
Abstract
Study Design:
Prospective observational cohort study.
Objective:
To determine whether biofilms exist on spinal instrumentation recovered during revision surgery in which microbial cultures were negative.
Background:
Biofilm bacteria are extremely difficult to detect by conventional culture methods used in the standard hospital setting. Chronic infections in which bacteria form biofilms have been demonstrated to slow healing and prevent bony fusion. These slime encased microbial communities serve to isolate the bacteria from the body's immune responses, while simultaneously providing metabolic resistance to antimicrobial therapy.
Methods:
Traditional debridement wound cultures were taken from each specimen and sent for microbiological analyses. Bacterial DNA testing was performed using polymerase chain reaction (PCR) electrospray ionization-mass spectrometry (ESI-MS). Based on the PCR/ESI-MS results, specific crossed immune electrophoresis was used to detect the bacterial species within biofilms observed on the removed instrumentation. In addition, fluorescent in situ hybridization (FISH) probes corresponding to the bacterial species identified by PCR/ESI-MS were used with confocal microscopy to visualize and confirm the infecting bacteria.
Results:
Fifteen patients presented for surgical revision of thoracolumbar spinal implantation: four for clinical suspicion of infection, six for adjacent segment disease (ASD), one with ASD and pseudoarthrosis (PA), three with PA, and one for pain. Infections were confirmed with PCR/ESI-MS for all four patients who presented with clinical infection, and for five of the patients for whom infection was not clinically suspected. Of the presumed non-infected implants, 50% demonstrated the presence of infectious biofilms. Half of the revisions due to pseudoarthrosis were shown to harbour biofilms. The revisions that were performed for pain demonstrated robust biofilms but did not grow bacteria on traditional culture media.
Conclusions:
Culture is inadequate as a diagnostic modality to detect indolent/subclinical biofilm infections of spinal instrumentation. The PCR/ESI-MS results for bacterial detection were confirmed using species-specific microscopic techniques for both bacterial nucleic acids and antigens. Biofilms may contribute to pseudoarthrosis and back pain in postoperative wounds otherwise considered sterile.
Introduction
Recent literature indicating the bacteria can form multicellular biofilms that escape immune surveillance and are often not detected through traditional culture mediums has created a paradigm shift with regard to our understanding of chronic infection, particularly in association with surgically implanted devices (Ehrlich et al, 2005, 2010, 2014; Kathju et al, 2009; Stoodley et al, 2005, 2011; Wolcott and Ehrlich, 2008). This understanding grew out of a convergence of molecular diagnostics (MDx), the recognition of genomic plasticity within a microbial species, and the inadequacy of cultural techniques to detect the multiple pathogens associated with polyclonal and polymicrobial infections (Aul et al, 1998; Marshall et al, 1997; Nickel et al, 2015; Palmer et al, 2014, 2016, 2022; Post et al, 1996; Shen et al, 2005a, 2005b).
Biofilms are complex multicellular bacterial aggregates that reside within a self-produced protective matrix that adhere to both living and abiotic surfaces. This self-protective nature allows the resident bacteria to survive the host's defenses, including the adaptive immune response. The bacteria deep within the biofilm are metabolically quiescent, enabling them to persist for extended periods of time, even in the presence of antibiotics (Borriello et al, 2004; Ehrlich et al, 2005, 2010, 2014; Hall Stoodley et al, 2008; Høiby et al, 2011; Kathju et al, 2009; Palmer et al, 2014, 2022; Stoodley et al, 2005, 2011; Wolcott and Ehrlich, 2008; Wolcott et al, 2008). Mature biofilms are also capable of producing planktonic showers, which can then seed new sites of focal biofilm infections (Borriello et al, 2004; Ehrlich et al, 2005, 2010, 2014; Kathju et al, 2009; Palmer et al, 2014, 2022; Stoodley et al, 2011; Wolcott and Ehrlich 2008; Wolcott et al, 2008).
Biofilm bacteria have been linked to many types of chronic infections that often have high morbidity and mortality rates (Wolcott and Ehrlich, 2008). These infections often cannot be eradicated with antibiotics, and if they can, require much higher concentrations of antibiotics than infections from free-floating bacteria, due to the triggering of the bacterial stringent response deep within the biofilm that results in the formation of persister cells (Borriello et al, 2004; Ehrlich et al, 2005, 2010, 2014; Hall-Stoodley et al, 2008; Høiby et al, 2011; Kathju et al, 2009; Nelson et al, 2005; Palmer et al, 2014, 2022; Schaudinn et al, 2007; Stoodley et al, 2005, 2011; Wolcott and Ehrlich, 2008).
