymous polymorphism located in the coding region of XRCC1. This variant causes an amino acid substitution in the BRCT domain of XRCC1 that can affect the function of XRCC1 protein, resulting in reduced DNA repair capacity (Masson et al., 1998).
Many studies have investigated the relationship of this polymorphism with OLK risk; however, the results have been inconsistent or even contradictory (Majumder et al., 2005, 2007; Ramachandran et al., 2006; Yadav et al., 2009; Mahimkar et al., 2010; Anantharaman et al., 2011). To obtain a comprehensive understanding of this relationship, we performed a meta-analysis to investigate the association between XRCC1 Arg399Gln and risk of OLK.
Materials and Methods
Publication search
A comprehensive literature search was conducted using PubMed, EMBASE, and China National Knowledge Infrastructure (CNKI) for studies reported up to October 22, 2020. Two reviewers identified articles evaluating the association of OLK risk and XRCC1 polymorphisms. The following search terms were used: (X-Ray repair cross-complementing 1 or XRCC1) and (oral leukoplakia or OLK) and (polymorphism or variant or mutation). Studies included in the meta-analysis met the following criteria: (1) investigation of polymorphisms of XRCC1 and OLK risk; (2) use of a case-control design with unrelated participants; (3) all patients must conform to the diagnostic criteria of OLK (van der Waal et al., 1997); and (4) sufficient genotype distributions of cases and controls to assess an odds ratio (OR) with a 95% confidence interval (CI).
Data extraction
Two reviewers independently extracted data from the identified studies and reached a consensus through consultation. The following information was extracted from each study: author, publication year, country, ethnicity, tobacco use history, OLK subtype, number of cases and controls, source of control groups, and genotyping method.
The Newcastle-Ottawa Scale (NOS) criteria were used to assess the methodological quality of the included studies. The NOS criteria include three aspects: (1) subject selection, scored 0-4; (2) comparability of subject, scored 0-2; and (3) clinical outcome, scored 0-3. NOS scores thus range from 0 to 9, with a score ≥7 indicating good quality.
Statistical analysis
The strength of association between XRCC1 polymorphisms and OLK risk was estimated using the OR and 95% CI. The statistical significance of the combined OR was determined using the Z-test. Stratification analyses were performed by OLK subtypes and tobacco use. Heterogeneity was evaluated by the χ2-based Q statistic. When the p-value was >0.05, a fixed-effects model was used; otherwise, a random-effects model was used (Dai et al., 2015). Statistical significance of the OR was determined using the Z-test, with p < 0.05 judged to be statistically significant.
Publication bias was visually assessed using Begg's funnel plot and the degree of asymmetry was assessed by Egger's test (Xie et al., 2014). A sensitivity analysis was performed to assess the stability of the meta-analysis by sequentially excluding each case-control study (Dai et al., 2015). All statistical analyses were performed using STATA11.0 (Stata Corporation, College Station, TX).
Results
Meta-analyses database
After the initial screening, 10 relevant publications were identified that met the search criteria. Two publications were excluded for not being relevant to XRCC1 genotype and OLK risk and three publications were excluded for not providing detailed genotype data. Ultimately, our meta-analysis data set consisted of seven case-control studies from five publications (Fig. 1). All of these studies were conducted in Indian populations. Genotyping method was polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) analysis. OLK subtype was confirmed histologically in all of the studies. The genotype distributions among controls were all in agreement with Hardy-Weinberg equilibrium.
