
Abstract
Aims:
In this study, we determined whether different genotypes of drug-metabolizing enzymes are associated with the therapeutic effects of gefitinib in non-small cell lung cancer (NSCLC).
Methods:
A retrospective analysis of 112 patients with stage III or IV NSCLC was performed. The clinical characteristics of these patients, including progression-free survival (PFS), outcome of gefitinib treatment, and relationship between the genotypes of rs1065852/rs2242480 and prognosis, were analyzed.
Results:
The rs1065852 CT/TT genotype was associated with worse prognosis than the CC type (p = 0.0306), and the median PFS was lower than that with the CC type (287 days vs. 350 days). Compared with those with CC+CC genotypes, individuals carrying T alleles (CT/TT+CT/TT) at rs1065852/rs2242480 had a poorer prognosis, and the median PFS of CT/TT+CT/TT at rs1065852/rs2242480 was significantly lower than that of the CC+CC type (188 days vs. 444.5 days).
Conclusions:
Genotypes of the drug-metabolizing enzymes rs1065852 and rs2242480 have an impact on the prognosis of patients with NSCLC treated with gefitinib.
Introduction
Lung cancer is one of the most frequently diagnosed cancers and is the leading cause of cancer-related deaths worldwide (Siegel et al, 2022). Non-small cell lung cancer (NSCLC) is the primary subtype of lung cancer, accounting for ∼85% of cases (Allemani et al, 2018). For patients with NSCLC with epidermal growth factor receptor (EGFR) gene mutations, the emergence of small-molecule targeted drugs has led to significant advances in NSCLC treatment (Gridelli et al, 2011). As a first-generation EGFR tyrosine kinase inhibit (TKI) drug (Douillard et al, 2014), gefitinib can exert an inhibitory effect on tumor growth and inhibit tumor metastasis and angiogenesis. Therefore, Gefitinib as a first-generation EGFR-TKI can also promote apoptosis of tumor cells and has some antitumor efficacy. Oral administration of gefitinib displays different pharmacokinetics in different patients (Swaisland et al, 2005), which may be attributed to drug metabolism.
Previous studies have shown that members of the P450 enzyme family can metabolize gefitinib. The main metabolizing enzymes of the P450 enzyme family include CYP3A4, CYP2D6, and CYP1A1 (Zhao et al, 2017). CYP3A4 extensively metabolizes gefitinib, and increasing evidence has shown that polymorphisms in the CYP3A4 gene have functional significance (Kumondai et al, 2021; Werk and Cascorbi, 2014). CYP3A4*1G (rs2242480) is the most common single nucleotide polymorphism (SNP) of CYP3A4 in the Chinese population, with a mutant allele occurring in 24.01% of the population (Hu et al, 2017).
Furthermore, another major metabolic enzyme for gefitinib is CYP2D6. CYP2D6*10 (rs1065852) is the most common genotype in the Asian population, with a variant allele frequency of 52.6% in the Chinese population (Kurose et al, 2012). The SNPs of the two drug-metabolizing enzymes are related to drug metabolism activity (Chen et al, 2018; McGraw et al, 2012; Regan et al, 2012). However, there are few studies on the correlation between the drug metabolism function of gefitinib and prognosis of disease.
This retrospective study reviewed the clinical features of 112 patients with advanced NSCLC with EGFR mutations who did not receive other treatments before gefitinib and analyzed the polymorphism sites of drug-metabolizing enzymes to explore whether different genotypes of CYP2D6 (rs1065852) and CYP3A4 (rs2242480) impact the clinical effect of gefitinib treatment.
Materials and Methods
Study population
A retrospective analysis of patients with lung adenocarcinoma who only harbored EGFR mutations and did not receive other treatments before targeted therapy at Henan Cancer Hospital from January 1, 2017, to March 10, 2021, was performed; clinical information of these patients, including EGFR mutation status, laboratory data, treatment information, and treatment response, was retrieved from their medical records. All patients received first-line treatment with gefitinib until disease progression, or March 10, 2021. The median follow-up period for the study subjects was 10 months (1-48 months). Next-generation sequencing (NGS) clarified the status of CYP2D6 (rs1065852). Sanger sequencing was performed on the remaining samples to determine the status of the CYP3A4 (rs2242480) and CYP2D6 (rs1065852) polymorphic loci.