This bacterial persistence poses a significant risk for postoperative care. This is particularly true for surgical implants, which if they become infected often require additional surgery (Borriello et al, 2004; Ehrlich et al, 2005, 2010, 2014; Hall-Stoodley et al, 2008; Jacovides et al 2012; Kathju et al, 2009; Nelson et al, 2005; Palmer et al, 2014, 2022; Stoodley et al, 2005, 2011; Wolcott and Ehrlich, 2008; Zimmerli, 2014).
Additional reasons for revision surgery include pseudoarthroses that cause instability and/or pain. Some authors have postulated that this form of delayed healing may also be due to indolent bacteria (Ehrlich et al, 2005, 2014). In such cases, intraoperative cultures are often negative when biofilms are present whether or not there is clinical suspicion of infection. This is because the bacteria in a biofilm are metabolically quiescent and require specific stimuli to resume division (Borriello et al, 2004; Ehrlich et al, 2005, 2010, 2014; Jacovides et al, 2012; Nelson et al, 2005; Palmer et al, 2014; Stoodley et al, 2011; Zimmerli, 2014). Standard hospital microbial detection procedures include the use of culture media to test for the presence of bacteria.
However, planktonic bacteria are often needed for a positive culture on agar or in broth, thus intraoperative swabs sent to clinical microbiology laboratories that do not perform MDx have a very low likelihood of being able to detect biofilm bacteria (Ehrlich et al, 2005, 2010, 2014; Jacovides et al, 2012; Kathju et al, 2009; Nelson et al, 2005; Palmer et al, 2014, 2022; Stoodley et al, 2005, 2011; Wolcott and Ehrlich, 2008). Recent studies have demonstrated that polymerase chain reaction (PCR)-based methods have a greater sensitivity for bacterial detection than culture media (Jacovides et al, 2012; Palmer et al, 2014, 2016, 2022; Nelson et al, 2005). This leads to the possibility that an undiagnosed biofilm presence may contribute to the need for additional surgery.
Swabs of failed implant surgery may remain culture-negative for the presence of bacteria, which may be due to undetected biofilms affording these sessile bacteria the ability of to remain near dormancy. This suggests that biofilms may still be present despite an absence of signs and symptoms of what most surgeons consider a clinical infection (Borriello et al, 2004, 2006; Ehrlich et al, 2005, 2010, 2014; Hall-Stoodley et al, 2008; Ho et al, 2003; Høiby et al, 2011; Jacovides et al, 2012; Kathju et al, 2009; Nelson et al, 2005; Palmer et al, 2014, 2016; Stoodley et al, 2005, 2011; Wolcott and Ehrlich, 2008; Zimmerli, 2014). Bacterial biofilms may be present on instrumentation otherwise considered sterile. Through molecular methods, including PCR-based methods, direct confocal microscopy, and crossed immune electrophoresis with immunofluorescence and fluorescent in situ hybridization (FISH), bacteria which would otherwise escape detection utilizing older “swab” methods can be identified (Nistico et al, 2009; Palmer et al, 2014, 2016; Stoodley et al, 2011).
Materials and Methods
This protocol was approved by the Allegheny General Hospital Internal Institutional Review Board, RC5433. All of the authors of this article have no conflict of interest to report, and have made significant contributions to the development, data analysis, and writing/editing of this article. The PCR/electrospray ionization mass spectrometry (ESI-MS) system was used in this study is an unlicensed instrument. All spinal implants used in this analysis were Food and Drug Administration approved.
Implant removal and specimen processing protocol
Spinal implants were removed intraoperatively during revision surgeries and handled with sterile technique. Only one person (D.T.A.) handled all implants using sterile instruments as grasping tools to handle the explants. Implants were immediately swabbed for microbial culture making sure to include visible adherent biological material in the swab. The implants were then placed in a sterile containers and sent for analyses to the MDx laboratory. Upon receipt in the MDx laboratory specimens (both the implant hardware and tissue excised from the explant) were fixed in 4% paraformaldehyde (Electron Microscopy Sciences) in 3 × phosphate buffered saline (PBS) for 12 h at 4°C and then washed three times with PBS. The buffer was removed and then replaced with a 50% PBS 50% ethanol solution and stored at −20°C before staining.