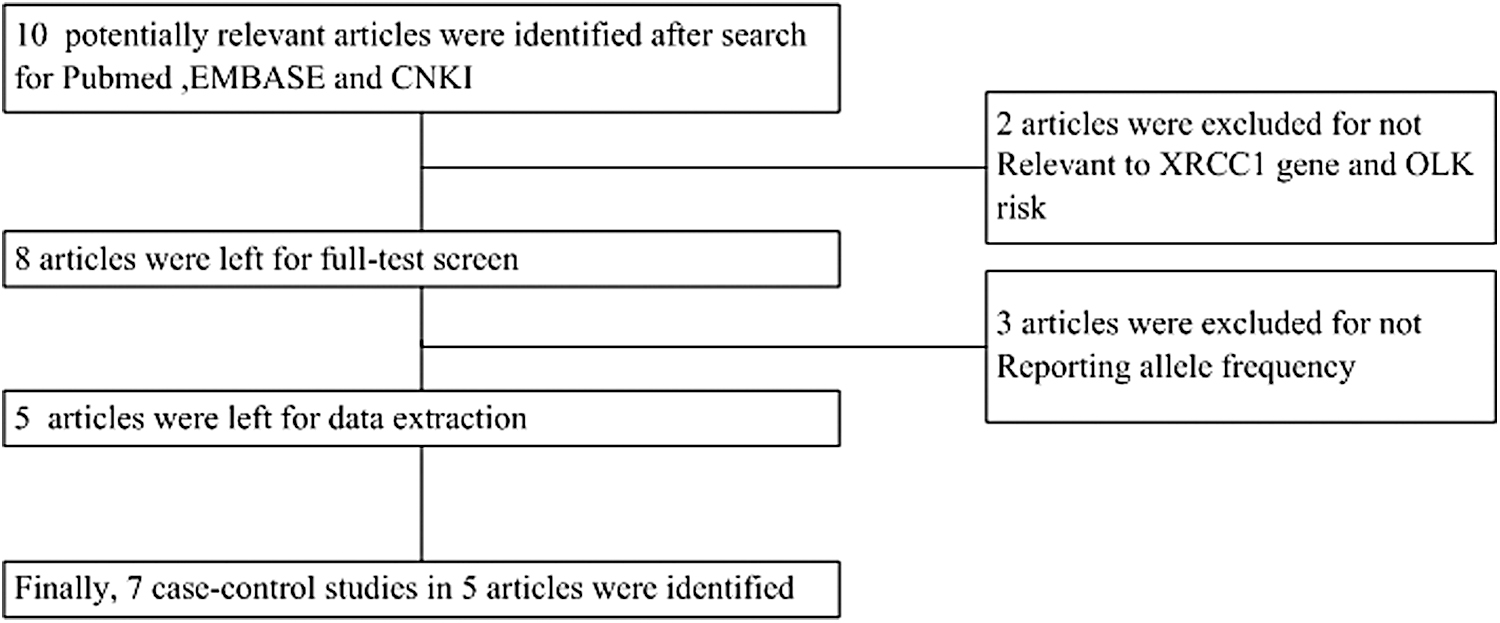
Flow diagram of the included/excluded studies.
Finally, 671 cases and 1009 controls from seven case-control studies were included in the analysis. All the included case-control studies had NOS scores ≥7 (Tables 1 and 2).
Characteristics of the Populations and Cancer Types of the Studies Included in the Meta-Analysis
Mixed means samples contain both users and nonusers.
HB, hospital based; HWE, Hardy-Weinberg equilibrium; ND, no data; NOS, Newcastle-Ottawa Scale; PB, public based; PCR, polymerase chain reaction; RFLP, restriction fragment length polymorphism.
Distribution of XRCC1 Arg399Gln Genotypes and Alleles Among Oral Leukoplakia Patients and Controls
Quantitative data synthesis
Overall analyses
As shown in Figure 2, the heterogeneity of AA versus GG+GA for all seven case-control studies was assessed and the p-value was 0.16, suggesting the absence of heterogeneity. Thus, a fixed-effects model was used to assess the data. The combined OR was 1.51 (95% CI = 1.10-2.06), and the test for the overall effect had a Z-value of 2.56 (p = 0.01). This result suggests that people with the AA genotype of Arg399Gln had a 51% increased risk of OLK relative to those with the G allele (GG and GA genotypes). The summary results of other genetic comparisons are listed in Table 3.