Identification of biallelic polymorphisms
Gene mutation of EGFR in the tumor tissues of patients was detected using NGS. In addition, the genetic profiles of the tissue samples were assessed with capture-based targeted deep sequencing using a gene panel (Burning Rock Biotech Ltd., Guangzhou, China), covering 76 kb of the human genome. In addition, all indexed samples were sequenced using NextSeq 500 (Illumina, Inc., USA) with paired-end reads (Tian et al, 2020; Zhang et al, 2019).
CYP2D6 and CYP3A4 gene mutations were screened using NGS or Sanger sequencing. The forward primer of CYP3A4 (rs2242480) was 5′-CTGGCTATGAAACCACGAGC-3′, and the reverse primer was 5′-TCTGCCAGTAGCAACCATTTG-3′. The forward primer of CYP2D6 (rs1065852) was 5′-GCAGGTATGGGGCTAGAAGC-3′, and the reverse primer was 5′-TGTTTGCTTCTGGTAGGGGAG-3′. Classification of the variants was performed by two clinical geneticists independently.
Statistical analysis
All statistical analyses were performed using GraphPad Prism 5 and IBM SPSS Statistics 25. Univariate analyses were performed with the log-rank test. A COX proportional-hazard model was used to compare the different clinical characteristics, including sex, age, smoking history, drinking history, EGFR mutation status, and CYP3A4 (rs2242480) and CYP2D6 (rs1065852) polymorphic loci, and multivariate COX regression was used to determine independent prognostic factors. The Kaplan-Meier method was used to estimate survival and compared it using the log-rank test. Statistical significance was set at p < 0.05.
Results
Patient characteristics and drug metabolizing enzyme genotype information
This study included 112 patients with lung adenocarcinomas with EGFR mutations. The participants included 42 men and 70 women. According to the tumor node metastasis (TNM) NSCLC staging system (Tsim et al, 2010), 12 and 100 patients were identified as having stages III and IV, respectively. The participants also included 57 (50.9%), 50 (44.6%), and 5 (4.5%) patients with EGFR-19del, L858R mutation, and other sensitive mutations. The clinical characteristics of 112 patients were analyzed using univariate analysis. The mentioned clinical data did not affect the survival of patients with lung adenocarcinoma treated with gefitinib (all p values >0.05) (Table 1).
Clinical Characteristics of 112 Patients
CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; EGFR, epidermal growth factor receptor; PFS, progression-free survival; TNM, tumor node metastasis.
The 112 patients showed that 35 (31.3%) patients had the CYP2D6 (rs1065852) CC genotype; 30 (26.8%), TT genotype; and 47 (41.9%), CT genotype (Table 2; Fig. 1). Sanger sequencing was performed on 62 of these patients (Fig. 1)—twenty-three (37.1%) with the CYP3A4 (rs2242480) CC genotype; 3 (4.8%), TT genotype; and 36 (58.1%), CT genotype (Table 2; Fig. 1).