Microbial culture
Wound specimens were collected intraoperatively as described (Palmer et al, 2016) using a minimum of two swabs to sample the immediate area surrounding the explanted hardware. After sampling the deepest portion of the wound, the swabs were replaced into the holder, placed into a biohazard bag, and transported immediately to the onsite clinical microbiology laboratory. If a tissue sample was taken at the same time, it was collected in a sterile container, placed in a biohazard bag, and transported immediately to the onsite clinical microbiology laboratory for processing.
Routine wound swabs were used to inoculate blood agar plates, chocolate agar plates, MacConkey agar plates, and Columbia-colistin-nalidixic acid agar. In addition, a Gram-stain was made by rolling the other swab on a glass slide to make a thin film. The agar plates were then incubated in 5% carbon dioxide (CO2) at 35°C. The tissue samples collected for culture and Gram-stain were first cut with a sterile scalpel to make a touch prep. The rest of the tissue was lysed in a sterile disposable tissue grinder and aliquots of the lysate were used to inoculate a set of agar plates as described earlier, as well as being used to inoculate a tube of thioglycolate media (THIO). All incubations were again performed at 35°C in 5% CO2.
All slides made for Gram-stain were examined for cells and bacteria using a high-magnification oil immersion objective. Any polymorphonuclear leukocytes and mononuclear cells were reported, and all organisms seen were reported and quantified numerically. The incubated cultures (both agar plates and broth) were examined at 24 h. If there was no growth on plates or in broth, they were incubated for an additional 24 h. After day 2, if no growth was seen in broth or plates, the plates were discarded and reported as “no growth day 2” and the THIO tubes were placed in the incubator for an additional 3 days. The THIO tubes were examined every 24 h until 5 days, and if no growth was found “no growth day 5” was reported.
If growth was seen on plates after the first 24 h, then the sample was re-incubated on plates and in broth for an additional 24 h. All significant isolates were reported on day 2, and any relevant plates were saved until day 5. If there was no growth on the plates, but growth in the THIO tube, the THIO culture was Gram-stained and subcultured on appropriate plates based upon the findings. All plates inoculated from the THIO tubes were incubated and analyzed daily for 5 days and then disposed.
PCR/electrospray ionization mass spectrometry
The PCR/ESI-MS method is a pan-domain MDx that provides species-level identification for the vast majority of eubacteria and some pathogenic fungal taxa. It is based on the principle that despite the great genomic diversity within the domains of life surveyed (eubacteria and fungi) that there are shared sets of common genes at various taxonomic levels, which when evaluated in combination, each at the allelic level, that collectively provide sufficient sequence compositional information for both the detection and speciation of essentially all microorganisms present in a specimen (Ecker et al, 2008; Jacovides et al, 2012; Tuttle et al, 2011). The method employs both very broad-range primers that are designed to amplify a product from an entire domain of microbial life (i.e., all eubacteria), whereas more specific primers are also included to identify genera and species for major pathogenic groups, as well as genes that determine several of the major antibiotic resistances.
Most samples produce a mixture of products, reflecting the diversity of the original mixture of organisms present in the starting sample. DNA extraction of the tissue removed from and adjacent to the implants after excision was performed as described (Ehrlich et al, 2014; Jacovides et al, 2012; Palmer et al, 2014, 2016; Stoodley et al, 2011). In brief, the tissue sample was lysed, homogenized, and the nucleic acids extracted using a commercial DNA extraction kit (Cat. No. 69506; Qiagen). For microbial detection, 10 μL of the isolated nucleic acid sample was loaded per well onto the bacteria, antibiotic resistance, and candida (BAC) detection PCR plate (No. PN 05N13-01; Abbott Molecular, Des Plains, IL).
The BAC detection plate is a 96-well plate in which each well contains 16 primer pairs that collectively survey all bacterial organisms by using a combination of omnipresent loci (e.g., 16S rRNA gene sequence) as well as more taxonomically constrained primers targeting specific groups (e.g., the Staphylococcus-specific tufB gene). The plate also includes primers for the detection of common fungal pathogens and some antibiotic resistance markers (e.g., mecA, vanA, vanB, and KPC).