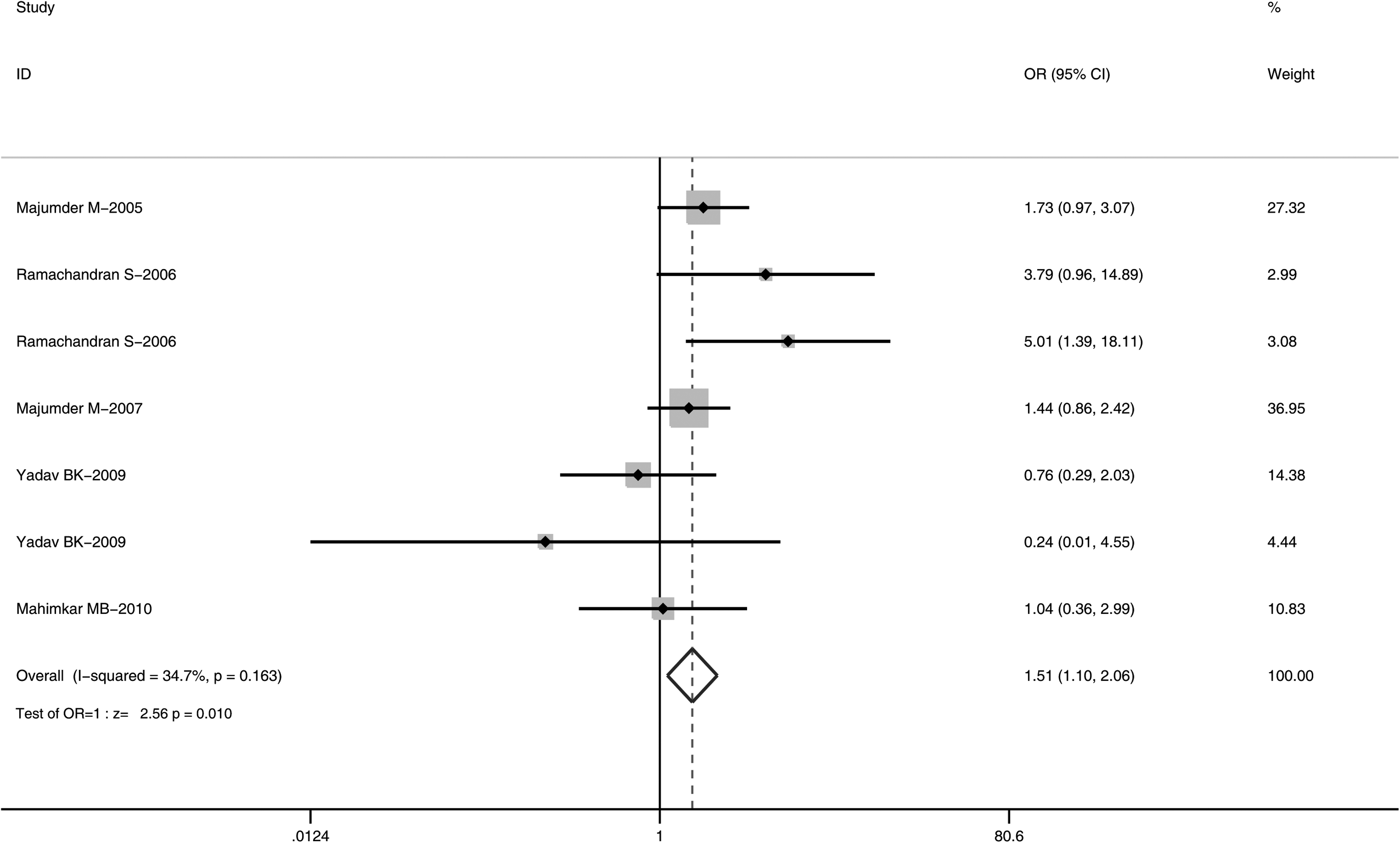
Meta-analysis using a fixed-effects model to test the association between OLK risk and XRCC1 Arg399Gln polymorphisms (AA vs. GA+GG). OLK, oral leukoplakia.
Summary of Different Comparative Results
Bold values mean the result is positive and the relationship is statistically significant.
p-Value of the Q test for heterogeneity test. A fixed-effects model was used when the p-value for the heterogeneity test was ≥0.05; otherwise, a random-effects model was used.
Subgroup analyses
Subgroup analyses were performed according to tobacco use history and OLK subtype. Subgroup analyses by tobacco use under a recessive model are shown in Figure 3. A significant association was found in the mixed group (OR = 1.51, 95% CI = 1.12-2.56), but not in the tobacco use group (OR = 1.40, 95% CI = 0.85-2.30) or no tobacco use group (OR = 0.24, 95% CI = 0.01-4.55).