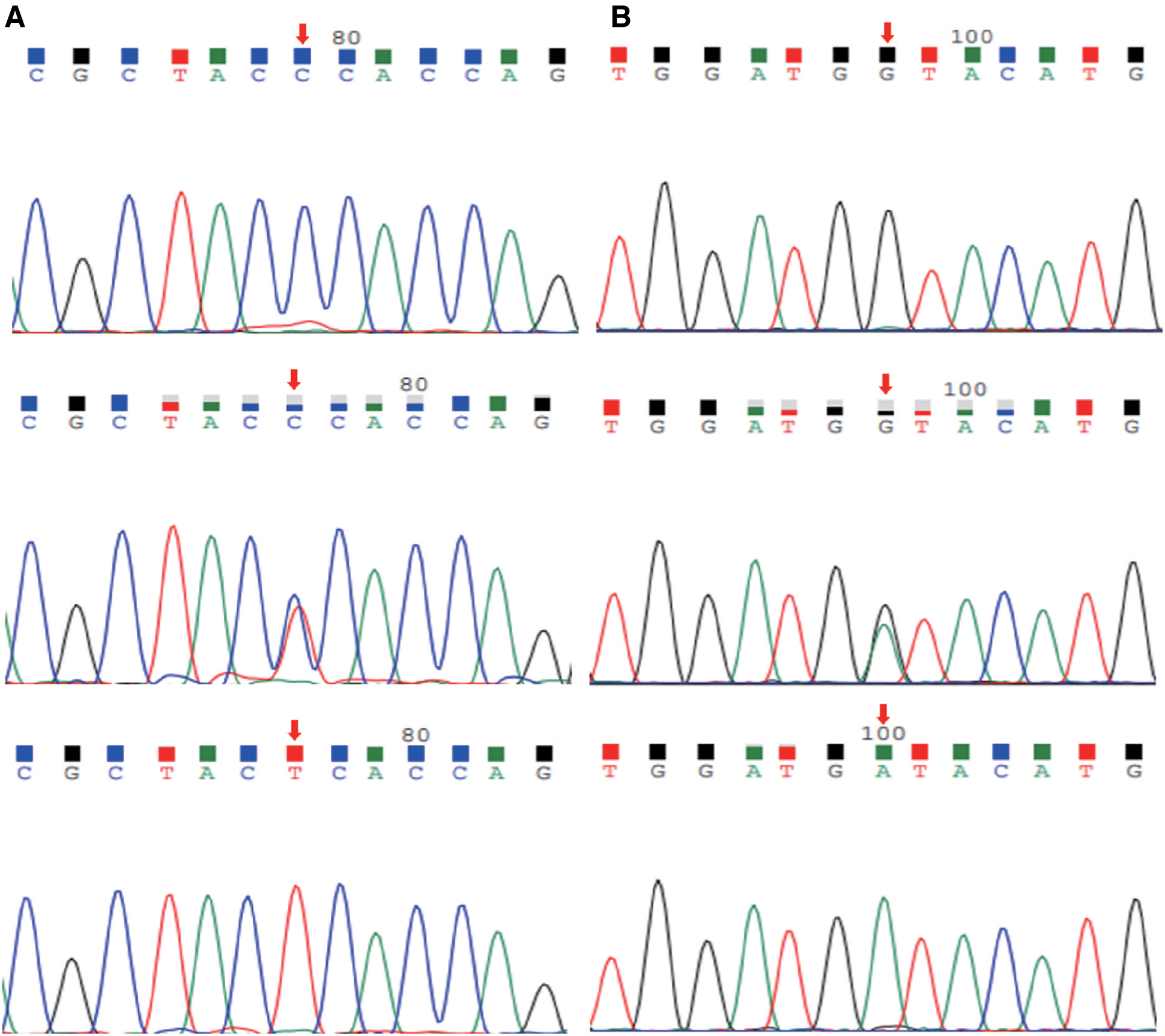
Sanger sequencing:
Distribution of CYP2D6 (rs1065852) and CYP3A4 (rs2242480)
Groups
The genotypes of 62 patients were classified as CYP2D6 (rs1065852) and CYP3A4 (rs2242480), which were categorized into CYP2D6 CC+CYP3A4 CC, CYP2D6 CC+CYP3A4 CT/TT, CYP2D6 CT/TT+CYP3A4 CC, and CYP2D6 CT/TT+CYP3A4 CT/TT (Table 3).
Groups of CYP2D6 (rs1065852) and CYP3A4 (rs2242480)
2D6, CYP2D6 (rs1065852); 3A4, CYP3A4 (rs2242480).