An internal calibrant composed of a synthetic DNA template was also included in each assay, controlling for false negatives (e.g., from PCR inhibitors). PCR amplification was carried out according to the manufacturer's recommendations and the products were desalted in a 96-well plate and sequentially analyzed using ESI-MS. The spectral signals were processed to determine the identities of the pathogens and their relative concentrations within the processed tissue (Boase et al, 2013; Ecker et al, 2008; Ehrlich et al, 2014; Ho et al, 2003; Jacovides et al, 2012; Palmer et al, 2014, 2016).
FISH and confocal laser scanning microscopy
The fixed specimens were then permeabilized to provide for improved uptake of the FISH probe by Gram-positive bacteria. This was accomplished by treating the explanted tissues with 0.5 mg/mL lysozyme (Sigma-Aldrich, St Louis, MO) in 0.1 M Tris-HCl (Sigma-Aldrich) at pH 8.0 and 0.05 M Na2EDTA (Sigma-Aldrich) for 3 h at 37°C followed by washes (3 × ) with ultrapure water. The samples were then dehydrated in a graded series of ethanol washes (50%, 80%, and 100%) for 3 min at each concentration.
FISH was performed as described previously (Capoor et al, 2016; Ho et al, 2003; Nistico et al, 2009; Palmer et al, 2014, 2016; Poppert et al, 2010; Stoodley et al, 2011) with species-specific or genus-specific fluorescent 16S and 23s rRNA probes (Integrated DNA Technologies, Inc., Coralville, IA): Streptococcus sp. (5′-CAC TCT CCC CTT CTG CAC-3′) (Trebesius et al, 2008); Staphylococcus aureus (5′-GAA GCA AGC TTC TCG TCC G-3′) (Borriello et al, 2004); Staphylococcus sp. (5′-TCC TCC ATA TCT CTG CGC-3′) (Kempf et al, 2000); and Cutibacterium acnes (5′-GCC CCA AGA TTA CAC TTC CG-3′) (Capoor et al, 2016) conjugated with the sulfoindocyanine dyes—Cy3 or Cy5.
Each tissue was incubated with probe-specific formamide and salt concentrations (based on the TM) and then immersed in washing buffer with the probe-specific salt concentrations. Samples were rinsed in sterile MilliQ water before confocal laser scanning microscopy (CLSM). After staining, tissues were mounted in a 35-mm petri plate and imaged with a Leica DM RXE microscope attached to a TCS SP2 AOBS confocal system (Leica Microsystems, Exton, PA) using a 63 × water immersion lens (NA 1.2). Images were collected and analyzed by using the Leica LCS by an observer who was blinded to the diagnostic group to which the sample belonged.
Results
Fifteen patients presented for surgical revision after spinal implantation: four (29%) for clinical suspicion of infection, six (43%) for adjacent segment disease (ASD) alone, one (7%) with ASD and pseudoarthrosis (PA), three (21%) with only PA, and one (7%) for pain. A specimen from one of the participants with ASD was contaminated and thus was excluded from the results.
All four of the participants who presented with clinical signs of infections were confirmed to have bacterial infections through both the PCR/ESI-MS and standard culture techniques (Table 1). The positive predictive value of the PCR/ESI-MS compared with clinical presentation (infection) was 100%. The positive predictive value of the PCR/ESI-MS compared with culture was also 100%. Five of the patients who did not present with clinical signs of infection were found to have evidence of infections by the DNA-based techniques (Table 1).
Fluorescent In Situ Hybridization, Polymerase Chain Reaction Electrospray Ionization-Mass Spectrometry, and Culture Swab Results
ESI-MS, electrospray ionization-mass spectrometry; FISH, fluorescent in situ hybridization; PCR, polymerase chain reaction.
One of these samples was confirmed with both PCR and FISH/CLSM techniques; (Fig. 1) with the remainder being confirmed through the PCR/ESI-MS. The remaining five participants who did not have clinical signs of infections were confirmed to be negative for infections by the MDx, as well as by traditional culture (Table 1). The negative predictive value for PCR/ESI-MS compared with clinical presentation (no infection) was 50%. The negative predictive value for PCR/ESI-MS compared with culture swabs was also 50%.