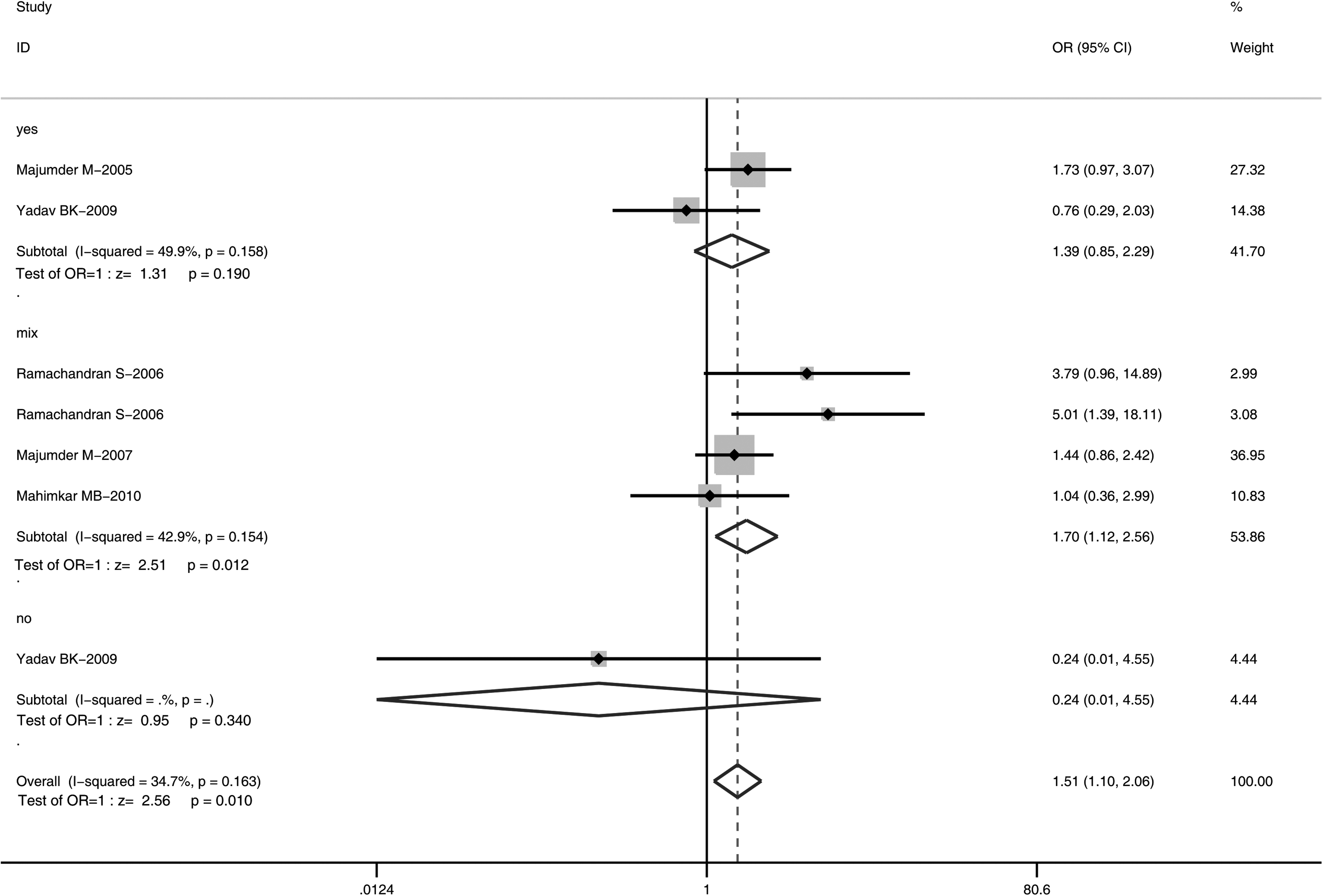
Meta-analysis using a fixed-effects model to test the association between OLK risk and XRCC1 Arg399Gln polymorphisms (AA vs. GA+GG): subgroup analysis by tobacco use.