Multivariable Cox regression for potential compounding factors
Multivariable Cox regression analysis was performed to adjust for potential confounding factors. Relative to that for the 112 patients with the CYP2D6 (rs1065852) CC genotype, the hazard ratio (HR) for tumors with the CYP2D6 (rs1065852) CT/TT genotype was 1.613 (p = 0.046, 95% confidence interval [CI]: 1.009-2.578); the results are reflected in Figure 2A. Data on the independent variables included in the multifactor regression model are presented in Supplementary Table S1. A decrease in CYP2D6 enzyme metabolism was found to be correlated with inferior outcomes in patients with NSCLC and is determined to be independent of other clinicopathological covariates.
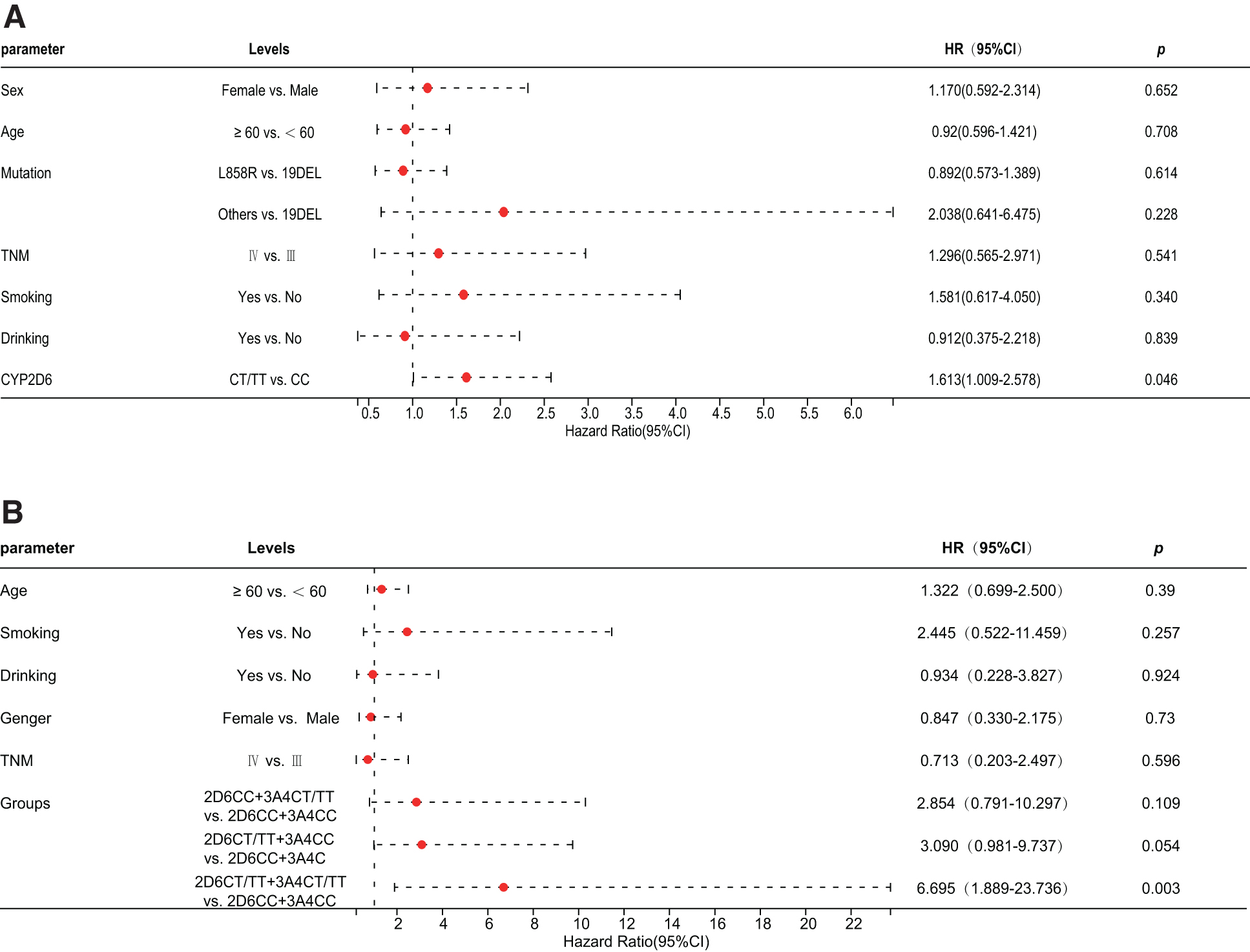
Result of COX's multivariable analysis is shown as forest plots and as Cox regression analysis for the 112 patients. CYP2D6 was identified as an independent prognostic factor.