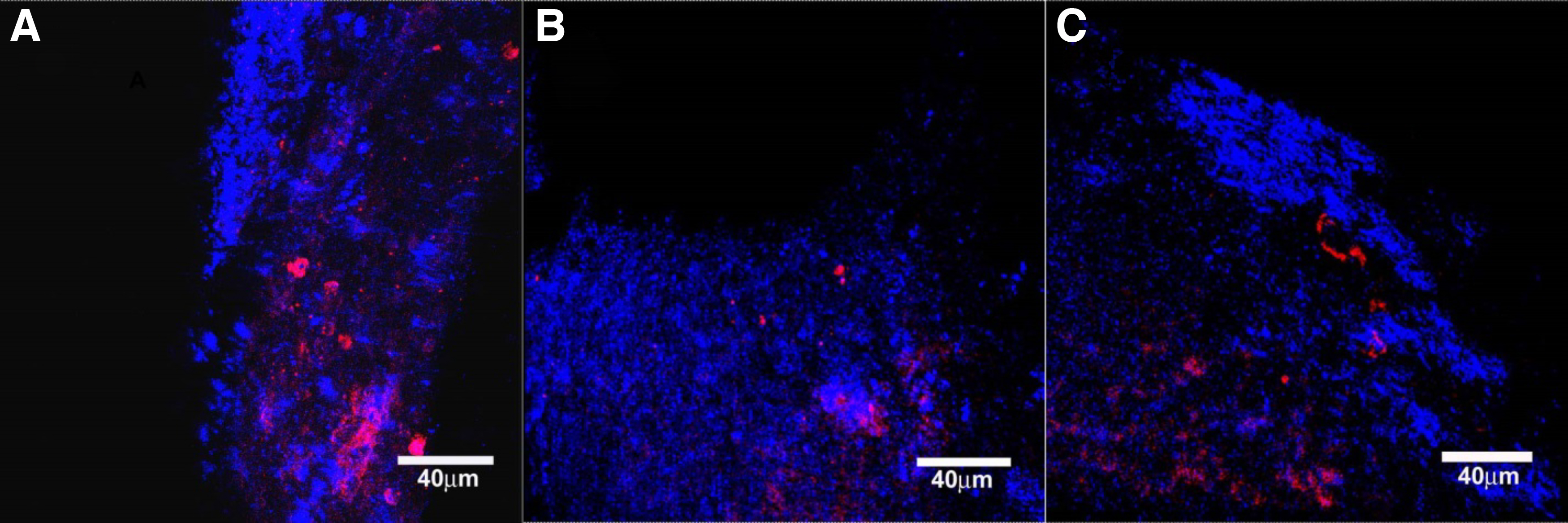
Fluorescent in situ hybridization of explant material. Blue is reflected light from the sample. Pink/red are bacteria-specific signals in single cells and clusters stained with species/genus-specific fluorescent probes.
Discussion
We confirmed the presence of bacteria in all implants from patients with clinical signs of infection with PCR and/or FISH technology. Interestingly, only those specimens that were removed due to clinical infection grew bacteria through traditional culture mediums, and none of the spinal instrumentation removed due to other reasons were culture-positive through traditional methods. Five of these culture-negative specimens revealed the presence of bacteria with the molecular methods.
In essence, 50% of specimens presumed to be sterile showed the presence of bacterial biofilms. Of the four (noninfected) revisions performed for lucency/PA, two were verified to harbor biofilms, yet none of the four evidenced infection through traditional culture media-based methods. In addition, the instrumentation removed due to debilitating pain was shown to harbor biofilm bacteria yet did not support culture. These findings raise the question of whether biofilms contribute to PA and/or back pain after arthrodesis as was seen previously with discitis (Capoor et al, 2016).
Bacterial growth on spinal implants may be routinely missed without the application of appropriate methods for the detection of biofilm bacteria and other slow-growing nonpyogenic bacteria such as C. acnes as we demonstrate in this study. C. acnes have recently been associated with a large number of orthopedic infections, including bony nonunions, intervertebral disc spaces after microdiscectomy, and nonseptic arthritis (Capoor et al, 2016; Ehrlich et al, 2014; Palmer et al, 2014, 2016; Piazza et al, 2017). Detection of biofilm bacteria in clinical settings is limited by the use of current hospital-based cultural techniques; thus, there is a need for updated standardized measures that include MDx (Ehrlich, 1996; Palmer et al, 2014, 2016, 2022; Stoodley et al, 2011; Wolcott and Ehrlich, 2008; Wolcott et al, 2008; Zimmerli, 2014).