When stratifying by OLK subtype (Fig. 4), a significantly increased risk was found in the hyperplastic subgroup (OR = 5.01, 95% CI = 1.39-18.11), whereas no association was found in the dysplastic subgroup (OR = 3.79, 95% CI = 0.96-14.89) or the mixed subgroup (OR = 1.32, 95% CI = 0.94-1.84).
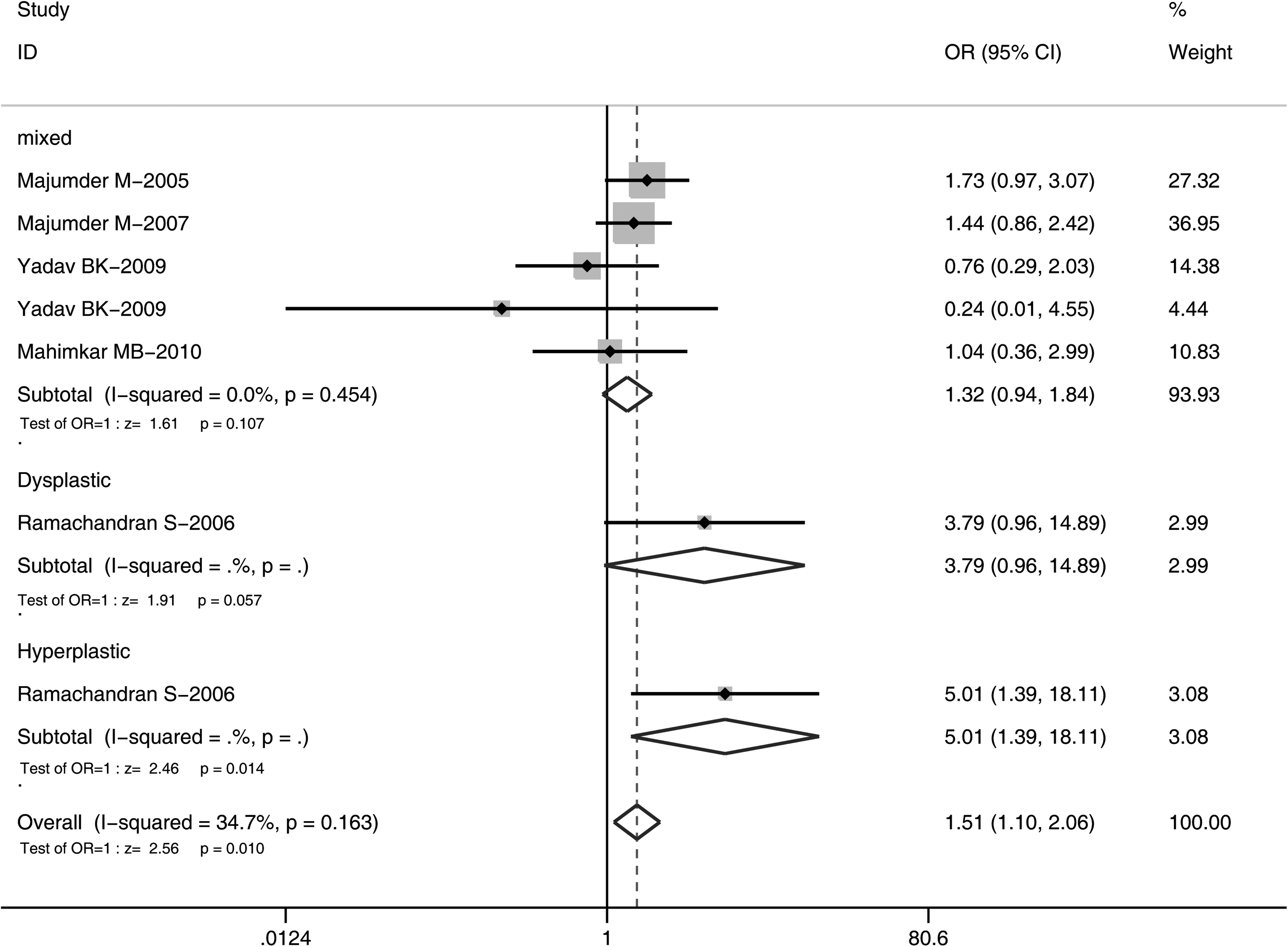
Meta-analysis using a fixed-effects model to test the association between OLK risk and XRCC1 Arg399Gln polymorphisms (AA vs. GA+GG): subgroup analysis according to OLK subtype.