Among the 62 patients, the HR for CYP2D6CT/TT+CYP3A4CT/TT was 6.695 (p = 0.003, 95% CI: 1.889-23.736) (Fig. 2B). COX's multivariate analysis presented in a forest plot (Fig. 2B) showed that compared with the CYP2D6CC+CYP3A4CC group, the CYP2D6CT/TT+CYP3A4CT/TT group was a risk factor and had worse prognosis. The included independent variables were age, history of smoking, history of alcohol consumption, sex, TNM stage, and drug-metabolizing enzyme groups (Supplementary Table S2).
Impact of the CYP2D6 and CYP3A4 enzyme genotype subtypes on the prognosis of the disease
Among the CYP2D6 (rs1065852) genotypes, CT/TT was found to have worse prognosis than the CC type, and the median progression-free survival (PFS) was lower than that with the CC type (287 days vs. 350 days) (p = 0.0306) (Fig. 3A). CYP3A4 (rs2242480) showed no significant difference in PFS between CC and CT/TT types (p = 0.1346) (Fig. 3B).
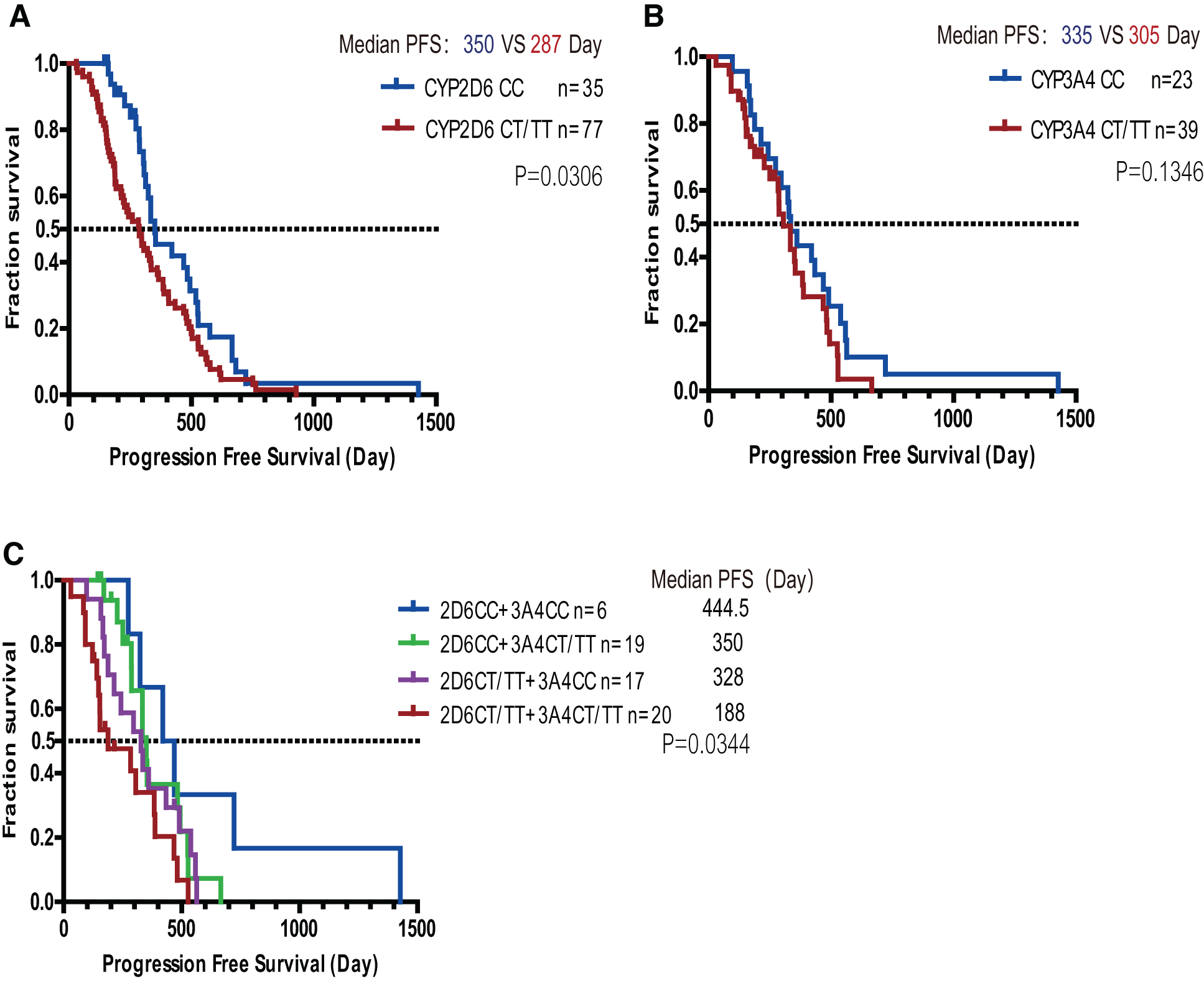
PFS analysis. Kaplan-Meier plot shows comparison of PFS in CYP2D6 (rs1065852)
Effects of different drug-metabolizing enzyme isotypes on treatment outcomes
In the CYP2D6CC+CYP3A4CC, CYP2D6CC+CYP3A4CT/TT, CYP2D6CT/TT+CYP3A4CC, and CYP2D6CT/TT+CYP3A4CT/TT groups, there was a significant trend of difference in PFS among the four groups (p = 0.0344) (Fig. 3C), indicating that the polymorphism of drug-metabolizing enzyme genotypes has a specific impact on prognosis.
In the CYP2D6 (rs1065852) and CYP3A4 (rs2242480) genotype groups (Table 3), the prognosis of the CYP2D6CT/TT+CYP3A4CT/TT group was poorer than that of the CYP2D6CC+CYP3A4CC group (Fig. 2B, p = 0.003, HR = 6.695) and the median PFS was lower than that in the CYP2D6CC+CYP3A4CC group (188 days vs. 444.5 days). Patients carrying T alleles (CC+CT/TT) at rs1065852/rs2242480 tended to have poorer PFS than those with the CC+CC type (Fig. 3C).