Our analysis, designed to look for biofilm presence on spinal implants was prompted by the increasing orthopedic literature on this topic for other types of implants that had demonstrated that implanted devices in regions other than the spine were often infected with biofilm bacteria (Ehrlich et al, 2014; Jacovides et al, 2012; Palmer et al, 2014, 2022; Stoodley et al, 2005, 2011). The near ubiquitous persistence of bacterial biofilms calls for a review of the extant sterilization protocols and techniques.
In this study, samples were taken from human subjects during spine instrumentation revision surgery, regardless of indication for revision, to determine bacterial presence on the implants. Through FISH and PCR/ESI-MS procedures, nine (60%) of the implants were found to have evidence of bacteria. This figure includes all participants with a clinically recognized infection and half of those without.
The sample size is the main limitation of this study. With only 14 samples taken from a single institution, it is difficult to generalize the results or draw statistically significant conclusions from the data. The results do warrant the need for future larger multicenter studies that can address these limitations. Consistent results will lead to studies focusing on improving the methods of detection and sterilization techniques.
Clinical implications
Back pain is a major cause of morbidity in postoperative spinal fusion patients, and this investigation begets the question of whether indolent bacterial biofilms may contribute to this epidemic (AlAujan et al, 2016; Chan and Peng, 2011; Kamper et al, 2014). As demonstrated in the one case of revision for back pain, nonpyogenic bacteria that have been shown to infect postoperative disc spaces may theoretically result in pain, which is otherwise known as discogenic back pain. In addition to back pain as a possible consequence of indolent bacteria on “healed” spinal instrumentation, PA as a result of biofilms may contribute to back pain otherwise presumed to be due to “non-fusion” due to other reasons.
Currently, trays containing implants are sterilized in bulk. In other words, any given tray containing screws, rods, and other implantable materials may be removed from the tray itself, trialed, and reinserted into the tray. These trays are then taken to be sterilized in an autoclave in bulk, often without first undergoing mechanical debridement of dried blood and tissue, which cannot be seen by the naked eye. Perhaps such implants should be subjected to physically removing any visible blood or other body products with a scrub or acid wash procedure before being heated for sterilization purposes.
Finally, titanium is considered to be a friendly material for implantation for bony fusions. Multiple previous trials have demonstrated the “superior” results of titanium when compared with other materials such as steel, carbon, polyether ether ketone, and other alloys (Ali et al, 1990; Hinüber et al, 2010; Yang et al, 2014). Titanium is used due to its ability to hinder fibrous reactions from forming on its outer layer of constructs and is considered more bioinert than other materials in situ. Titanium has been shown to allow better proliferation of osteoblasts than other alloys, leading many to consider titanium the most biofriendly (to the native bone host) option when fusion is considered the end goal.
Perhaps such biocompatible materials are also friendly to other biological organisms, such as bacteria. Titanium is not considered to be osteoconductive or osteoinductive, but it does allow for decreased fibrous reactions, and allows for the proliferation of necessary host cells. This process of osteointegration has heretofore not been described in the field of spine surgery, and the authors propose the rethinking and analysis of such materials in the human body and their reactivity to host tissue and how that compares with the reactivity they have to bacterial biofilms.
Identification of shortcomings in current protocols will facilitate a change in clinical methodology. This would significantly improve the postoperative outcomes for patients who undergo implantation surgery by the way of reducing the need for revision surgeries due to infection, and particularly for PA. The typical surgical treatments for infection can lead to large accumulated costs for both the hospital system and the patient (Adogwa et al, 2015; Palmer et al, 2014; Piazza et al, 2017).
This study supports the need for preventative and therapeutic measures aimed specifically at biofilm-caused infections. We have little doubt that the bacteria reported were actually present as our PCR facilities are rigorously designed and operated to prevent molecular carryover of amplimers that can lead to false positives, and the CLSM-FISH results corroborate the presence of bacteria. However, we recognize that this was a pilot study and as such further larger-scale studies are needed that not only examine a larger specimen set but also critically examine whether the presence of bacteria in the absence of clinical suspicion contributes to the pathology.
Footnotes
Authors' Contributions
Conceptualization, data curation, investigation, visualization, and writing/editing by D.A.D. Conceptualization, funding acquisition, project administration, resources, supervision, and writing/editing by B.C. Data curation, investigation, methodology, validation, visualization, and writing/editing by R.K. and L.N. Conceptualization, funding acquisition, methodology, project administration, resources, supervision, and writing/editing by G.D.E. Data curation, investigation, and writing/editing by S.A. Conceptualization, project administration, resources, supervision, and writing/editing by D.T.A.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.