Sensitivity analysis
As shown in Figure 5, similar combined ORs were obtained after sequentially excluding each case-control study from overall analysis, suggesting the stability of the results.
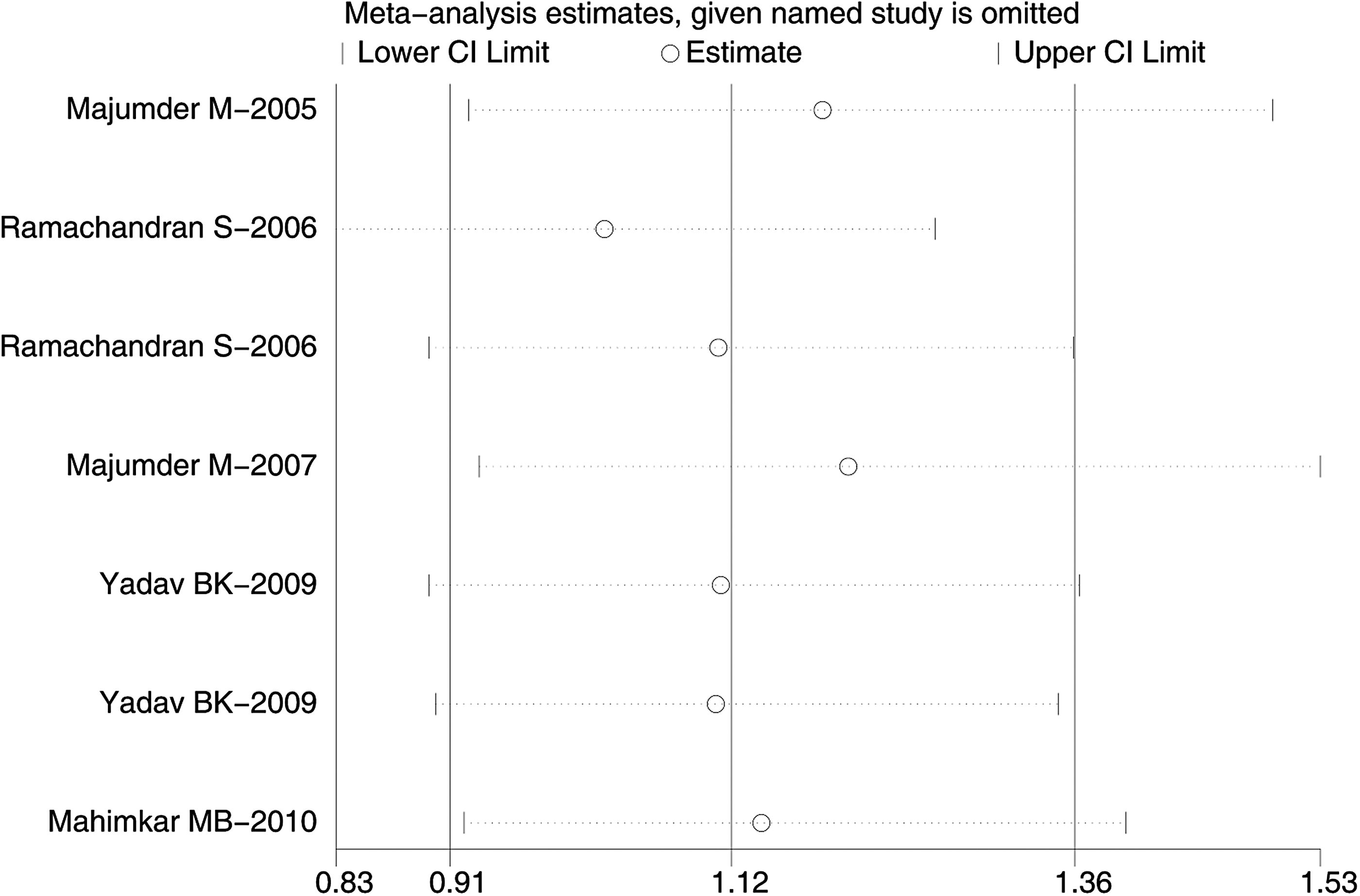
Sensitivity analysis of the summary OR coefficients of the relationships between XRCC1 Arg399Gln polymorphisms and the risk of OLK.