Discussion
Gefitinib is an inhibitor of the tyrosine kinase domain of EGFR and is used to treat patients with locally advanced or metastatic NSCLC. Although the main resistance mechanisms are secondary EGFR mutations, it is undeniable that drug-metabolizing enzymes can affect therapeutic outcomes. Here, we explored the relationship between drug-metabolizing enzyme activity and treatment effect to guide patients with advanced lung cancer to obtain more efficient treatment.
Gefitinib is mainly metabolized by CYP3A4, whereas O-desmethyl-gefitinib (M523595) is metabolized by CYP2D6 (Li et al, 2007; Swaisland et al, 2006). It is the main metabolite observed in human plasma. Several studies have reported that genotype polymorphisms can affect the activity of drug-metabolizing enzymes and that differences in drug metabolism can lead to severe toxicity or treatment failure (Linder et al, 1997).
Previous studies have shown that CT or TT in CYP2D6 (rs1065852) and CT or TT in CYP3A4 (rs2242480) are associated with a decreased function (Chi et al, 2015; Lu et al, 2021). Changes in the activity of drug-metabolizing enzymes are caused by genetic variations (polymorphisms), and genotypes with reduced function lead to decreased clearance of drugs from the body, which may impact prognosis. Luo et al. (2021) reported that patients with loss of CYP2D6 genotype expression have a poor prognosis. After the initiation of gefitinib therapy, the slow-metabolizing type of drug-metabolizing enzymes had a significantly poor response to gefitinib treatment, and patients with NSCLC with the CYP2D6 T alleles (CT/TT) of the drug-metabolizing enzyme had decreased metabolic enzyme activity, leading to increased resistance to gefitinib when compared with that with type CC (Fig. 3A).
Decreased function of drug-metabolizing enzymes can lead to high blood levels of gefitinib in the body, which may impact prognosis. In fact, studies have reported that compared with low blood concentration, high blood concentration of gefitinib does not correlate with a good prognosis (median PFS 9 months vs. 11 months). Conversely, a high blood concentration may lead to poorer prognoses. (Hirose et al, 2016). Some studies have shown no significant difference in PFS between patients receiving low-dose gefitinib and those receiving standard gefitinib doses of 250 mg/day (Satoh et al, 2011; Sim et al, 2014). Yokota et al. (2020) reported that gefitinib plasma trough concentrations (C0) between 200 and 400 ng/mL tended to have longer PFS than C0 ≥ 400 ng/mL.
In addition, drug-metabolizing enzymes that show poor metabolism have no clinical benefit and are even associated with poor prognosis. We further categorized the patients as having slow metabolizers CT/TT and normal metabolizers CC. We found that compared with those with the CC+CC genotype, individuals with T alleles (CT/TT+CT/TT) at rs1065852/rs2242480 had poorer prognoses (Figs. 2B and 3C). The median PFS of rs1065852/rs2242480 CT/TT+CT/TT was lower than that of the CC+CC type (188 days vs. 444.5 days), which is consistent with previous findings (Fig. 3C).
In the case of low-metabolizing drug-metabolizing enzymes, the clearance rate of gefitinib was reduced, and the prognosis was poor, which may increase gefitinib exposure leading to toxicity (Suzumura et al, 2012). In the 150-1,000-mg phase I clinical trial of gefitinib, no relationship was observed between changes in plasma concentrations of gefitinib and antitumor response after reaching the treatment response. However, the plasma concentration was related to its toxicity (Baselga et al, 2002). Therefore, a potential increase in gefitinib exposure leading to toxicity may have adverse effects on the prognosis, but the mechanisms leading to its poor prognosis remain to be further explored.
With the development of second- and third-generation EGFR-TKIs, the PFS of patients with NSCLC receiving targeted therapy is prolonged, and the impact of drug-metabolizing enzymes on prognosis deserves further attention. By determining the genotype of the patient's drug-metabolizing enzymes before treatment, the patient's treatment can be stratified, making the clinical treatment more precise. The CYP3A4 (rs2242480) C > T and CYP2D6 (rs1065852) C > T polymorphisms can predict the clinical results of gefitinib treatment. They may guide clinical treatment, implying that the genotype of drug-metabolizing enzymes can be used to predict the efficacy of gefitinib.
Conclusions
Our study shows that patients with rs1065852 (CYP2D6) and rs2242480 (CYP3A4) lung adenocarcinomas with T alleles have worse prognosis than those with the CC type. However, these finding influences clinical treatment and can be used as a potential prognostic marker for targeted therapies.
Footnotes
Authors' Contributions
R.F.: Conceptualization (equal), writing—original draft (lead), writing—review and editing (equal), and formal analysis (equal). J.Z.: Conceptualization (equal), writing—original draft (equal), writing—review and editing (equal), and formal analysis (equal). B.W.: writing—review and editing (equal). X.L., Y.G., and L.Z.: data curation (equal). P.R. and R.S.: Software (equal). Y.G.: Project administration (lead) and funding acquisition (lead).
Ethical Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Henan Cancer Hospital, and all participants signed a written informed consent. The ethical review number is 2021-KY-0092-001.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially supported by funding from the Major Public Welfare Projects in Henan Province (Grant No.: 201300310400) and the Funding Program for Medical Sciences and Technologies of Henan Province (Grant No.: LHGJ20190672).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.