Publication bias
Publication bias was evaluated using Begg's funnel plot and Egger's test. The shapes of the funnel plots did not show obvious asymmetry (Fig. 6). The results of Egger's test also indicated a lack of publication bias (p = 0.17).
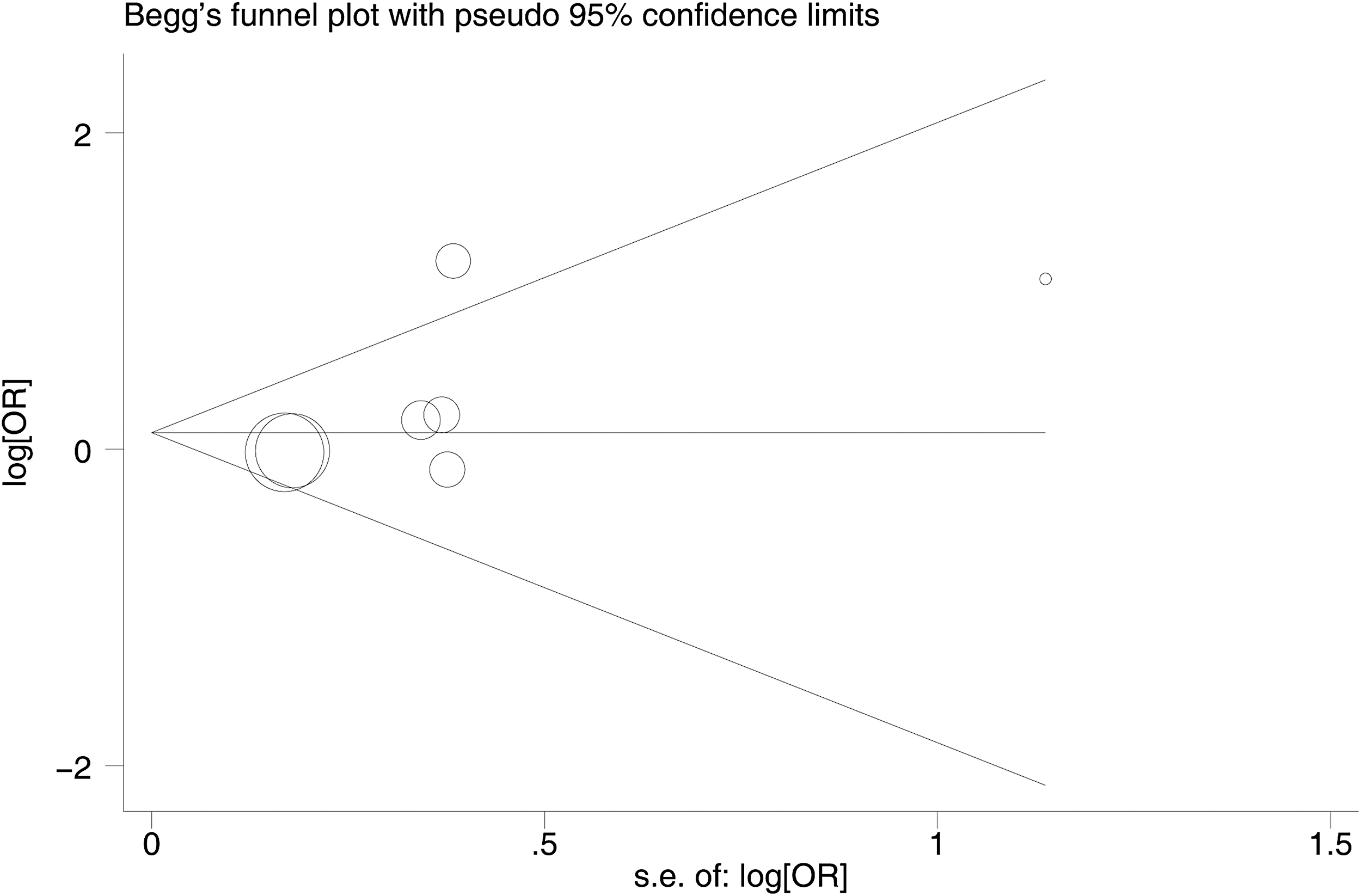
Begg's funnel plot for publication bias in the selection of studies on XRCC1 Arg399Gln polymorphisms (AA vs. GA+GG).
Discussion
OLK is associated with an increased risk of oral squamous cell carcinoma (Schepman et al., 1998). In recent years, an increasing number of studies have investigated genetic susceptibility to OLK (Roy et al., 2014). The XRCC1 gene plays an important role in fixing base damage and DNA single-strand breaks caused by alkylating agents and ionizing radiation (Mok et al., 2019). Arg399Gln (rs25487) is one of the most commonly studied polymorphisms of the XRCC1 gene, as it might interact with environmental factors to influence the development of OLK. Although numerous studies have investigated the association between Arg399Gln polymorphisms and OLK risk, the results remain inconclusive and contradictory (Majumder et al., 2005, 2007, 2009; Ramachandran et al., 2006; Yadav et al., 2009; Mahimkar et al., 2010; Anantharaman et al., 2011). To derive a more precise conclusion, we performed a comprehensive meta-analysis to explore the association between risk of OLK and XRCC1 Arg399Gln.
This meta-analysis incorporated seven cases-control studies involving 671 OLK cases and 1009 controls concerning Arg399Gln in XRCC1. Overall, we found that AA homozygotes were associated with an increased risk of OLK compared with GG/GA carriers under a recessive model (OR = 1.51, 95% CI = 1.10-2.06). The amino acid substitution caused by Arg399Gln can disrupt the function of XRCC1, resulting in a reduced DNA repair capacity. This reduction may increase susceptibility to the development of cellular diseases such as leukoplakia and cancer.
In our meta-analysis, we carried out subgroup analyses for tobacco use history and leukoplakia subtypes. The results showed that, in the mixed tobacco use group, AA homozygotes were associated with an increased risk of OLK relative to GG/GA carriers under a recessive model. As for the leukoplakia subtypes, we found a significant association between OLK risk and Arg399Gln polymorphisms in the hyperplastic subgroup but not in the dysplastic or mixed subgroups.
Heterogeneity is an important issue when performing a meta-analysis. There was no heterogeneity in the overall comparisons in the recessive model. Heterogeneity was not significant for any of the subgroups stratified by OLK subtype and tobacco use history. Similarly, publication bias is an important issue. In this meta-analysis, we showed no significant publication bias using Begg's funnel plots and Egger's test, indicating the reliability of our results.
There are several limitations of this meta-analysis. First, we only searched for publications in PubMed, EMBASE, and CNKI databases. It is possible that we may have missed some relevant publications in other databases. Second, although significant publication bias was not found in our meta-analysis, it is possible that there are unpublished results. Third, in the subgroup analysis, the case-control number of some subgroups was small, which could result in low statistical power to reveal reliable associations. Finally, all participants in this meta-analysis were Indian. Thus, possible ethnic differences in the association of XRCC1 polymorphisms with OLK should be investigated and more studies involving other ethnicities are needed.
Conclusions
In conclusion, our meta-analysis suggests that the substitution of G to A of XRCC1 Arg399Gln polymorphism is a risk factor of OLK, especially for the hyperplastic subgroup and mixed tobacco use subgroup. In the future, well-designed case-control studies should be conducted to validate these findings in diverse populations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from National Science and Technology Major Projects for “Major New Drugs Innovation and Development” (Grant Nos. 2018ZX09201014, 2017ZX09304028, and 2017ZX09101001), China Postdoctoral Science Foundation (Grant No. 2019M650390), the National Key R&D Program of China (Grant No. 2016YFC0904900), National Natural Science Foundation of China (Grant Nos. 81872940, 81973395, and 82073935), and Beijing Natural Science Foundation (Grant No. 7171012).